Author: Dr Val Phua
Estimated reading time: 15 minutes
Recovery after Implantable Collamer Lens surgery—commonly known as ICL surgery—is usually relatively quick.
Many patients notice a substantial improvement in their distance vision within the first day. Some are able to return to office-based work within a few days, although the speed of recovery varies between individuals.
Clearer vision does not mean that the eye has completely healed. During the first few weeks, the eye is still recovering from the corneal incision and intraocular surgery. The ICL position, vault, eye pressure, inflammation and visual result must be monitored carefully.
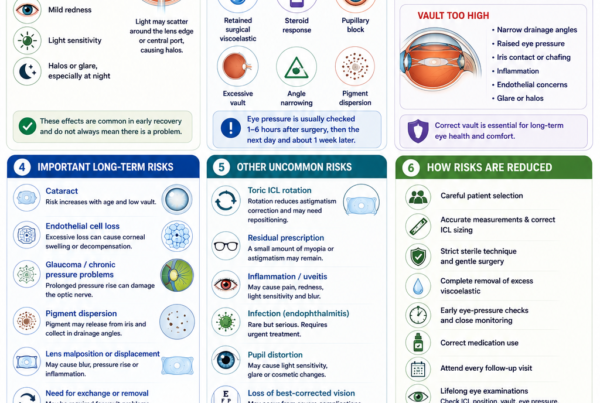
Early follow-up is particularly important because eye pressure can occasionally rise within the first few hours after surgery. United States FDA guidance recommends measuring eye pressure between one and six hours after EVO ICL implantation, followed by reviews the next day and approximately one week later.
Most patients recover without serious problems. However, increasing pain, rapidly worsening vision, marked redness, significant light sensitivity or nausea with headache should not be regarded as part of normal recovery.
What Happens Immediately After ICL Surgery?
ICL surgery is usually performed as a day procedure.
At the end of the operation, the surgeon may place:
- Antibiotic eyedrops
- Anti-inflammatory eyedrops
- Lubricating drops or ointment
- A transparent eye shield
- An eye patch in selected cases
Vision may initially be blurred because of:
- Pupil-dilating medication
- Anaesthetic medication
- Mild corneal swelling
- Temporary inflammation
- Tear-film disturbance
- Residual surgical fluid
- Adjustment to the new optical correction
The pupil may remain enlarged for several hours. This can make the eye sensitive to light and may temporarily increase glare or halos.
Patients should arrange for someone to take them home. They should not drive on the day of surgery.
Why Is Eye Pressure Checked Soon After Surgery?
A temporary increase in intraocular pressure is one of the main issues that surgeons monitor during the first several hours after ICL implantation.
Possible causes include:
- Residual surgical viscoelastic inside the eye
- Postoperative inflammation
- Pupillary block
- Excessive ICL vault
- Narrowing of the drainage angle
- An unusual response to medication
In the pivotal EVO ICL clinical study, some eyes developed an early pressure increase between one and six hours after surgery, usually because surgical viscoelastic remained inside the eye. These pressure elevations generally settled by the following day after observation or treatment.
This is why patients should not leave immediately after surgery without the checks arranged by their surgeon.
Possible Symptoms of Raised Eye Pressure
A significant pressure increase may cause:
- Eye pain
- Headache
- Redness
- Cloudy or blurred vision
- Coloured rings around lights
- Nausea
- Vomiting
Raised eye pressure may occasionally cause few obvious symptoms. Attending the scheduled pressure check is therefore important even when the eye feels comfortable.
Recovery After ICL Surgery: The Typical Timeline
Recovery differs between patients. The following timeline describes what many patients experience, but it should not replace the instructions provided by the operating surgeon.
The First Few Hours
Vision is usually blurred immediately after surgery, although some patients already notice that distant objects are clearer than they were without glasses.
Common experiences include:
- Dilated pupils
- Light sensitivity
- Mild watering
- A gritty or foreign-body sensation
- Mild redness
- Halos around lights
- Temporary fluctuations in vision
- Mild discomfort around the eye
The surgeon will usually check:
- Eye pressure
- The position of the ICL
- The pupil
- The corneal incision
- The amount of inflammation
- The clarity of the cornea
Severe pain or rapidly worsening vision is not expected.
