Author: Dr Val Phua
Estimated reading time: 16 minutes
Implantable Collamer Lens surgery, commonly known as ICL surgery, can correct short-sightedness and astigmatism by placing a specially designed lens inside the eye.
The ICL is positioned behind the iris and in front of the eye’s natural crystalline lens. Unlike LASIK, PRK or SMILE, ICL surgery does not remove central corneal tissue to correct the prescription.
ICL surgery is often associated with high myopia, but it is not limited to patients with extremely high prescriptions. Modern central-port ICLs have also produced effective and predictable results in appropriately selected patients with low-to-moderate myopia.
However, having myopia does not automatically make someone suitable for ICL surgery.
A suitable patient generally needs:
- A reasonably stable spectacle prescription
- Adequate space inside the front of the eye
- Healthy corneal endothelial cells
- A clear natural lens
- Acceptable eye pressure and drainage angles
- No active eye disease that would make surgery unsafe
- Realistic expectations about vision and long-term follow-up
The decision requires a comprehensive examination of the cornea, anterior chamber, natural lens, optic nerve and retina. It cannot be made from the spectacle prescription alone.
What Is ICL Surgery?
ICL stands for Implantable Collamer Lens.
It is a type of phakic intraocular lens:
- Phakic means that the natural lens remains inside the eye.
- Intraocular means that the corrective lens is implanted within the eye.
- Collamer refers to the collagen-containing polymer from which the lens is made.
The ICL is inserted through a small corneal incision and positioned in the posterior chamber, behind the iris and in front of the natural lens.
Modern EVO ICL models contain a small central opening that allows the eye’s natural aqueous fluid to circulate through the lens. Unlike older ICL designs without a central port, EVO ICL implantation generally does not require a preoperative peripheral iridotomy.
Is ICL Only Suitable for High Myopia?
No.
ICL surgery was traditionally considered mainly for moderate, high or very high myopia, especially when laser vision correction would require excessive corneal tissue removal.
However, research has shown good outcomes in both lower and higher myopic prescriptions.
A multicentre study of 351 eyes found that central-port ICL implantation provided similar safety, efficacy, predictability and stability in eyes with low-to-moderate myopia and eyes with high myopia during the first postoperative year. Approximately 98% to 99% of eyes in the two groups were within 1.00 dioptre of the intended correction.
A separate study also reported satisfactory outcomes in low- and high-myopia groups while emphasising the importance of careful sizing, particularly in older patients and those with shallower anterior chambers.
ICL may therefore be considered across a broader range of myopia when the patient’s anatomy and overall risk profile are suitable.
The fact that ICL can correct a lower prescription does not necessarily mean that intraocular surgery is preferable to LASIK, SMILE, PRK, glasses or contact lenses. The potential benefit must justify the additional risks and long-term monitoring associated with an implanted lens.
What Prescription Is Suitable for ICL?
The available treatment range depends on:
- The ICL model
- The country’s regulatory approval
- The available lens powers
- The patient’s anatomy
- The surgeon’s clinical judgement
As an example, US FDA labelling for EVO ICL describes treatment of myopia from −3.00 to −15.00 dioptres and reduction of myopia up to −20.00 dioptres. The toric model is approved there for myopia with 1.00 to 4.00 dioptres of astigmatism. Approved ranges may differ in Singapore and other jurisdictions.
A patient whose prescription falls within a technical treatment range may still be unsuitable because of shallow internal anatomy, low endothelial cell density, cataract, glaucoma or another eye condition.
Conversely, a person with a lower prescription may still be considered for ICL when corneal laser surgery is less suitable and the internal eye anatomy is favourable.
Who Is Commonly a Good Candidate for ICL?
A typical suitable candidate may have several of the following characteristics.
Moderate, High or Very High Myopia
ICL is particularly useful for patients with significant myopia.
As the amount of myopia treated with LASIK or SMILE increases, a greater amount of corneal tissue generally needs to be removed. ICL corrects the focusing error without requiring a corresponding amount of central corneal tissue removal.
This can be advantageous when:
- The prescription is high
- Corneal thickness is limited
- The expected laser correction would substantially alter corneal shape
- Preserving corneal tissue is a priority
- Visual quality with a large corneal correction is a concern
Long-term studies of central-port ICLs have reported good refractive stability, visual outcomes and safety in selected patients with moderate-to-high myopia.
Myopia With Astigmatism
A toric ICL can correct regular astigmatism together with myopia.
Suitable patients require:
- Accurate measurement of the astigmatism
- A stable astigmatic prescription
- Astigmatism that falls within the available lens range
- Sufficient internal anatomy for safe implantation
- No major irregular corneal disease limiting visual quality
The toric lens must be placed at the correct axis and remain rotationally stable. Significant postoperative rotation can reduce the astigmatic correction and may require surgical repositioning.
