Author: Dr Val Phua
Estimated reading time: 16 minutes
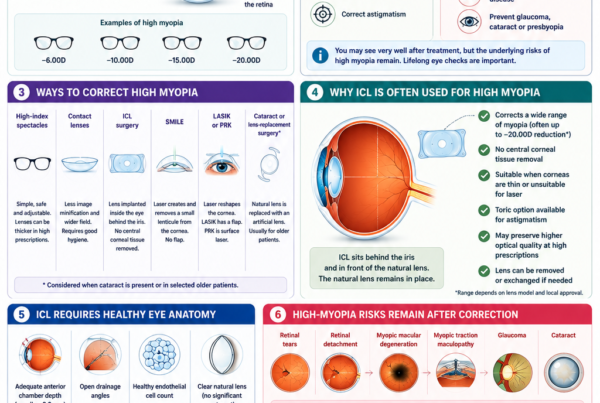
Implantable Collamer Lens surgery—commonly known as ICL surgery—can provide excellent correction of myopia and astigmatism, particularly in patients with high prescriptions or corneas that are less suitable for laser vision correction.
Unlike LASIK or SMILE, ICL surgery does not remove central corneal tissue. A soft corrective lens is implanted behind the iris and in front of the natural crystalline lens.
Modern central-port ICLs have demonstrated favourable safety, accuracy and visual outcomes in appropriately selected patients. However, ICL implantation remains an operation inside the eye. It therefore carries risks that do not occur with spectacles, contact lenses or corneal laser surgery.
Potential complications include:
- Raised eye pressure
- Incorrect ICL vault
- Cataract
- Corneal endothelial cell loss
- Glare and halos
- Residual prescription
- Toric ICL rotation
- Inflammation
- Infection
- The need for lens repositioning, exchange or removal
A 2026 systematic review concluded that posterior chamber phakic lenses have a low overall incidence of complications and that sight-threatening events appear very uncommon. However, the authors cautioned that relatively short follow-up and bias within the available studies may underestimate complications that emerge many years after surgery.
How Safe Is Modern ICL Surgery?
Modern EVO ICL lenses contain a small central opening that permits the natural circulation of aqueous fluid through the lens. This has reduced the risk of pupillary block and anterior subcapsular cataract compared with older ICL models that did not have a central port.
In the three-year United States FDA prospective study:
- Two eyes, or 0.32%, required ICL exchange because of high vault
- One eye, or 0.16%, developed an anterior subcapsular cataract
- No eye developed pupillary block requiring peripheral iridotomy
- No eye developed raised pressure due to angle narrowing or pigment dispersion
- Mean endothelial cell density decreased by 6.7% at three years
These figures describe one carefully controlled clinical study and should not be treated as universal complication rates for every surgeon, patient or healthcare setting.
Ten-year studies of central-port ICLs have also reported stable vision and eye pressure with relatively modest average endothelial cell reduction in selected cohorts. Nevertheless, study populations, lens models, patient ages and definitions of complications differ, making direct comparison difficult.
What Is the Difference Between a Side Effect and a Complication?
A side effect is an expected or relatively common consequence that is usually temporary and does not cause permanent harm.
Examples include:
- Mild grittiness
- Watering
- Temporary blurred vision
- Mild redness
- Light sensitivity
- Glare or halos during early recovery
A complication is an unintended medical problem that may require additional treatment or surgery.
Examples include:
- Significantly raised eye pressure
- Cataract
- Corneal endothelial damage
- Infection
- Incorrect lens position
- Retinal detachment
- Loss of best-corrected vision
The distinction is not always absolute. A mild pressure increase may be temporary, while an untreated severe pressure increase can damage the optic nerve.
