Author: Dr Val Phua
Estimated reading time: 10–12 minutes
A Retinal Tear Can Threaten Vision Without Causing Pain
A retinal tear is a break in the thin, light-sensitive tissue lining the back of the eye.
Many retinal tears occur when the vitreous—the clear gel filling the eye—separates from the retina and pulls strongly enough to create a tear. Fluid can then pass through the opening and collect beneath the retina, potentially causing a retinal detachment.
A retinal tear does not always cause noticeable symptoms. When symptoms occur, they commonly include:
- A sudden increase in floaters
- Flashes of light
- Numerous small black dots resembling pepper
- Blurred vision
- A shadow or curtain entering the field of vision
Retinal tears and detachments are usually painless. Therefore, the absence of pain does not mean the problem is harmless. Sudden flashes, new floaters or a visual-field shadow require a prompt dilated retinal examination.
When a retinal tear is found and treated before the retina detaches, the outlook is generally excellent.
What Is the Retina?
The retina is a thin layer of nerve tissue lining the inside of the back of the eye.
It detects light and converts visual information into electrical signals that travel through the optic nerve to the brain.
The central part of the retina, known as the macula, provides the detailed vision required for:
- Reading
- Recognising faces
- Driving
- Seeing fine detail
The peripheral retina provides side vision and is where many retinal tears develop.
What Is a Retinal Tear?
A retinal tear forms when traction pulls the retina strongly enough to split it.
The most common type is a horseshoe or flap tear, in which the vitreous remains attached to a small flap of retina and continues pulling on it.
Other peripheral retinal abnormalities include:
- Operculated retinal holes
- Atrophic round holes
- Retinal dialysis
- Lattice degeneration
These lesions do not all carry the same risk. Their management depends on their appearance, symptoms, location, surrounding fluid and the patient’s individual risk factors.
Retinal Tear Versus Retinal Hole
The terms are sometimes used interchangeably, but they usually describe different mechanisms.
Retinal Tear
A retinal tear generally develops because the vitreous pulls on the retina.
Active traction may increase the risk of fluid passing beneath the retina and producing a detachment.
Retinal Hole
A retinal hole commonly develops from gradual thinning of the retina rather than active vitreous traction.
Atrophic holes are often smaller and usually carry a lower risk of retinal detachment. Some can be safely monitored, although treatment may still be recommended when other high-risk features are present.
Retinal Tear Versus Retinal Detachment
A retinal tear means that a break has formed in the retina, but the retina may still remain largely attached.
A retinal detachment occurs when fluid passes through the tear and separates the retina from the wall of the eye.
A tear may often be treated with laser or cryotherapy in the clinic. Once a significant detachment has developed, an operation may be required to reposition the retina.
Early diagnosis is therefore important: treating the tear may prevent the need for retinal-detachment surgery.
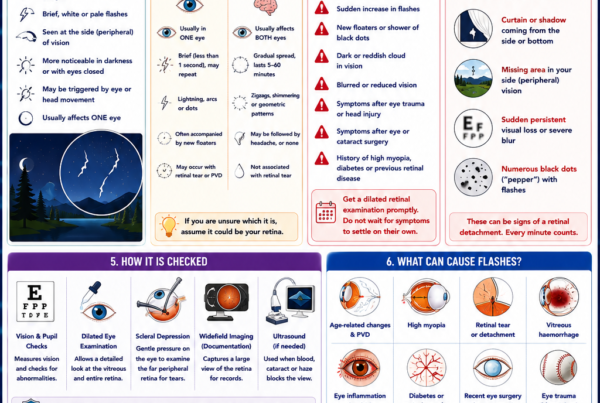
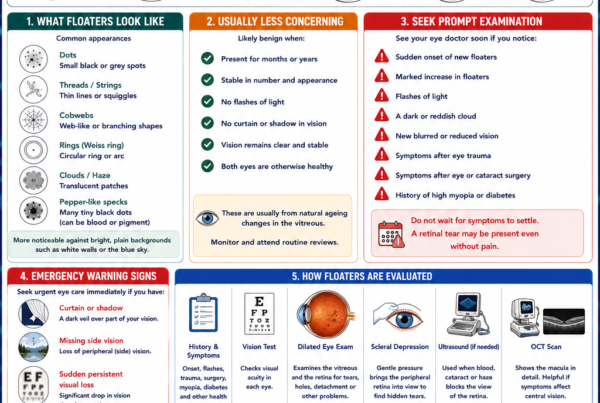
What Symptoms Can a Retinal Tear Cause?
A Sudden Increase in Floaters
Floaters may appear as:
- Dots
- Threads
- Cobwebs
- Rings
- Curved lines
- Small black specks
A sudden shower of numerous dark dots may resemble pepper being shaken across the vision. This may indicate pigment cells or blood released into the vitreous when the retina tears.
Longstanding stable floaters are common and are usually less concerning. The important change is the sudden appearance of new floaters or a marked increase in their number.
Flashes of Light
Flashes may appear as:
- Brief lightning streaks
- Camera-like flashes
- Flickering in the peripheral vision
- Arcs of light
They are often most noticeable in dim lighting or when the eyes or head move.
Flashes occur because mechanical pulling stimulates the retina. They may indicate an evolving posterior vitreous detachment, with or without a retinal tear.
Blurred or Hazy Vision
Blur may occur when:
- Blood enters the vitreous
- Numerous floaters obstruct vision
- A retinal detachment develops
- The macula becomes affected
A sudden visual reduction should be assessed urgently.