Published studies have generally reported favourable safety, predictability and refractive stability with toric ICL implantation in selected patients.
Thin Corneas
ICL may be suitable when the cornea is too thin for the amount of tissue that would need to be removed during laser vision correction.
This does not mean that every thin cornea should receive an ICL.
A thin cornea may be:
- Naturally thin but otherwise normal
- Associated with keratoconus
- Associated with another corneal disorder
- Previously treated with laser surgery
- Structurally unstable
Corneal topography and tomography are therefore still essential before ICL surgery.
ICL corrects the refractive error but does not strengthen the cornea or treat progressive keratoconus.
Corneas Unsuitable for LASIK or SMILE
ICL may be considered when laser treatment is less suitable because of:
- Insufficient corneal thickness
- A high prescription requiring excessive tissue removal
- Previous corneal laser surgery with inadequate tissue for enhancement
- Certain stable corneal irregularities
- Concern about corneal biomechanical strength
- A lifestyle in which preserving corneal tissue is preferred
However, the underlying reason for abnormal corneal measurements must be understood before proceeding.
Progressive corneal disease remains a contraindication to elective refractive surgery until it has been appropriately assessed and managed.
Stable Keratoconus in Selected Cases
ICL is not a treatment for keratoconus.
Nevertheless, selected patients with stable, non-progressive keratoconus may sometimes receive an ICL to correct residual myopia and astigmatism, particularly after corneal cross-linking.
The patient must understand that:
- ICL does not regularise the corneal shape
- Irregular astigmatism may remain
- Best-corrected vision may still be limited
- Corneal progression must first be excluded
- Contact lenses may still be needed for optimal vision
- Long-term corneal monitoring remains necessary
Reviews and clinical studies suggest that phakic lens implantation can be effective in selected eyes with stable keratoconus, but patient selection is more complex than in eyes with normal corneas.
Significant Dry-Eye Concerns
ICL may be considered for patients with dry-eye risk because it does not involve central corneal laser ablation or the creation of a LASIK flap.
Laser vision correction can temporarily reduce corneal sensation and disrupt feedback mechanisms involved in blinking and tear production. ICL generally produces less central corneal nerve disruption.
However, ICL does not cure dry eye.
Temporary dryness or irritation can still occur because of:
- The small corneal incision
- Surgical antiseptic
- Postoperative medication
- Preservatives in eyedrops
- Reduced blinking
- Pre-existing blepharitis
- Meibomian gland dysfunction
Dry-eye disease and eyelid inflammation should be treated before surgery, regardless of which refractive procedure is chosen.
Contact Lens Intolerance
Patients who can no longer comfortably wear contact lenses may consider ICL surgery.
Contact lens intolerance may result from:
- Dry eye
- Allergy
- Giant papillary conjunctivitis
- Lens deposits
- Poor lens fit
- Recurrent inflammation
- Occupational or lifestyle difficulties
The underlying cause still needs to be identified.
A patient with active giant papillary conjunctivitis, severe allergy or significant eye-surface inflammation should usually be treated before elective ICL surgery.
A Stable Spectacle Prescription
A suitable candidate should generally have a prescription that has remained reasonably stable.
Significant continuing myopia progression may produce a residual prescription after surgery, even when the lens power was calculated correctly.
The definition of stability varies, but surgeons often look for no major change during the preceding year.
Small variations may be acceptable, particularly at very high prescriptions, but a clear pattern of progression should be investigated.
Factors that can cause temporary or continuing prescription changes include:
- Ongoing axial myopia progression
- Pregnancy
- Breastfeeding
- Uncontrolled diabetes
- Certain medications
- Corneal disease
- Changes caused by contact lens wear
- Accommodation or focusing spasm
FDA information states that the safety and effectiveness of EVO ICL have not been established in patients with unstable or worsening myopia.
A Clear Natural Lens
The natural crystalline lens remains inside the eye after ICL surgery.
An ideal candidate should not already have a visually significant cataract.
If cataract is present, implanting an ICL may provide only temporary benefit before the ICL needs to be removed and cataract surgery performed.
Patients approaching the age at which cataract and presbyopia become more relevant require especially careful counselling.
Is There an Ideal Age for ICL Surgery?
Age criteria vary by country and product labelling.
In the United States, EVO ICL is indicated for patients aged 21 to 45 years. The FDA-approved clinical study included patients aged 22 to 45.
Outside the United States, clinical practice and regulatory limits may differ.