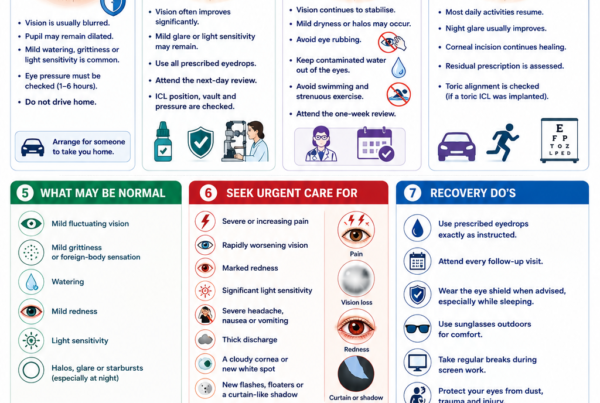
Common Temporary Effects After ICL Surgery
Blurred or Fluctuating Vision
Vision may be blurred during the first hours or days because of:
- Dilated pupils
- Mild corneal swelling
- Tear-film disturbance
- Postoperative inflammation
- Residual surgical medication
- A temporary pressure change
- Adaptation to the new optical correction
Vision should generally improve rather than become progressively worse.
Sudden or rapidly worsening blur requires urgent assessment.
Grittiness and Watering
The small corneal incision, antiseptic preparation and postoperative eyedrops may temporarily irritate the eye surface.
Patients may notice:
- A sandy sensation
- Mild burning
- Watering
- A feeling that something is in the eye
- Increased sensitivity to wind or air-conditioning
These symptoms usually improve during the first several days.
Mild Redness
A small amount of conjunctival redness or a localised area of bleeding may occur after surgery.
This is usually harmless and gradually fades.
Increasing redness associated with pain, light sensitivity, discharge or reduced vision is not normal.
Light Sensitivity
The pupil may remain enlarged for several hours after surgery. Mild inflammation can also make bright light uncomfortable.
Sunglasses may improve comfort during the early recovery period.
Dry-Eye Symptoms
ICL surgery generally disrupts fewer central corneal nerves than LASIK, but it can still temporarily affect the eye surface because of:
- The corneal incision
- Frequent postoperative medication
- Eyedrop preservatives
- Reduced blinking
- Pre-existing blepharitis
- Meibomian gland dysfunction
Dryness may cause burning, grittiness, watering or fluctuating vision.
Glare, Halos and Night-Vision Symptoms
Patients may notice:
- Halos around headlights
- Glare from bright lights
- Starbursts
- Light scatter
- Arcs or rings of light
- Reduced confidence when driving at night
These symptoms are often more noticeable when the pupil enlarges in dim lighting.
Possible contributing factors include:
- A pupil larger than the ICL’s effective optical zone
- The optical edge of the lens
- The EVO central port
- Residual myopia or astigmatism
- Toric ICL misalignment
- Tear-film instability
- Early inflammation
- Neural adaptation
The FDA advises that glare and halos can begin or worsen after ICL surgery, particularly when the pupil is large in relation to the lens optic.
Many patients notice improvement over weeks or months. However, halos can remain a persistent visual symptom in some patients even when eye-chart vision is excellent.
Raised Eye Pressure
Raised intraocular pressure is one of the most important early complications after ICL surgery.
Possible causes include:
- Retained surgical viscoelastic
- Postoperative inflammation
- A steroid response
- Pupillary block
- Excessive vault
- Narrowing of the drainage angle
- Pigment dispersion
- Pre-existing glaucoma susceptibility
Early Pressure Elevation
An early pressure rise commonly results from viscoelastic material remaining inside the eye after surgery.
Viscoelastic is used to protect internal eye structures and create space during ICL implantation. If too much remains, it can obstruct the eye’s drainage system.
This is why pressure is usually checked within several hours of surgery and again during early follow-up. The FDA recommends an eye-pressure assessment between one and six hours after EVO ICL implantation.
Steroid-Induced Pressure Elevation
Steroid eyedrops are commonly prescribed to control postoperative inflammation.
Some patients are steroid responders and develop increased eye pressure after several days or weeks of treatment.