The First Night
Patients should rest and avoid unnecessary visual strain.
The surgeon may advise wearing an eye shield during sleep to prevent accidental rubbing or pressure on the eye.
During the first night:
- Do not rub or press the eye
- Use all prescribed medication
- Avoid getting water or skincare products into the eye
- Do not drive
- Avoid alcohol if it interferes with medication or recovery
- Contact the clinic if pain or vision worsens
Mild discomfort may improve after resting or taking the pain medication recommended by the surgeon.
The First Day After Surgery
Many patients notice significantly clearer vision by the following morning.
However, vision may not yet feel perfectly sharp. It may fluctuate because of:
- Residual pupil dilation
- Mild corneal swelling
- Tear-film instability
- Postoperative inflammation
- A small residual prescription
- Differences between the two eyes
- Early adaptation to the ICL optics
The day-one examination commonly assesses:
- Unaided visual acuity
- Refraction when needed
- Eye pressure
- Corneal clarity
- Inflammation
- ICL position
- ICL vault
- Pupil shape
- Toric alignment when a toric ICL was implanted
The FDA professional guidance recommends assessing vault within approximately 24 hours after implantation.
The First Week
During the first week, most mild irritation and light sensitivity should gradually improve.
Patients may still notice:
- Mild fluctuations in vision
- Glare or halos at night
- A slightly gritty sensation
- Dryness
- Mild redness
- Different visual clarity between the eyes
- Increased awareness of bright lights
Antibiotic and anti-inflammatory eyedrops are commonly used during this period. The precise medication, frequency and duration vary between surgeons.
The official EVO ICL patient booklet advises patients to use prescribed medication carefully, avoid eye rubbing during the early postoperative period and attend reviews the next day and approximately one week after surgery.
Two to Four Weeks After Surgery
By this stage, many patients have returned to their usual daily routines.
Vision generally becomes more stable as:
- The corneal incision heals
- Inflammation settles
- The tear film improves
- The pupil returns to its normal behaviour
- The brain adapts to the new optical correction
Some patients continue to notice halos or glare, particularly:
- When driving at night
- Around headlights
- In very dim surroundings
- When the pupil is large
- When one eye has a small residual prescription
A single-centre United States study reported strong one-month visual outcomes after EVO and EVO+ ICL implantation. Among eyes capable of 20/20 corrected vision before surgery, 95.2% achieved 20/20 or better unaided vision at one month. These results represent one clinical population and should not be interpreted as a guarantee for every patient.
One to Three Months After Surgery
Most patients have stable functional vision by this stage.
The surgeon may assess:
- Final or near-final refraction
- Residual myopia or astigmatism
- Toric ICL alignment
- Eye pressure
- Vault
- Drainage-angle anatomy
- Corneal endothelial health
- The natural lens
- Retinal health when indicated
If a small residual prescription remains, the surgeon may recommend:
- Observation
- Spectacles for selected tasks
- Further refraction after additional stabilisation
- Toric lens repositioning
- ICL exchange
- Corneal laser enhancement in suitable eyes
Enhancement decisions should not be rushed while the refraction or eye surface is still changing.
Six Months and Beyond
By six months, vision and refraction are usually stable unless there is:
- Continuing myopia progression
- Toric lens rotation
- Dry-eye-related fluctuation
- Cataract development
- An ICL sizing or vault issue
- Another corneal, retinal or optic nerve condition
The ICL is designed to remain inside the eye long term, but ongoing eye examinations remain necessary.
Long-term central-port ICL studies have reported favourable refractive stability and visual outcomes. Nevertheless, the natural lens, eye pressure, drainage angles, endothelial cells and retina continue to change with age.
What Symptoms Are Normal After ICL Surgery?
The following symptoms can occur during uncomplicated early recovery.
Mild Blurred or Fluctuating Vision
Vision may vary during the first days because of:
- Pupil dilation
- Tear-film disturbance
- Mild inflammation
- Corneal swelling
- Adjustment to the new prescription
The vision should generally trend towards improvement rather than become progressively worse.