Age matters because it influences:
- Prescription stability
- Anterior chamber anatomy
- Endothelial cell reserve
- Natural-lens thickness
- Presbyopia
- Cataract risk
- The expected duration the ICL will remain inside the eye
Patients in Their Twenties
Patients in their twenties may be good candidates when:
- Their prescription is stable
- The internal anatomy is adequate
- The endothelial cell count is healthy
- The natural lens is clear
- They understand that myopia may still progress
- They accept lifelong eye examinations
Very young adults with recently changing prescriptions may benefit from waiting until stability is confirmed.
Patients in Their Thirties
Many patients in their thirties remain suitable candidates.
Important factors include:
- Prescription stability
- Corneal and anterior-chamber anatomy
- Family history of early cataract
- Eye pressure
- Endothelial cell count
- Lifestyle and visual goals
Patients Over 40
ICL may still be considered in selected patients over 40, but age-related issues become increasingly important.
These include:
- Presbyopia
- Early natural-lens opacity
- A thicker natural lens
- Reduced anterior-chamber space
- A shorter interval before cataract surgery may become necessary
- Greater long-term cataract risk
Long-term studies involving earlier ICL models have found that older age and low vault are associated with a higher likelihood of cataract development.
A patient over 40 with a clear natural lens and favourable anatomy may still be suitable. However, if early cataract is already present, cataract surgery or lens-replacement surgery may be more appropriate.
How Does Presbyopia Affect Suitability?
Presbyopia is the age-related loss of the natural lens’s ability to focus at near.
A standard ICL corrects distance myopia but does not prevent presbyopia.
A short-sighted patient may currently be able to read without glasses by removing their distance spectacles. If both eyes are fully corrected for distance with ICL, that unaided near vision may be lost.
Options may include:
- Reading glasses after surgery
- Leaving a small amount of myopia
- Monovision
- Correcting one eye for distance and the other for nearer tasks
- Choosing a different surgical strategy
Monovision is not suitable for everyone because it may affect:
- Depth perception
- Night vision
- Contrast sensitivity
- Fine visual tasks
- Sports performance
A contact lens monovision trial is often helpful before committing to a permanent monovision target.
What Internal Eye Anatomy Is Required?
ICL sits inside the eye, so there must be adequate space for it.
Important measurements include:
- Anterior chamber depth
- Drainage-angle width
- White-to-white corneal diameter
- Sulcus-to-sulcus dimensions
- Anterior chamber volume
- Natural-lens thickness and position
- Crystalline lens rise
- Pupil size
These measurements help determine whether the lens can be implanted safely and which ICL size should be selected.
Anterior Chamber Depth
Anterior chamber depth refers to the space between the cornea and the natural lens.
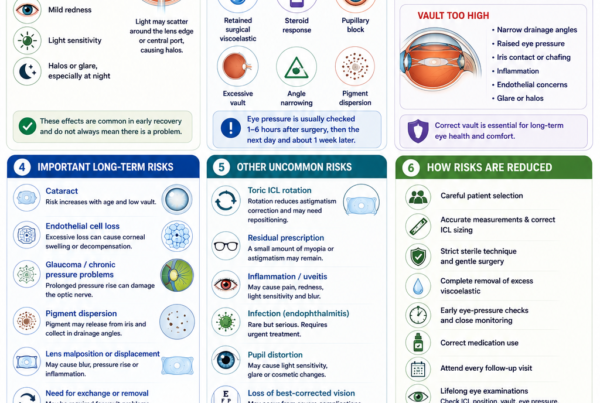
If the chamber is too shallow, an ICL may crowd the front of the eye and increase the risk of:
- Narrow drainage angles
- Raised eye pressure
- Iris contact
- Pigment dispersion
- Endothelial damage
- Unsuitable vault
US FDA labelling contraindicates EVO ICL when the true anterior chamber depth is below 3.0 mm. It also requires an adequately open anterior chamber angle. These values are regulatory criteria for a particular market and should not be treated as the only measurements considered in clinical practice.
Drainage-Angle Anatomy
The drainage angle is where fluid leaves the front of the eye.
An ICL may reduce the available space within this region. Patients with narrow or abnormal drainage angles may be at increased risk of raised pressure or angle closure.
Gonioscopy or anterior-segment imaging may be used to assess the angle.
FDA information advises against implantation when the angle is below Grade III on gonioscopy under its approved criteria.
Lens Sizing and Vault
The ICL must be the correct physical size for the eye.
After implantation, the lens should sit with an appropriate vault, which is the space between the back of the ICL and the front of the natural lens.