Management may involve:
- Reducing or changing the steroid
- Pressure-lowering eyedrops
- Oral pressure-lowering medication
- Closer monitoring
Patients should not discontinue prescribed steroids independently because uncontrolled inflammation can also harm the eye.
Pupillary Block
Pupillary block occurs when fluid cannot flow normally from behind the iris into the front of the eye.
This can produce a rapid and potentially dangerous increase in eye pressure.
The central port in modern EVO ICLs has greatly reduced this risk, but pupillary block may still be possible if:
- The central port is obstructed
- The lens is positioned incorrectly
- Severe inflammation occurs
- The lens is implanted upside down
- The internal anatomy is unusual
Symptoms of Significantly Raised Pressure
Possible symptoms include:
- Eye pain
- Headache
- Cloudy or blurred vision
- Coloured rings around lights
- Redness
- Nausea
- Vomiting
Raised pressure may occasionally cause few symptoms, which is why scheduled postoperative checks remain necessary. Reviews of ICL-related pressure complications emphasise that treatment must be directed at the underlying cause rather than simply lowering the pressure temporarily.
Can ICL Surgery Cause Glaucoma?
ICL surgery does not inevitably cause glaucoma.
However, prolonged or recurrent pressure elevation can damage the optic nerve. Possible mechanisms include:
- Chronic angle narrowing from excessive vault
- Pigment dispersion
- Steroid response
- Peripheral anterior synechiae
- Repeated pressure spikes
- Pre-existing glaucoma susceptibility
Patients with high myopia already have an increased risk of glaucoma, independent of ICL surgery. The optic nerve can also be more difficult to interpret in highly myopic eyes.
Moderate or advanced glaucoma is generally a contraindication to EVO ICL under FDA guidance. Patients with ocular hypertension, narrow angles, pigment dispersion or suspicious optic nerves require careful individual assessment.
Incorrect ICL Vault
Vault is the space between the back of the ICL and the front surface of the natural lens.
An appropriate vault is essential because the ICL must remain sufficiently separated from the natural lens without excessively crowding the front of the eye.
Complications are often related to a vault that is too low or too high.
What Are the Risks of Low Vault?
A very low vault may increase the risk of:
- Contact between the ICL and natural lens
- Anterior subcapsular lens opacity
- Cataract formation
- Reduced aqueous circulation
- Lens exchange
Vault often decreases gradually as the natural lens becomes thicker with age, which is one reason lifelong monitoring is important.
What Are the Risks of High Vault?
A very high vault may:
- Narrow the drainage angles
- Raise eye pressure
- Cause iris contact
- Produce pigment dispersion
- Increase inflammation
- Bring the ICL closer to the corneal endothelium
- Contribute to glare or optical symptoms
A paired-eye study found greater long-term endothelial cell reduction in eyes with high vault than in fellow eyes with lower vault, suggesting that excessive vault may affect more than eye pressure alone.
How Is Incorrect Vault Managed?
Management depends on:
- The measured vault
- Drainage-angle anatomy
- Eye pressure
- Endothelial cell count
- Natural-lens changes
- The patient’s symptoms
Options may include:
- Observation
- More frequent imaging
- Pressure-lowering medication
- Rotating a non-toric ICL to reduce vault
- Lens repositioning
- Exchange for a different size
- Lens removal
In a retrospective seven-year series of 2,283 implantations, 46 lenses—approximately 2%—required exchange or removal. Incorrect vault was the most common indication. This is a study-specific figure rather than a universal expected rate.
Cataract Formation
The ICL is positioned immediately in front of the natural crystalline lens.
A cataract may develop because of:
- Normal ageing
- Low vault
- Direct surgical contact with the natural lens
- Reduced fluid circulation around the lens
- Older age at implantation
- Very high myopia
- Individual anatomical factors
The cataract most specifically associated with ICL is an anterior subcapsular cataract, which develops at the front surface of the natural lens.