Mild Grittiness or Foreign-Body Sensation
The small corneal incision and postoperative drops can make the eye feel slightly gritty.
This should gradually settle.
Mild Redness
A small area of redness near the incision or on the conjunctiva may be present.
Extensive or increasing redness, particularly when associated with pain or vision loss, requires assessment.
Watering
Reflex tearing can occur because the eye surface is temporarily irritated.
Light Sensitivity
Sensitivity to bright light is common while the pupil remains dilated or mild inflammation is present.
Sunglasses may improve comfort.
Halos, Glare and Starbursts
These may be noticed around lights, especially at night.
Possible contributing factors include:
- A dilated pupil
- The edge or central port of the ICL
- Residual refractive error
- Early inflammation
- Tear-film instability
- Neural adaptation
Small observational studies suggest that glare often becomes less noticeable over the first few weeks or months, although some patients continue to experience mild night-vision symptoms.
Mild Dryness
ICL surgery generally causes less central corneal nerve disruption than LASIK, but temporary dryness can still occur because of:
- The corneal incision
- Antiseptic preparation
- Frequent postoperative eyedrops
- Preservatives
- Reduced blinking
- Pre-existing blepharitis or meibomian gland dysfunction
Lubricating eyedrops may be recommended.
What Symptoms Are Not Normal?
Contact the surgeon urgently if you develop:
- Severe or increasing eye pain
- Rapidly worsening vision
- A sudden significant drop in vision
- Marked or increasing redness
- Significant light sensitivity
- Thick discharge
- Increasing eyelid swelling
- A cloudy cornea
- A new white or grey spot on the eye
- Severe headache
- Nausea or vomiting
- A distorted or unusually fixed pupil
- New flashes or floaters
- A curtain or shadow across the vision
These symptoms may indicate:
- Raised eye pressure
- Corneal infection
- Endophthalmitis
- Severe inflammation
- Wound leakage
- ICL displacement
- Pupillary block
- Retinal tear or detachment
- Another sight-threatening complication
Do not wait for the next scheduled appointment when symptoms are rapidly worsening.
What Eyedrops Are Used After ICL Surgery?
The exact regimen varies.
Common categories include:
Antibiotic Eyedrops
These are used to reduce the risk of postoperative infection.
They are usually prescribed for a limited period.
Steroid or Anti-Inflammatory Eyedrops
These reduce inflammation inside the eye.
The dose is often gradually reduced according to the surgeon’s instructions.
Steroid drops can increase eye pressure in susceptible individuals. Do not use them more frequently or for longer than prescribed.
Lubricating Eyedrops
Preservative-free artificial tears may improve:
- Grittiness
- Dryness
- Burning
- Fluctuating vision
- Eye fatigue
Pressure-Lowering Medication
Some patients temporarily require medication to reduce eye pressure.
This may include eyedrops or oral medication, depending on the cause and degree of pressure elevation.
How Should You Use Eyedrops Correctly?
To reduce contamination and improve absorption:
- Wash and dry your hands.
- Shake the bottle if instructed.
- Tilt your head backwards.
- Gently pull down the lower eyelid.
- Place one drop into the lower eyelid pocket.
- Avoid touching the bottle tip against the eye, eyelashes or skin.
- Close the eye gently.
- Apply light pressure to the inner corner when advised.
- Wait several minutes between different medications.
- Replace the bottle cap immediately.
One properly placed drop is usually sufficient. Applying several drops at once does not necessarily improve the effect.
Contact the clinic if you are uncertain about the medication schedule rather than stopping or changing it independently.
When Can You Return to Work?
Many patients with office-based work can return within one to three days.
Some can work the following day if:
- Vision is sufficiently clear
- Light sensitivity is mild
- Eye pressure is normal
- The surgeon is satisfied with recovery
- The work does not involve dust, contaminants or physical risk
An NHS patient guide notes that many patients see well enough to return to work the day after ICL surgery, although individual recovery varies.
More time may be needed when work involves:
- Heavy physical activity
- Outdoor dust or fumes
- Machinery
- Driving
- Water exposure
- Contact sports
- Risk of impact to the eye
- Long shifts without access to eyedrops
When Can You Drive?