A very low vault may increase concern about:
- Contact or proximity to the natural lens
- Anterior subcapsular cataract
- Reduced fluid circulation
A very high vault may contribute to:
- Narrow drainage angles
- Increased eye pressure
- Iris contact
- Pigment dispersion
- Inflammation
- Optical symptoms
Vault is influenced by multiple factors, including anterior chamber depth, internal eye diameter, ICL size, natural-lens anatomy and age.
Modern imaging and sizing formulas improve planning, but postoperative vault cannot be predicted perfectly.
Why Is the Endothelial Cell Count Important?
The corneal endothelium is a single layer of cells lining the inner surface of the cornea.
These cells pump fluid out of the cornea and help keep it clear.
Human endothelial cells have limited ability to regenerate. Their number naturally decreases with age and may also be affected by intraocular surgery.
A patient needs an adequate endothelial cell reserve before ICL surgery.
The minimum acceptable count depends on:
- Age
- Anterior chamber depth
- The applicable regulatory criteria
- Existing corneal health
- The surgeon’s judgement
- The expected number of years the lens will remain in the eye
FDA labelling provides age- and anterior-chamber-depth-specific minimum endothelial cell densities for EVO ICL.
Patients with an inadequate endothelial cell count may be unsuitable because excessive future cell loss could eventually lead to:
- Corneal swelling
- Blurred vision
- Corneal decompensation
- The need for corneal transplantation in severe cases
Long-term central-port ICL studies have generally reported favourable endothelial outcomes, but continued monitoring remains important.
Is ICL Suitable if You Have Glaucoma?
ICL may be unsuitable in patients with significant glaucoma.
The procedure can affect eye pressure through:
- Retained surgical viscoelastic
- Postoperative inflammation
- Steroid response
- Excessive vault
- Narrowing of the drainage angle
- Pigment release
- Pupillary block
US FDA labelling lists moderate-to-severe glaucomatous optic nerve damage as a contraindication and states that safety has not been established in patients with glaucoma or ocular hypertension.
A patient with a history of raised eye pressure, narrow angles, pigment dispersion, pseudoexfoliation or a strong glaucoma risk requires careful evaluation.
Some patients with mild or well-controlled pressure abnormalities may be considered only after specialist assessment, but suitability is highly individual.
Is ICL Suitable if You Have Cataract?
A visually significant cataract generally makes ICL a poor choice.
ICL surgery leaves the natural lens in place, so it does not treat the cataract.
Implanting an ICL when cataract is already developing may mean:
- Vision remains limited by the cataract
- Glare and night symptoms persist
- The ICL must be removed relatively soon
- Cataract surgery is still required
- The patient undergoes two intraocular procedures instead of one
An older patient with myopia, presbyopia and early cataract may be more appropriately treated with cataract surgery or refractive lens exchange.
Modern central-port ICLs appear to have reduced lens-opacity concerns compared with older designs, but cataract remains a recognised long-term risk. Age and low vault have been associated with cataract development in long-term studies.
Is ICL Suitable if You Have Retinal Problems?
Many highly myopic patients have an increased lifetime risk of retinal disease because the eye is elongated.
Possible conditions include:
- Retinal holes
- Retinal tears
- Lattice degeneration
- Retinal detachment
- Myopic macular degeneration
- Macular haemorrhage
- Epiretinal membrane
- Other peripheral retinal abnormalities
ICL corrects the optical blur caused by myopia but does not shorten the eye or remove these risks.
A dilated retinal examination is therefore important before surgery.
Selected retinal holes or tears may require treatment before ICL surgery. Other retinal findings may simply need observation.
Long-term comparative studies have not found that central-port ICL implantation necessarily increases retinal-detachment prevalence beyond the underlying risk of high myopia. However, these results do not mean that retinal detachment cannot occur after surgery.
A patient with active or vision-limiting retinal disease may be unsuitable if ICL surgery is unlikely to provide meaningful visual benefit.
Is ICL Suitable After Previous Retinal Surgery?
Previous retinal surgery does not automatically rule out ICL, but it makes the assessment more complex.
The surgeon must consider:
- Why retinal surgery was required
- Current retinal stability
- Visual potential
- Previous scleral buckle or vitrectomy
- Changes in eye anatomy
- Risk of future retinal procedures
- Whether the prescription is stable
- Whether another operation is justified
FDA information states that safety and effectiveness have not been established in patients with previous retinal-detachment surgery.
This does not mean that treatment is never performed, but it should not be regarded as routine.
Is ICL Suitable After LASIK, SMILE or PRK?
ICL may be considered after previous corneal laser surgery when:
- A significant residual or recurrent prescription remains
- Further corneal tissue removal would be undesirable
- The cornea is stable
- The natural lens is clear
- The internal eye anatomy is suitable
- The endothelial cell count is adequate
Previous refractive surgery makes assessment more individualised.