Modern central-port ICLs have reduced this complication compared with older models, but they have not eliminated it.
Who Has a Higher Cataract Risk?
Risk may be higher in patients who:
- Are older at the time of implantation
- Have a very high myopic prescription
- Have a shallow anterior chamber
- Develop low vault
- Already have early lens changes
- Retain the ICL for many years
Long-term studies involving different ICL generations have produced different cataract rates. One ten-year study of an earlier posterior chamber ICL model reported anterior subcapsular cataract in 10.5% of eyes, while another ten-year central-port study reported no ICL-induced anterior subcapsular opacity in its selected cohort. These differences illustrate why lens design, age, vault and study population must be considered when interpreting published risks.
What Happens if Cataract Develops?
If the cataract becomes visually significant:
- The ICL is usually removed.
- The cloudy natural lens is removed.
- A cataract intraocular lens is implanted.
Cataract surgery after ICL is usually feasible, but it represents an additional intraocular operation.
Corneal Endothelial Cell Loss
The corneal endothelium is a single layer of cells lining the inner surface of the cornea.
These cells pump excess fluid out of the cornea and keep it transparent. They have very limited regenerative ability.
Some endothelial cell loss occurs naturally with age, and additional loss may occur following intraocular surgery.
If the cell count becomes critically low, the cornea may develop:
- Persistent swelling
- Hazy vision
- Glare
- Painful surface blisters
- Corneal decompensation
Severe decompensation may require corneal transplantation.
The FDA recommends measuring endothelial cell density before surgery and monitoring it for as long as the EVO ICL remains inside the eye.
What Increases the Risk of Endothelial Cell Loss?
Possible risk factors include:
- A low preoperative endothelial cell count
- Excessive vault
- A shallow internal eye
- Surgical trauma
- Increasing age
- Inflammation
- Multiple intraocular procedures
- Abnormal ICL position
- Prolonged contact between the implant and internal structures
Published estimates vary considerably. In the three-year FDA EVO trial, mean endothelial cell density decreased by 6.7% from baseline, while a selected ten-year central-port cohort reported a mean reduction of approximately 4%. Differences in measurement methods, patient selection and follow-up complicate direct comparison.
Residual Prescription
ICL surgery cannot guarantee an exact zero prescription.
A patient may retain:
- Mild myopia
- Mild hyperopia
- Residual astigmatism
- An imbalance between the two eyes
Possible reasons include:
- Measurement variability
- Limited available lens powers
- Healing
- Incorrect lens power
- Toric rotation
- Incision-induced astigmatism
- Continued myopia progression
- Changes in the natural lens
Management may include:
- Observation
- Spectacles
- Contact lenses
- ICL exchange
- Toric ICL repositioning
- LASIK or PRK enhancement when the cornea is suitable
A small residual prescription that does not interfere with daily activities may not require further surgery.
Toric ICL Rotation
A toric ICL corrects astigmatism and must remain aligned with the intended axis.
If it rotates:
- Astigmatism correction is reduced
- Vision may become blurred
- Ghosting or shadowing may occur
- Night vision may deteriorate
- Glasses may be required
Small rotations may have little effect, particularly with lower toric powers. Larger rotations can substantially reduce the cylinder correction.
Management may include:
- Observation
- Spectacles
- Surgical repositioning
- Lens exchange
- Corneal laser enhancement
Long-term studies generally report good rotational stability, although clinically significant rotation and repositioning remain recognised risks.
ICL Malposition, Displacement or Incorrect Orientation
An ICL can occasionally be:
- Decentred
- Displaced
- Incorrectly oriented
- Implanted upside down
- Trapped in an abnormal position
- Damaged during insertion
Possible effects include:
- Blurred vision
- Abnormal vault
- Raised eye pressure
- Pupil distortion
- Iris chafing
- Inflammation
- Cataract
Significant malposition usually requires surgical correction.
Trauma can also displace an ICL after an initially successful operation. Although uncommon, significant eye injury should be examined even when vision initially appears acceptable.