Do not drive on the day of surgery.
Driving may resume only when:
- Vision meets the legal driving requirement
- The operated eye is comfortable
- Glare and light sensitivity are manageable
- Both eyes work together adequately
- The surgeon confirms that it is safe
Some patients may meet the visual requirement by the next day, while others require more time.
Night driving may remain more difficult than daytime driving during the early recovery period because of glare and halos.
Can You Use a Computer or Phone?
Yes, once comfortable.
Screen use does not normally damage the implanted ICL or displace it.
However, prolonged concentration reduces blink frequency and may worsen:
- Dryness
- Grittiness
- Watering
- Eye fatigue
- Fluctuating vision
During the first few days:
- Use screens in shorter sessions
- Blink fully and regularly
- Take frequent breaks
- Reduce brightness if light sensitive
- Use lubricating eyedrops when advised
- Stop and rest if vision becomes uncomfortable
When Can You Read?
Reading can resume when comfortable.
Near tasks do not damage the ICL. However, reading may initially feel more difficult because of:
- Pupil dilation
- Temporary focusing changes
- Dryness
- Differences between the two eyes
- Presbyopia
- A distance-focused refractive target
Patients over approximately 40 may notice that they require reading glasses after their distance myopia has been corrected.
When Can You Shower or Wash Your Hair?
Many patients can shower from the following day, but direct water, soap and shampoo should be kept out of the eye during early healing.
A cautious approach includes:
- Keeping the eyes closed while washing the face
- Avoiding forceful water spray towards the eyes
- Dabbing the eyelids gently rather than rubbing
- Using a clean towel
- Avoiding contaminated water
The surgeon’s specific advice should take priority.
When Can You Wear Eye Makeup?
Eye makeup is usually avoided during the early recovery period to reduce the risk of contamination and accidental rubbing.
Many surgeons advise waiting at least approximately one week, and longer when:
- Redness persists
- The incision has not fully healed
- Inflammation remains
- Additional surgery is being considered
- The surgeon advises a longer restriction
Old or potentially contaminated eye cosmetics should be replaced.
When Can You Exercise?
Light walking is usually acceptable relatively soon after surgery.
Strenuous exercise should be postponed until the surgeon confirms that:
- Eye pressure is stable
- The incision is healing
- Inflammation is controlled
- There is no concern about the ICL position
During early recovery, avoid:
- Heavy lifting
- Intense straining
- High-impact exercise
- Activities that cause sweat to run into the eyes
- Exercises that risk accidental eye contact
A gradual return is safer than immediately resuming maximum-intensity training.
When Can You Swim?
Swimming pools, the sea, hot tubs and other recreational water can expose the healing eye to microorganisms and irritants.
Many surgeons advise avoiding swimming for at least one to two weeks, and sometimes longer depending on healing and the type of water exposure.
Do not resume swimming until the operating surgeon has confirmed that it is safe.
Goggles reduce water exposure but do not completely eliminate infection risk.
When Can You Resume Contact Sports?
Contact sports usually require a longer restriction than walking or light gym exercise.
Examples include:
- Boxing
- Martial arts
- Rugby
- Football
- Basketball
- Water polo
- Combat sports
The surgeon should consider:
- The stage of healing
- The risk of direct impact
- Whether one or both eyes were treated
- ICL position and vault
- Toric alignment
- Retinal risk from high myopia
- The type and intensity of sport
Even after complete recovery, protective eyewear is advisable whenever practical.
Can You Fly After ICL Surgery?
ICL surgery does not normally involve placing a gas bubble inside the eye, so the altitude restriction associated with retinal gas surgery does not generally apply.
However, flying immediately after surgery may be inadvisable because:
- Eye pressure needs early monitoring
- A next-day review is usually required
- Access to the operating surgeon may be limited
- Cabin air may worsen dryness
- An early complication could require urgent treatment
Travel should be discussed with the surgeon before surgery. It is generally more important to complete the early follow-up schedule than to leave the country immediately after the procedure.
Can You Sleep Normally?
Most patients can sleep in their usual position unless instructed otherwise.