The surgeon must determine whether the recurrent prescription is caused by:
- Natural myopia progression
- Corneal regression
- Corneal ectasia
- Cataract
- Measurement variability
- Another eye condition
ICL should not be used simply to mask progressive corneal ectasia without addressing the underlying instability.
Is ICL Suitable for Contact-Sport Athletes?
ICL may be attractive to patients involved in contact sports because it does not create a LASIK flap.
Potential candidates include people involved in:
- Martial arts
- Boxing
- Rugby
- Football
- Water polo
- Military or tactical work
- Occupations with facial-trauma risk
However, the absence of a flap does not make an ICL-protected eye immune to injury.
Significant trauma can damage:
- The ICL
- The iris
- The drainage angle
- The natural lens
- The retina
- The corneal incision
Protective eyewear remains important.
A patient should discuss the precise sport, level of competition and expected trauma risk with the surgeon.
Is ICL Suitable for People With Large Pupils?
Possibly, but pupil size affects counselling.
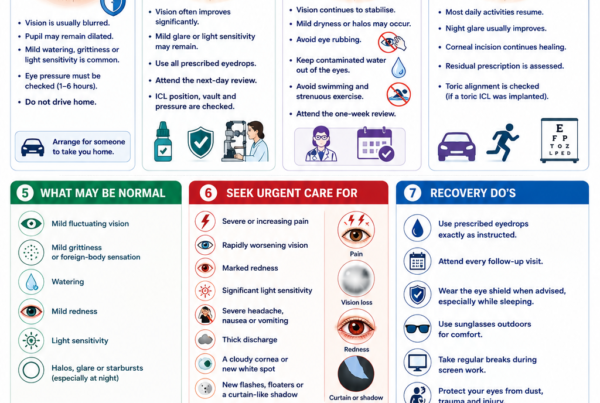
Patients with large pupils in dim lighting may be more aware of:
- Halos
- Glare
- Starbursts
- Light scatter
- Night-driving difficulty
These symptoms may occur when the pupil extends beyond the effective optical zone of the ICL or because of the interaction between the pupil, central port and lens optics.
FDA patient information specifically advises discussing pupil size because larger pupils may increase glare or halo symptoms.
Large pupils are not necessarily an absolute contraindication, but the patient should understand the potential effect on night vision.
Is ICL Suitable During Pregnancy or Breastfeeding?
Elective ICL surgery is generally postponed during pregnancy and breastfeeding.
Hormonal and fluid changes can temporarily affect:
- Refraction
- Corneal thickness
- Tear-film function
- Contact lens tolerance
- Blood sugar control
- Medication safety
US FDA labelling lists pregnancy and nursing as contraindications for EVO ICL implantation.
Surgery can be reconsidered once pregnancy and breastfeeding have ended and the prescription and ocular measurements have stabilised.
Is ICL Suitable if You Have Diabetes?
Diabetes does not automatically exclude every patient, but suitability depends on disease control and eye health.
Important considerations include:
- Stability of blood glucose
- Stability of the spectacle prescription
- Presence of diabetic retinopathy
- Corneal healing
- Infection risk
- Kidney and cardiovascular complications
- Medication use
Blood glucose fluctuations can change refraction, making lens-power calculation less reliable.
Patients with diabetic retinopathy or poorly controlled diabetes may be unsuitable.
FDA information states that safety and effectiveness have not been established in patients with diabetic retinopathy or insulin-dependent diabetes.
What Other Medical Conditions May Affect Suitability?
Additional caution may be required in patients with:
- Autoimmune disease
- Immunosuppression
- Uncontrolled inflammatory disease
- Recurrent eye inflammation
- Severe atopic disease
- Poor wound healing
- Active infection
- Significant neurological disease affecting vision
- Life-threatening systemic illness
- Medications that alter healing or immune function
The relevance depends on the condition, its severity, current treatment and whether it is stable.
A complete medical and medication history should be provided before surgery.
Who Should Not Have ICL Surgery?
ICL surgery should generally not proceed when the risks outweigh the likely visual benefit.
The Prescription Is Unstable
Continuing myopia progression may result in a residual or recurrent prescription after surgery.
The Anterior Chamber Is Too Shallow
Inadequate space increases the risk of angle crowding, pressure elevation and endothelial damage.
The Drainage Angles Are Too Narrow
The ICL may further narrow the drainage pathway and increase glaucoma risk.
The Endothelial Cell Count Is Inadequate
Insufficient endothelial reserve may place the cornea at risk of future swelling and decompensation.
Moderate or Severe Glaucoma Is Present
An implanted lens and postoperative pressure changes may threaten an already damaged optic nerve.
