Gallery

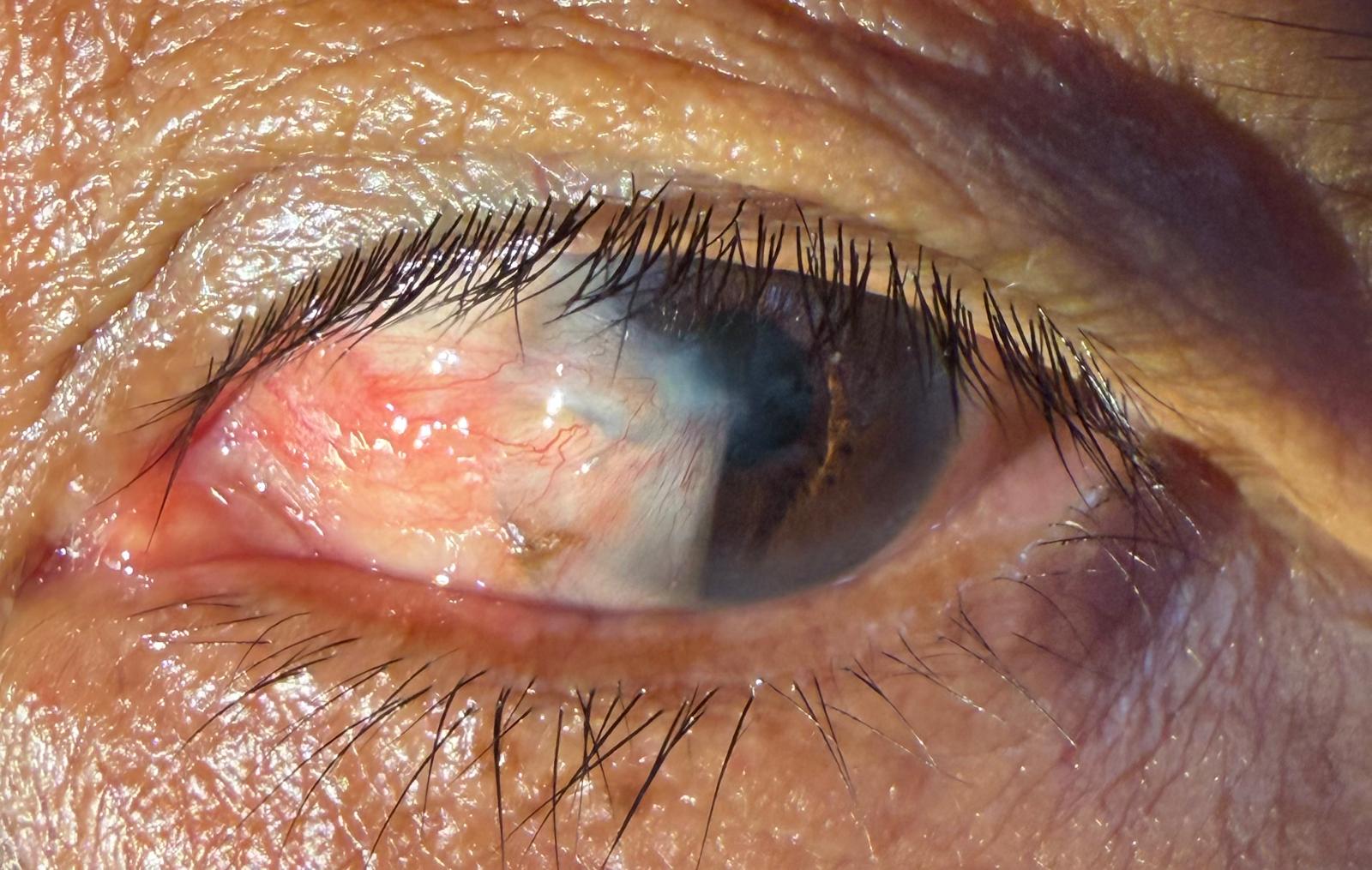
In a small village in rural Cambodia, we conducted a simple eye‑health screening and discovered that this gentle, elderly villager was living with a dense cataract and a pterygium. A pterygium is a fleshy, triangular growth that starts in the corner of the eye, often caused by long‑term exposure to sunlight and environmental irritation; though non‑cancerous, it can irritate the eye and eventually affect vision, and treatments range from eye drops to surgery. The cataract was more troubling: globally, cataracts and uncorrected refractive errors are the leading causes of vision impairment and blindness. Cataract surgery is straightforward and highly successful, yet about half of the people who need this surgery worldwide have no access to it. The burden is heaviest in low‑income countries, where vision impairment due to unoperated cataracts is significantly more common than in high‑income regions.