The surgeon may recommend:
- Wearing an eye shield
- Avoiding pressure directly on the operated eye
- Sleeping with the head slightly elevated
- Avoiding face-down sleeping during the first few nights
The main purpose is to prevent accidental rubbing or pressure while asleep.
Should You Rub the Eye?
No.
The FDA patient booklet specifically advises avoiding eye rubbing during the early postoperative period.
Rubbing may:
- Irritate the corneal incision
- Transfer bacteria
- Increase inflammation
- Disturb the eye surface
- Place pressure on the eye
- Potentially affect toric alignment during early healing
If the eye feels itchy or gritty, use the prescribed lubricants or contact the clinic rather than rubbing.
Can the ICL Move During Recovery?
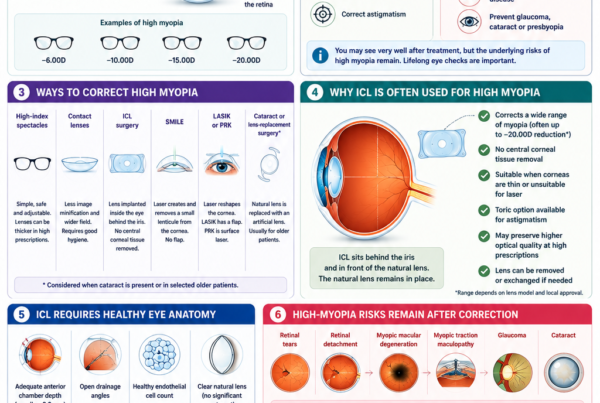
The ICL is positioned behind the iris and supported within the ciliary sulcus. It does not normally move with routine blinking, reading or normal eye movements.
However, uncommon positional problems can occur.
These include:
- Toric ICL rotation
- Incorrect vault
- Lens displacement
- Lens orientation problems
Symptoms may include:
- Vision becoming less clear after initially improving
- New ghosting
- Residual astigmatism
- Unequal vision between the eyes
- Glare or halos
- Unexpected pressure changes
An examination is required to determine whether symptoms are caused by the ICL, the tear film, residual prescription or another eye condition.
What Is Vault and Why Is It Checked?
Vault is the distance between the back of the ICL and the front of the natural crystalline lens.
An appropriate vault helps keep the ICL safely separated from the natural lens while avoiding excessive crowding of the front of the eye.
A Low Vault May Increase Concern About:
- Contact with the natural lens
- Anterior subcapsular cataract
- Reduced fluid circulation
- The need for closer observation or lens exchange
A High Vault May Increase Concern About:
- Narrow drainage angles
- Raised eye pressure
- Iris contact
- Pigment dispersion
- Inflammation
Vault can change over time as the pupil, ciliary body and natural lens change.
Research indicates that early postoperative vault measurements are useful, although vault may gradually decrease over the longer term.
What if a Small Prescription Remains?
A small residual prescription does not necessarily mean that the operation has failed.
Possible reasons include:
- The available ICL power
- Measurement variation
- Healing
- Toric alignment
- Corneal astigmatism
- Natural prescription change
- The surgeon deliberately targeting mild myopia
Management may include:
- No treatment when vision is satisfactory
- Spectacles for night driving or fine tasks
- Contact lenses
- Toric ICL repositioning
- ICL exchange
- Laser enhancement when the cornea is suitable
The prescription should be stable before enhancement is considered.
What if the Two Eyes Recover Differently?
It is common for one eye to be temporarily clearer than the other.
Possible reasons include:
- Different amounts of preoperative myopia
- Different levels of astigmatism
- One eye receiving a toric lens
- Differences in pupil dilation
- Mildly different corneal swelling
- Different tear-film quality
- Different healing responses
The difference should gradually reduce.
A persistent or increasing difference requires assessment for residual prescription, toric rotation, pressure differences, inflammation or another problem.
Does Toric ICL Recovery Differ?
The general recovery is similar.
However, a toric ICL must remain aligned with the intended astigmatic axis.
During follow-up, the surgeon may assess:
- Toric lens markings
- Rotational position
- Residual cylinder
- Visual clarity
- Vault
- Whether repositioning is needed
A small rotation may not affect vision significantly.