A Significant Cataract Is Present
Cataract surgery, rather than ICL implantation, may better address the patient’s visual needs.
Active Inflammation or Infection Is Present
Examples include:
- Uveitis
- Keratitis
- Conjunctivitis
- Active blepharitis
- Significant allergic inflammation
- Eyelid infection
Elective surgery should be delayed until the condition is adequately treated.
Progressive Keratoconus or Ectasia Is Present
ICL does not stabilise an unstable cornea.
Vision Is Limited by Retinal or Optic Nerve Disease
Correcting the spectacle prescription will not restore vision lost from advanced retinal, macular or optic nerve disease.
The Patient Is Pregnant or Breastfeeding
Measurements and prescription may be unstable, and elective surgery is normally deferred.
Expectations Are Unrealistic
A patient may be unsuitable if they expect:
- Guaranteed perfect vision
- Complete elimination of glasses in every situation
- No possibility of glare or halos
- No future cataract
- No future retinal disease
- No need for follow-up
- No possibility of additional surgery
Informed expectations are part of surgical suitability.
Does ICL Guarantee Freedom From Glasses?
No.
Many suitable patients become substantially less dependent on glasses or contact lenses, but some may still require spectacles for:
- Fine distance vision
- Night driving
- Reading after presbyopia develops
- Residual astigmatism
- Small undercorrection or overcorrection
- Future prescription changes
- Retinal or corneal limitations
No lens-power calculation can guarantee an exact zero prescription.
Can an ICL Be Removed if the Patient Is Unsuitable Later?
The ICL can usually be surgically removed or exchanged.
Reasons may include:
- Incorrect vault
- Incorrect power
- Toric lens rotation
- Cataract
- Raised eye pressure
- Inflammation
- Endothelial concerns
- Patient intolerance
However, removal requires another intraocular operation.
ICL should therefore be described as removable, rather than completely reversible. FDA patient information notes that the eye cannot be guaranteed to return to precisely its preoperative state after the lens is removed.
What Tests Determine ICL Suitability?
A detailed preoperative assessment is essential.
Refraction and Visual Acuity
Testing determines:
- The degree of myopia
- The amount and axis of astigmatism
- Best-corrected visual acuity
- Prescription stability
- The expected visual potential
Cycloplegic refraction may be performed in selected patients to temporarily relax accommodation.
Corneal Topography and Tomography
These scans assess:
- Corneal shape
- Corneal thickness
- Astigmatism
- Keratoconus
- Ectasia risk
- Previous laser treatment
- Corneal scars or irregularities
Normal tomography is not as central to ICL as it is to LASIK or SMILE, but it remains essential for understanding the source of the refractive error and excluding progressive corneal disease.
Anterior Chamber Depth
This confirms that there is adequate internal space for the ICL.
Drainage-Angle Examination
Gonioscopy or anterior-segment imaging evaluates whether the drainage angles are sufficiently open.
Internal Eye Measurements
Measurements may include:
- White-to-white diameter
- Sulcus-to-sulcus dimensions
- Anterior chamber width
- Crystalline lens rise
- Lens thickness
- Pupil size
These contribute to ICL-size selection and vault prediction.
A review of ICL planning emphasised that no single measurement perfectly predicts postoperative vault and that modern planning increasingly combines several internal anatomical parameters.
Endothelial Cell Count
Specular microscopy measures the number, size and shape of corneal endothelial cells.
Eye Pressure
Eye pressure is measured, and the optic nerve is evaluated for glaucoma.
Natural-Lens Examination
The natural lens is examined for:
- Cataract
- Anterior subcapsular opacity
- Abnormal shape or position
- Other lens disease
Dilated Retinal Examination
The retina is examined for:
- Retinal holes
- Tears
- Lattice degeneration
- Detachment
- Macular degeneration
- Myopic macular disease
- Other peripheral changes
Dry-Eye and Eyelid Assessment
The examination may identify:
- Tear-film instability
- Meibomian gland dysfunction
- Blepharitis
- Allergy
- Contact lens-related inflammation
These conditions should be treated before surgery.
What Makes Someone an Excellent ICL Candidate?
An excellent candidate typically has:
- Stable myopia, with or without regular astigmatism
- A prescription for which ICL offers a meaningful advantage
- A clear natural lens
- An adequately deep anterior chamber
- Open drainage angles
- A healthy endothelial cell count
- Normal or acceptably stable corneal findings
- Controlled dry-eye and eyelid health
- Normal or stable retinal findings
- No significant glaucoma
- Realistic expectations
- Willingness to attend lifelong eye examinations
What Makes Someone a Borderline Candidate?