Standing in that village, I was struck by how something so easily treated elsewhere can still condemn people to darkness. The fact that vision loss from cataracts is largely preventable or treatable, yet 94 million people worldwide still live with distance vision impairment because of unaddressed cataracts, underscores the injustice of unequal access to care. Despite their hardships, the people we screened were deeply appreciative for the attention and hope we offered. Their gratitude reminded me how privileged I am to have the skills and resources to help restore sight. Being able to serve in places like this—where the difference between blindness and vision can hinge on a simple surgical procedure—has been one of the most humbling and rewarding experiences of my life.
In a remote corner of Nepal, I joined Dr Sanduk Ruit to run a cataract camp for people who would otherwise never see an eye specialist. Many of the patients had dense, advanced cataracts that would normally require expensive phacoemulsification machines. Instead, we used Dr Ruit’s modified manual small‑incision cataract surgery (SICS) technique—an efficient, low‑technology procedure in which a self‑sealing 6‑mm incision allows the cloudy lens to be removed and replaced with a PMMA intraocular lens. The British Journal of Ophthalmology reports that this manual SICS method can be performed in under five minutes, costs less than US $15 per case and achieves high‑volume, low‑complication cataract care in resource‑limited settings.
Over a few days we treated more than 300 patients. Working alongside Dr Ruit and his team was humbling—watching them restore sight so efficiently while keeping costs low is inspiring. The real reward came when the bandages came off: as CBS News describes, eyes and faces “light up with a quiet sort of joy and wonder” when people realise they can see again after years of darkness. That moment never gets old; witnessing lives transformed and being part of a team that makes such a profound difference is a privilege I will always cherish.



In Cambodia I had the privilege of working alongside Dr Paul Zhao and Dr David Lu from China and the Khmer Sight Foundation team. Over two days we treated more than 50 patients at a local eye camp. Dr Huot, the foundation’s medical director, and Chakmun travelled to rural villages ahead of our visit to identify people who needed surgery and prepared the facility so we could work efficiently. We were supported by a dedicated group of volunteers—anesthetists, optometrists, nurses and medical students—who provided translation and ensured patients felt at ease despite the language barrier.
Many of the people we saw had dense cataracts and severe pterygia. A pterygium is a raised, fleshy, triangular growth that starts in the corner of the eye; long‑term exposure to ultraviolet light is the main cause. Although it isn’t cancerous, a pterygium can grow across the cornea and obscure the pupil, leading to vision problems that sometimes require surgery. Hats and wraparound UV‑blocking sunglasses are recommended to protect against further damage and slow the growth of these lesions. Seeing so many advanced cases reminded us how vital it is to protect eyes from sun and dust and to treat pterygia before they progress.
We were able to offer high‑quality care thanks to generous donations from companies we regularly collaborate with, including Zeiss, Alcon and Baxter. Their support, combined with the tireless efforts of Khmer Sight Foundation staff and volunteers, allowed us to restore sight to dozens of people. Watching patients with bandaged eyes return the next day, full of gratitude and excitement as they saw clearly for the first time in years, was profoundly rewarding. I am thankful to have been part of such a collaborative, compassionate team and humbled by the opportunity to help transform lives.