Pupil Distortion and Iris Complications
The iris surrounds and lies immediately in front of the ICL.
Possible iris-related complications include:
- Pupil ovalisation
- Unequal pupil size
- A poorly reactive pupil
- Iris atrophy
- Pigment release
- Iris prolapse through the surgical wound
- Peripheral anterior synechiae
- Chronic iris irritation
A temporary abnormal pupil may result from:
- Surgical manipulation
- Raised eye pressure
- Medication
- Inflammation
Persistent distortion may affect appearance, glare and light sensitivity.
Pigment Dispersion
The back surface of the iris contains pigment.
If the ICL repeatedly rubs against the iris, pigment may be released and accumulate within the eye’s drainage system.
This may lead to:
- Increased trabecular pigmentation
- Raised eye pressure
- Pigmentary glaucoma
- Inflammation
Risk may be influenced by:
- Excessive vault
- ICL position
- Iris anatomy
- Pupil movement
- Lens sizing
Modern central-port lenses have shown favourable pressure outcomes, but long-term angle and pressure monitoring remains advisable.
Inflammation and Uveitis
Mild inflammation inside the eye is expected after surgery and is usually controlled with steroid eyedrops.
Excessive or persistent inflammation may cause:
- Pain
- Redness
- Light sensitivity
- Blurred vision
- Deposits on the ICL
- Posterior synechiae
- Raised eye pressure
- Cystoid macular oedema
Possible causes include:
- Surgical trauma
- Retained viscoelastic
- Infection
- Iris contact
- Pre-existing inflammatory disease
- Inadequate medication
- An unusual immune response
Patients with previous uveitis require especially careful assessment because the safety of EVO ICL has not been established in this group under FDA guidance.
Infection and Endophthalmitis
Because ICL surgery enters the eye, there is a small risk of serious intraocular infection.
Endophthalmitis is an infection involving the internal structures of the eye. It can cause rapid and permanent loss of vision if treatment is delayed.
Warning symptoms include:
- Increasing pain
- Rapidly worsening vision
- Marked redness
- Significant light sensitivity
- Eyelid swelling
- Increasing discharge
- A cloudy appearance within the eye
An older international survey estimated an endophthalmitis rate of approximately 0.017%, or roughly one case per 6,000 ICL procedures. Contemporary rates may differ because surgical techniques, lens designs, antisepsis and reporting practices have changed.
Treatment may require:
- Antibiotic injections into the eye
- Laboratory sampling
- Intensive topical treatment
- Vitrectomy
- Removal of the ICL in selected cases
Endophthalmitis is rare, but its potential severity is one reason ICL surgery should only be undertaken when its benefits justify intraocular risk.
Corneal Infection
The small corneal incision can also become infected.
Symptoms may include:
- Localised pain
- Redness
- Discharge
- Light sensitivity
- A white or grey corneal spot
- Reduced vision
Prompt treatment is required to reduce the risk of corneal scarring.
Retinal Tears and Retinal Detachment
Many ICL patients have high or very high myopia.
A highly myopic eye is often elongated and has a naturally increased lifetime risk of:
- Peripheral retinal degeneration
- Retinal holes
- Retinal tears
- Posterior vitreous detachment
- Retinal detachment
Correcting the prescription with an ICL does not shorten the eye or eliminate these underlying risks.
Long-term comparative studies have not found clear evidence that modern central-port ICL implantation itself adds substantial retinal-detachment risk beyond the baseline risk associated with high myopia. However, these studies cannot prove that the risk is zero.
A dilated retinal examination is therefore important before surgery, and new retinal symptoms require urgent assessment after surgery.
Warning Symptoms of a Retinal Tear or Detachment
Seek urgent care for:
- Sudden new floaters
- Flashes of light
- A curtain or shadow
- Sudden peripheral visual-field loss
- Sudden deterioration in vision
Myopic Macular Disease
ICL surgery improves focus but does not treat structural disease at the back of a highly myopic eye.