A borderline candidate may have:
- Mild prescription instability
- Age over 40
- Early but non-significant lens changes
- An anterior chamber close to the lower acceptable limit
- An endothelial cell count close to the minimum threshold
- Mild glaucoma risk
- A history of uveitis
- Stable keratoconus
- Previous retinal surgery
- Very large pupils
- Significant dry eye
- Previous corneal refractive surgery
Borderline suitability does not necessarily mean that surgery cannot be performed.
It means that:
- Additional tests may be required
- Alternatives should be considered carefully
- The expected benefit must justify the added risk
- Counselling should be more detailed
- Follow-up may need to be more frequent
What Alternatives Are Available if You Are Not Suitable?
Alternatives may include:
- Glasses
- Soft contact lenses
- Rigid gas-permeable contact lenses
- Scleral lenses
- Orthokeratology
- LASIK
- SMILE
- PRK or surface laser treatment
- Corneal cross-linking for progressive keratoconus
- Cataract surgery
- Refractive lens exchange in selected older patients
- Continued observation
Choosing not to undergo elective surgery is also a valid option.
What Questions Should You Ask Before ICL Surgery?
Useful questions include:
- Is my prescription stable?
- Why is ICL preferable to LASIK, SMILE or PRK for my eyes?
- What is my anterior chamber depth?
- Are my drainage angles sufficiently open?
- What is my endothelial cell count?
- Is my natural lens completely clear?
- Is my corneal tomography normal?
- What ICL size will be used?
- What postoperative vault do you expect?
- What is my risk of cataract?
- What is my risk of raised eye pressure?
- How might my pupil size affect night vision?
- Do I have any retinal holes or degeneration?
- Will I still need reading glasses?
- What happens if a prescription remains?
- How often will I need long-term follow-up?
- Under what circumstances would the lens need to be removed or exchanged?
When Should Surgery Be Postponed?
ICL surgery may be postponed when:
- The prescription is still changing
- Contact lenses have not been stopped long enough for accurate measurements
- Dry eye remains uncontrolled
- Blepharitis or allergy is active
- An eye infection is present
- Blood glucose is unstable
- Pregnancy or breastfeeding is ongoing
- Retinal treatment is required
- Corneal stability remains uncertain
- Additional glaucoma investigations are needed
- The patient needs more time to consider the alternatives
Postponing surgery does not necessarily mean permanent unsuitability.
It may allow the eye to stabilise and improve the accuracy and safety of the eventual procedure.
Frequently Asked Questions About ICL Suitability
Is My Prescription High Enough for ICL?
ICL is commonly used for moderate-to-high myopia, but modern central-port lenses have also produced good results in lower myopia.
Suitability depends on more than the prescription. Corneal anatomy, dry-eye status, internal eye dimensions and the relative merits of laser surgery must also be considered.
Can I Have ICL With a Low Prescription?
Possibly.
The question is not only whether ICL can correct the prescription, but whether an intraocular operation offers sufficient advantage over glasses, contact lenses or corneal laser surgery.
Can I Have ICL if My Corneas Are Thin?
Potentially, yes.
Because ICL does not remove central corneal tissue, it may be considered when corneal thickness limits LASIK or SMILE.
However, corneal tomography is still required to exclude progressive keratoconus or ectasia.
Can I Have ICL if I Have Dry Eyes?
Many patients with dry-eye risk may be suitable.
The underlying dry eye, blepharitis or meibomian gland dysfunction should be treated before surgery.
Can I Have ICL if I Have Astigmatism?
A toric ICL can correct regular myopic astigmatism within the available treatment range.
Irregular astigmatism may not be completely corrected.
Can I Have ICL After Age 40?
Possibly, if the natural lens is clear and the internal anatomy is suitable.
Presbyopia and cataract risk must be discussed carefully. Some patients may be better served by cataract surgery or lens replacement.
Can I Have ICL if I Have Keratoconus?
Only selected patients with stable, non-progressive disease may be considered.
ICL does not treat or stabilise keratoconus.
Can I Have ICL if I Have Glaucoma?
Significant glaucoma generally makes ICL unsuitable.
Patients with ocular hypertension, narrow angles or glaucoma risk require individual specialist assessment.
Can I Have ICL if I Have Had LASIK?
Possibly.
ICL may be considered when a residual or recurrent prescription remains and further corneal laser treatment is undesirable.
Can I Have ICL if I Have Retinal Holes?
Retinal holes require assessment.
Some may only need observation, while others may require laser treatment before refractive surgery. The decision depends on the appearance, symptoms and surrounding retina.
Is ICL Suitable if I Play Contact Sports?
ICL avoids a LASIK flap and may be attractive for some contact-sport athletes.