A larger rotation can reduce the astigmatism correction and cause:
- Blurred vision
- Ghosting
- Shadowing around letters
- Reduced night clarity
How Often Are Follow-Up Visits Needed?
The exact schedule varies.
A typical programme may include:
- A pressure check within the first several hours
- A review the next day
- A review approximately one week later
- A review at about one month
- Additional reviews at three to six months
- Regular long-term eye examinations
The EVO ICL patient information recommends continued examinations for as long as the lens remains implanted. These reviews should monitor eye pressure, cataract formation and corneal endothelial health.
Why Is Long-Term Follow-Up Necessary?
The ICL is designed to remain inside the eye long term, but the eye continues to age.
Regular examinations may assess:
- Vision and refraction
- ICL position
- Vault
- Toric alignment
- Eye pressure
- Drainage angles
- Corneal endothelial cell density
- The natural lens for cataract
- The retina and macula
- The optic nerve
Long-term follow-up can identify changes before they produce significant symptoms.
Can Cataract Develop After ICL Surgery?
Yes.
The natural lens remains inside the eye and can develop cataract as part of normal ageing.
Additional cataract risk may be influenced by:
- Increasing age
- Low vault
- Proximity between the ICL and the natural lens
- Surgical contact with the natural lens
- Individual anatomy
- Length of time since implantation
Modern central-port ICLs have shown favourable long-term outcomes, but cataract risk cannot be eliminated.
If visually significant cataract develops:
- The ICL is usually removed.
- The cloudy natural lens is removed.
- A cataract intraocular lens is implanted.
Can Eye Pressure Problems Develop Later?
Yes, although many pressure elevations occur early.
Later pressure problems may be associated with:
- Steroid response
- Excessive vault
- Narrow drainage angles
- Pigment dispersion
- Glaucoma developing independently
- Age-related anatomical changes
A review of pressure-related complications after ICL surgery emphasised that the cause must be identified because treatment differs depending on whether the pressure rise results from medication, retained viscoelastic, pupillary block, vault or angle changes.
Does ICL Surgery Remove the Risks of High Myopia?
No.
ICL surgery corrects the optical focusing error. It does not shorten the elongated eye.
Patients with high myopia remain at increased risk of:
- Retinal holes
- Retinal tears
- Retinal detachment
- Myopic macular degeneration
- Myopic traction maculopathy
- Glaucoma
- Cataract
Excellent unaided vision after surgery does not remove the need for retinal and optic nerve examinations.
Frequently Asked Questions About ICL Recovery
How Soon Will I See Clearly?
Many patients notice significantly clearer vision by the following day.
Some take several days or weeks to reach their best and most stable visual quality.
Is Blurred Vision Normal the Next Day?
Mild blur or fluctuation can be normal.
The vision should generally be improving. Sudden or progressive deterioration requires urgent review.
How Long Does the Incision Take to Heal?
The small corneal incision generally seals quickly and continues to heal over approximately one to two weeks.
How Long Will My Eye Feel Gritty?
Mild grittiness usually improves over the first few days.
Persistent or worsening discomfort should be assessed.
How Long Do Halos Last?
Halos may improve over weeks or months as the pupil settles and the brain adapts.
Some patients continue to notice mild halos during night driving.
Is Pain Normal?
Mild discomfort may occur.
Severe or increasing pain is not normal.
When Can I Return to Work?
Many patients return to office-based work within one to three days.
Physically demanding, dusty or hazardous work may require a longer break.
When Can I Drive?
Only after the surgeon confirms that vision is adequate and safe.
Do not drive on the day of surgery.
Can I Use My Phone After Surgery?
Yes, when comfortable.
Take breaks and use lubricating drops if screen use causes dryness or fluctuating vision.
When Can I Exercise?
Light activity may resume relatively early, but strenuous exercise should wait until the surgeon confirms that eye pressure and healing are satisfactory.
When Can I Swim?
Swimming should be avoided during early healing, commonly for at least one to two weeks or according to the surgeon’s instructions.
Can I Fly?
There is usually no gas-related altitude restriction, but early follow-up and access to urgent care must be considered.
Can I Rub My Eyes?
Avoid rubbing, particularly during the first several days.