Vision may later be affected by:
- Myopic macular degeneration
- Myopic choroidal neovascularisation
- Macular haemorrhage
- Myopic traction maculopathy
- Macular hole
- Retinoschisis
These are primarily complications of high myopia rather than the implanted lens itself.
Patients should continue regular retinal and macular monitoring even when unaided vision after ICL surgery is excellent.
Loss of Best-Corrected Vision
Most patients maintain or improve their best-corrected visual acuity.
Nevertheless, it is possible to lose lines of vision that cannot be restored fully with spectacles.
Potential causes include:
- Infection
- Cataract
- Glaucoma
- Corneal decompensation
- Severe inflammation
- Retinal detachment
- Macular disease
- Surgical trauma
- Irregular astigmatism
The FDA identifies loss of two or more lines of best-corrected vision as a potential serious risk that should be discussed before surgery.
Could the ICL Need to Be Removed or Exchanged?
Yes.
Possible reasons include:
- Incorrect vault
- Incorrect lens power
- Toric rotation
- Cataract
- Raised eye pressure
- Endothelial cell concerns
- Inflammation
- Patient dissatisfaction
- Trauma or displacement
The ability to remove the ICL is an advantage over permanent corneal tissue removal. However, removal or exchange is another intraocular operation and carries additional risks.
ICL is therefore better described as removable rather than completely reversible.
Are Modern EVO ICL Risks Lower Than Older ICL Risks?
The central-port design appears to have reduced several complications associated with older non-port ICLs, particularly:
- Pupillary block
- The need for preoperative peripheral iridotomy
- Anterior subcapsular cataract related to impaired aqueous circulation
The three-year FDA EVO study reported no pupillary block requiring iridotomy and a very low incidence of anterior subcapsular cataract.
However, EVO ICL has not eliminated:
- Cataract risk
- Vault problems
- Endothelial cell loss
- Eye-pressure changes
- Glare and halos
- Infection
- The possibility of secondary surgery
Long-term evidence extending beyond ten to fifteen years remains more limited than short- and medium-term evidence.
Who Has a Higher Risk of ICL Complications?
Risk may be higher when there is:
- Older age
- Very high myopia
- A shallow anterior chamber
- Narrow drainage angles
- Low endothelial cell density
- Early cataract
- Glaucoma or ocular hypertension
- Pigment dispersion
- Previous uveitis
- Abnormal internal eye anatomy
- Inaccurate lens sizing
- Very low or high vault
- Large pupils
- Unstable refraction
- Poor adherence to medication or follow-up
The FDA lists inadequate anterior chamber depth, moderate-to-severe glaucomatous damage, pregnancy or nursing, and insufficient endothelial cell density among contraindications under its EVO ICL approval.
How Are ICL Risks Reduced?
Careful Patient Selection
Assessment should include:
- Stable refraction
- Corneal topography and tomography
- Anterior chamber depth
- Drainage-angle examination
- Internal eye measurements
- Endothelial cell count
- Eye pressure
- Optic nerve assessment
- Natural-lens examination
- Dilated retinal examination
Accurate ICL Sizing
Correct sizing reduces the risk of excessive or inadequate vault.
Modern planning may incorporate:
- White-to-white measurements
- Sulcus-to-sulcus dimensions
- Anterior chamber width
- Crystalline lens rise
- Angle-to-angle measurements
- Ultrasound biomicroscopy
- Anterior-segment OCT
No formula predicts vault perfectly, so postoperative measurement remains necessary.