It does not prevent internal eye injury from trauma, so protective eyewear remains important.
How Stable Must My Prescription Be?
Surgeons commonly look for no significant change over approximately one year, although the acceptable variation depends on age, prescription and circumstances.
Will I Still Need Reading Glasses?
Possibly.
A standard ICL does not prevent presbyopia. Patients approaching or over 40 should expect that near-vision needs may change.
Is an ICL Permanent?
The lens is designed to remain inside the eye long term.
It can usually be removed or exchanged, but removal requires another operation.
Do I Need Follow-Up for Life?
Regular long-term eye examinations are recommended.
Monitoring may include:
- Vision and refraction
- Eye pressure
- ICL position
- Vault
- Drainage-angle anatomy
- Endothelial cells
- Cataract
- Retinal health
FDA patient information recommends regular monitoring of the corneal endothelium, natural lens and eye pressure for as long as the ICL remains in the eye.
Key Takeaway
ICL surgery may be suitable for adults with stable myopia, with or without astigmatism, who have adequate internal eye anatomy, a healthy corneal endothelial cell count and a clear natural lens.
It is particularly useful for patients with:
- Moderate-to-very-high myopia
- Thin or laser-unsuitable corneas
- Significant dry-eye concerns
- A desire to preserve central corneal tissue
- A lifestyle in which avoiding a corneal flap is beneficial
However, ICL may be unsuitable when there is:
- A shallow anterior chamber
- Narrow drainage angles
- An inadequate endothelial cell count
- Significant cataract
- Moderate or advanced glaucoma
- Active inflammation or infection
- Progressive keratoconus
- Unstable myopia
- Pregnancy or breastfeeding
- Retinal or optic nerve disease that substantially limits visual potential
The spectacle prescription is only one part of the decision.
A comprehensive assessment of the cornea, tear film, anterior chamber, drainage angles, endothelial cells, natural lens, eye pressure and retina is necessary before deciding whether ICL is the safest and most appropriate form of vision correction.
References
- US Food and Drug Administration. EVO/EVO+ Visian Implantable Collamer Lens: Recently Approved Device.
- US Food and Drug Administration. EVO ICL Patient Information Booklet.
- US Food and Drug Administration. EVO ICL Instructions for Use.
- Kamiya K, et al. Posterior Chamber Phakic Intraocular Lens Implantation: Comparative Multicentre Study in Eyes With Low-to-Moderate or High Myopia. 2018.
- Du J, et al. Efficacy and Safety of Implantable Collamer Lens V4c Implantation in Low and High Myopia. 2023.
- Larivoir NB, et al. Efficacy, Predictability and Safety of Phakic Implantable Collamer Lenses With a Central Port: A Meta-analysis. 2025.
- Fernández-Vega-Cueto L, et al. Seven-Year Follow-up of Posterior Chamber Phakic Intraocular Lens With Central Port Design. 2021.
- Alfonso-Bartolozzi B, et al. Ten-Year Follow-up of Posterior Chamber Phakic Intraocular Lenses With Central-Port Design. 2024.
- Chung B, et al. Ten-Year Clinical Outcomes of V4c Implantable Collamer Lens Implantation. 2025.
- Kim YH, et al. Long-Term Outcome and Related Risk Factors in Implantable Collamer Lens Surgery. 2025.
- Packer KT, et al. US Military Implantable Collamer Lens Surgical Outcomes: An 11-Year Retrospective Review. 2022.
- Thompson V, et al. Implantable Collamer Lens Procedure Planning: A Review of Sizing and Vault. 2024.
- Zhang P, et al. Influencing Factors Comparing Different Vault Groups After Phakic Implantable Collamer Lens Implantation: Review and Meta-analysis. 2024.
- Moshirfar M, et al. Comparative Evaluation of Multiple Nomograms for Predicting Postoperative Vault After ICL Surgery. 2024.
- Fairaq R, et al. Outcomes and Complications of Implantable Collamer Lens Implantation in Stable Keratoconus. 2021.
- Emerah SH, et al. Visual and Refractive Outcomes of Posterior Chamber Phakic ICL in Stable Keratoconus. 2019.
- Xu W, et al. Long-Term Outcomes of Retinal Detachment in Phakic Eyes After ICL Implantation. 2020.
- Arrevola-Velasco L, et al. Ten-Year Prevalence of Rhegmatogenous Retinal Detachment Following ICL Implantation for High Myopia. 2023.
- Chen X, et al. Long-Term Comparison of Vault and Complications Between Central-Port and Non-Central-Port ICLs. 2022.
- Kamiya K, et al. Eight-Year Outcomes of Posterior Chamber Phakic ICL With Central-Port Technology. 2021.