Habitual vigorous eye rubbing should also be avoided long term.
Can the Lens Fall Out?
No.
The ICL is positioned inside the eye and cannot fall out like a contact lens.
Can the Lens Move?
Significant movement is uncommon, but toric rotation, inappropriate vault or displacement can occur.
What Happens if My Vision Is Still Blurry After One Month?
Possible causes include:
- Residual prescription
- Dry eye
- Toric rotation
- ICL power or position
- Vault
- Cataract
- Corneal irregularity
- Retinal or macular disease
An examination is needed before deciding whether treatment is required.
Will I Need Reading Glasses?
Possibly.
ICL surgery does not prevent presbyopia. Patients approaching or over 40 may still require reading glasses.
Do I Need Yearly Eye Examinations?
Yes.
Long-term monitoring should include eye pressure, the natural lens, endothelial cells, the retina and the ICL position.
Key Takeaway
Recovery after ICL surgery is usually relatively quick.
Many patients notice substantially clearer vision within the first day and return to office-based activities within a few days. Mild grittiness, watering, light sensitivity, fluctuating vision and halos can occur during early recovery.
However, clear vision does not mean that the eye has finished healing.
Early follow-up is essential to assess:
- Eye pressure
- Inflammation
- ICL position
- Vault
- Toric alignment
- Corneal healing
Use all prescribed eyedrops, avoid rubbing the eyes and follow the surgeon’s instructions regarding driving, exercise, swimming and contact sports.
Seek urgent eye care for severe pain, rapidly worsening vision, marked redness, significant light sensitivity, nausea, vomiting, a cloudy cornea, new flashes or floaters, or a curtain-like shadow across the vision.
Long-term examinations remain important because the ICL, eye pressure, corneal endothelial cells, natural lens, retina and optic nerve must continue to be monitored even when vision is excellent.
References
- US Food and Drug Administration. EVO and EVO+ Visian Implantable Collamer Lens Patient Information Booklet. 2022. FDA
- US Food and Drug Administration. EVO and EVO+ Visian Implantable Collamer Lens Instructions for Use. 2022. FDA
- Parkhurst G, et al. Three-Year Results From the United States FDA Prospective Multicentre Clinical Study of the EVO Implantable Collamer Lens. 2025. PubMed
- Albo C, et al. A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Refractive Outcomes in a United States Single-Centre Study. 2024. PubMed
- Gong D, et al. Causes and Management Strategies for Elevated Intraocular Pressure After Implantable Collamer Lens Implantation. 2024. PubMed Central
- Zhang H, et al. Analysis of Perioperative Problems Related to Intraocular Implantable Collamer Lens Implantation and Their Management. 2022. PubMed Central
- Chen X, et al. Long-Term Observation of Glare and Dynamic Pupil After EVO Implantable Collamer Lens Implantation. 2025. PubMed Central
- Alfonso-Bartolozzi B, et al. Ten-Year Follow-up of Posterior Chamber Phakic Intraocular Lenses With Central-Port Design. 2024. PubMed
- Nakamura T, et al. Posterior Chamber Phakic Intraocular Lens Implantation for Myopia and Myopic Astigmatism: A 10-Year Follow-up Study. 2019. PubMed
- Kim YH, et al. Long-Term Outcome and Related Risk Factors in Implantable Collamer Lens Surgery. 2025. PubMed
- Qin Q, et al. Pure ICL Implantation: Visual Recovery and Intraocular Pressure Outcomes. 2021. PubMed
- Martínez-Plaza E, et al. Inter-Eye and Postoperative Prediction of Vault After Implantable Collamer Lens Implantation. 2023. PubMed
- Alhamzah A, et al. Indications for Exchange or Explantation of Phakic Implantable Collamer Lenses With a Central Port. 2021. PubMed
- Zhang H, et al. Changes in Objective Dry-Eye Indicators After Implantable Collamer Lens Surgery. 2024. PubMed
- Imperial College Healthcare NHS Trust. Implantable Collamer Lens: Patient Information. NHS
- New York Eye and Ear Infirmary of Mount Sinai. What to Expect Before and After Refractive Surgery. NYEE