Careful Surgical Technique
Risk reduction includes:
- Strict antiseptic preparation
- Minimising iris and lens contact
- Correct lens orientation
- Accurate toric alignment
- Complete removal of excess viscoelastic
- Checking wound integrity
- Appropriate postoperative medication
Early Postoperative Monitoring
Important early checks include:
- Eye pressure
- ICL position
- Vault
- Pupil shape
- Inflammation
- Corneal clarity
- Toric alignment
Long-Term Monitoring
Long-term reviews may assess:
- Vision and refraction
- Eye pressure
- Drainage-angle anatomy
- Vault
- Endothelial cell density
- Natural-lens clarity
- ICL position
- Retinal and macular health
- Optic nerve health
ICL Risks Compared With LASIK or SMILE
ICL, LASIK and SMILE have different risk profiles.
Risks More Specific to ICL
- Raised pressure from retained viscoelastic
- Incorrect vault
- Cataract
- Endothelial cell loss
- Toric lens rotation
- Intraocular inflammation
- Endophthalmitis
- Need for lens exchange
Risks More Specific to LASIK
- Flap displacement or wrinkles
- Epithelial ingrowth
- Flap inflammation
- Corneal ectasia
- Greater corneal nerve disruption
- Permanent corneal tissue removal
Risks More Specific to SMILE
- Difficult lenticule separation
- Retained lenticule fragments
- Cap tears
- Interface inflammation
- Corneal ectasia
- Permanent corneal tissue removal
ICL avoids corneal ablation but introduces intraocular risks. LASIK and SMILE avoid an implant inside the eye but permanently alter the cornea.
The safest operation is the one whose risks are best matched to the patient’s prescription, anatomy and lifestyle.
When Should You Seek Urgent Care After ICL Surgery?
Contact the surgeon or an emergency eye service immediately for:
- Severe or increasing pain
- Rapidly worsening vision
- Sudden loss of vision
- Marked or increasing redness
- Significant light sensitivity
- Severe headache
- Nausea or vomiting
- Thick discharge
- A cloudy cornea
- A white or grey spot on the eye
- A distorted or non-reactive pupil
- New flashes or floaters
- A curtain-like shadow
- Significant trauma to the operated eye
Do not wait for the next routine appointment if these symptoms develop.
Frequently Asked Questions About ICL Risks
Is ICL Surgery Dangerous?
Serious complications are uncommon in appropriately selected patients, but ICL is not risk-free.
Because the procedure takes place inside the eye, rare complications can potentially cause permanent visual loss.
What Is the Most Common Serious ICL Problem?
Incorrect vault and eye-pressure changes are among the more important reasons for additional treatment or lens exchange.
The most clinically important risk varies according to the patient’s age and anatomy.
Can ICL Cause Blindness?
Severe permanent visual loss is rare but possible.
Potential causes include:
- Endophthalmitis
- Uncontrolled glaucoma
- Corneal decompensation
- Retinal detachment
- Severe inflammation
- Surgical trauma
Can ICL Cause Cataract?
Yes.
The risk is influenced by age, vault, eye anatomy, lens design and duration of implantation.
Does Everyone Lose Endothelial Cells After ICL?
Some endothelial cell reduction can occur after intraocular surgery and as part of natural ageing.
The amount varies between patients. An adequate preoperative count and long-term monitoring are essential.
Can ICL Cause Glaucoma?
ICL can contribute to raised eye pressure through several mechanisms.
Prompt detection and treatment usually prevent permanent damage, but prolonged uncontrolled pressure can cause glaucoma.
Can an EVO ICL Cause Pupillary Block?
The central port has substantially reduced the risk, but pupillary block is not theoretically impossible.
Can the ICL Move?
Major movement is uncommon.
Toric lenses can rotate, and a lens may occasionally be displaced or positioned incorrectly.
Can the ICL Fall Out?
No.
It is positioned inside the eye and cannot fall out like a contact lens.
Can the ICL Be Removed?
Usually, yes.
Removal requires another intraocular operation and is not risk-free.
Can ICL Risks Develop Years Later?
Yes.
Possible later issues include:
- Cataract
- Endothelial cell loss
- Vault changes
- Glaucoma
- Pigment dispersion
- Natural progression of myopia
- Retinal or macular disease
Does ICL Increase Retinal-Detachment Risk?
High myopia itself increases retinal-detachment risk.
Available long-term comparative studies have not shown a clear additional risk from modern central-port ICL implantation, but regular retinal monitoring remains essential.
Is ICL Safer Than LASIK?
Neither procedure is universally safer.
ICL avoids corneal flap and tissue-removal risks but introduces intraocular, cataract, vault and pressure risks.
LASIK avoids intraocular surgery but introduces flap, dry-eye, ectasia and permanent corneal tissue-removal risks.
Are Halos Permanent?
They often become less noticeable over time, but some patients continue to experience halos in dim lighting.
Can Careful Screening Eliminate Every Risk?
No.
Screening substantially reduces avoidable risk but cannot make any operation completely risk-free.
Key Takeaway
Modern ICL surgery has a favourable safety profile in carefully selected patients, and serious sight-threatening complications are uncommon.
However, ICL is an intraocular operation. Important risks include:
- Raised eye pressure
- Incorrect vault
- Cataract
- Endothelial cell loss
- Glare and halos
- Residual prescription
- Toric lens rotation
- Inflammation
- Infection
- The need for additional surgery
Modern central-port EVO lenses have reduced the occurrence of pupillary block and some forms of anterior subcapsular cataract compared with older lens designs, but they have not eliminated all short- and long-term risks.
Safety depends on:
- Appropriate patient selection
- Accurate internal eye measurements
- Correct ICL sizing
- Careful surgical technique
- Early postoperative pressure checks
- Correct medication use
- Lifelong eye examinations
Patients should understand that excellent unaided vision does not remove the need to monitor the ICL, vault, eye pressure, corneal endothelial cells, natural lens, retina and optic nerve.
References
- US Food and Drug Administration. EVO and EVO+ Visian Implantable Collamer Lens Patient Information Booklet. 2022.
- US Food and Drug Administration. EVO and EVO+ Visian Implantable Collamer Lens Instructions for Use. 2022.
- Parkhurst G, et al. Three-Year Results From the United States FDA Prospective Multicentre Clinical Study of the EVO/EVO+ Implantable Collamer Lens. 2025.
- Passaro ML, et al. Potential Harms of Posterior Chamber Phakic Intraocular Lenses: A Systematic Review and Meta-analysis of Complication Incidence. 2026.
- Gong D, et al. Causes and Management Strategies for Elevated Intraocular Pressure After Implantable Collamer Lens Implantation. 2024.
- Thompson V, et al. Implantable Collamer Lens Procedure Planning: A Review of Sizing and Vault. 2024.
- Alhamzah A, et al. Indications for Exchange or Explantation of Phakic Implantable Collamer Lenses With a Central Port. 2021.
- Alfonso-Bartolozzi B, et al. Ten-Year Follow-up of Posterior Chamber Phakic Intraocular Lenses With Central-Port Design. 2024.
- Kim YH, et al. Long-Term Outcome and Related Risk Factors in Implantable Collamer Lens Surgery. 2025.
- Choi H, et al. Paired-Eye Comparison of Endothelial Cell Density and Vault Following ICL Implantation. 2024.
- Allan BD, et al. Endophthalmitis Rates After Implantation of the Intraocular Collamer Lens. 2009.
- Xu W, et al. Long-Term Outcomes of Retinal Detachment in Phakic Eyes After ICL Implantation. 2020.
- Arrevola-Velasco L, et al. Ten-Year Prevalence of Rhegmatogenous Retinal Detachment Following ICL Implantation for High Myopia. 2023.
- Mohr N, et al. Determinants of Subjective Quality of Vision After Phakic ICL Implantation. 2022.
- Nie LL, et al. Subjective and Objective Changes in Visual Quality After EVO ICL Implantation. 2025.
- Zhang H, et al. Analysis of Perioperative Problems Related to Implantable Collamer Lens Implantation and Their Management. 2022.