A Shadow or Curtain
A dark curtain, veil or shadow moving across the field of vision is particularly concerning for retinal detachment.
The shadow may begin from the side, above or below and gradually enlarge as more retina detaches.
This is a medical emergency. Prompt treatment gives the best opportunity to preserve vision.
No Symptoms
Some retinal tears are discovered incidentally during a dilated eye examination.
The absence of symptoms does not automatically determine whether treatment is needed. The ophthalmologist will consider the tear’s type, location, traction and other risk factors.
When Should I Seek Urgent Eye Care?
Arrange a prompt same-day dilated retinal examination if you notice:
- A sudden onset of new floaters
- A marked increase in existing floaters
- New flashes of light
- Numerous black dots or a “pepper shower”
- Sudden blurred vision
- A shadow, curtain or missing area of vision
- Symptoms following an eye injury
Do not wait to see whether the symptoms disappear.
A posterior vitreous detachment frequently occurs without a tear, but it is not possible to distinguish an uncomplicated vitreous detachment from a retinal tear based on symptoms alone. A dilated retinal examination is required.
In a large prospective study, approximately 9.9% of patients presenting with symptomatic posterior vitreous detachment had a retinal tear or rhegmatogenous retinal detachment at their initial assessment.
What Causes a Retinal Tear?
Posterior Vitreous Detachment
The vitreous is a clear gel filling the space between the lens and the retina.
When we are young, the vitreous is relatively firm and attached to the retinal surface. With age, it becomes more liquefied and gradually separates from the retina. This process is called a posterior vitreous detachment, or PVD.
A PVD often occurs without complication. However, if part of the vitreous is unusually firmly attached, it may pull hard enough to tear the retina during separation. Most spontaneous retinal tears occur in association with a PVD.
Eye Trauma
A direct impact may deform the eye and create retinal tears or retinal dialysis.
Possible causes include:
- A ball hitting the eye
- Contact sports
- Falls
- Road-traffic accidents
- Workplace injuries
- Blunt assault
- Penetrating injuries
Visual symptoms may occur immediately or appear later. A significant eye injury should therefore be examined even when central vision initially appears normal.
Retinal Thinning
Areas of retinal thinning, such as lattice degeneration, are more susceptible to developing holes or tears.
However, most people with lattice degeneration never develop a retinal detachment, and preventive treatment is not automatically required for every area of lattice.
Who Is at Greater Risk?
A retinal tear can occur without an obvious risk factor, but the likelihood is greater in people with:
- Increasing age
- Myopia, particularly high myopia
- Lattice degeneration
- Previous eye injury
- Previous retinal tear or detachment
- A family history of retinal detachment
- Previous eye surgery, including cataract surgery
- Certain inherited retinal or connective-tissue disorders
These factors increase risk but do not predict exactly who will develop a tear or when it will occur.
Why Does High Myopia Increase the Risk?
In myopia, the eye is usually longer from front to back.
As the eye elongates:
- The retina becomes more stretched.
- Areas of peripheral retinal thinning become more common.
- Posterior vitreous detachment may occur earlier.
- The lifetime risk of retinal tears and detachment increases.
People who previously had high myopia remain at increased retinal risk even after LASIK, SMILE or ICL surgery. These procedures correct the focusing error but do not shorten the eyeball.
Does Cataract Surgery Cause Retinal Tears?
Most patients undergo cataract surgery without retinal complications.
However, previous intraocular surgery is recognised as a risk factor for retinal tears and retinal detachment. The risk is influenced by factors such as:
- Age
- Axial length
- Degree of myopia
- Peripheral retinal condition
- Surgical complications
- The condition of the vitreous
New flashes, floaters or a visual-field shadow after cataract surgery require prompt retinal assessment rather than being assumed to be a normal postoperative effect.
How Is a Retinal Tear Diagnosed?
Dilated Retinal Examination
Dilating drops enlarge the pupil so that the ophthalmologist can examine the retina.
The assessment usually includes:
- Visual-acuity testing
- Pupil examination
- Slit-lamp examination
- Examination of the vitreous for pigment or blood
- Detailed inspection of the peripheral retina
Both eyes may be examined because retinal abnormalities or vitreous changes may be present in the other eye.
Scleral Depression
Scleral depression involves applying gentle pressure to the outside of the eyelid or eye while viewing the peripheral retina.
This brings the far peripheral retina into view and can reveal small tears that may otherwise be difficult to detect.
The examination may feel unusual or briefly uncomfortable but is important when a retinal tear is suspected.
Widefield Retinal Photography
Widefield imaging can document large areas of the peripheral retina and is useful for:
- Recording the tear’s location
- Monitoring surrounding laser treatment
- Comparing future examinations
- Patient education
However, retinal photography does not always show the entire far peripheral retina. It should not automatically replace a careful dilated examination with scleral depression when an acute tear is suspected.
Optical Coherence Tomography
OCT provides detailed cross-sectional images of the retina.
It is especially useful for examining the macula and detecting:
- Macular holes
- Epiretinal membranes
- Macular fluid
- Vitreomacular traction
Standard macular OCT is not the primary test for excluding a small peripheral retinal tear.
Ocular Ultrasound
Ultrasound may be required when the retina cannot be seen clearly because of:
- Vitreous haemorrhage
- Dense cataract
- Corneal opacity
- Severe inflammation
Ultrasound can help identify a retinal detachment, although a small tear may still be difficult to locate until the view improves.
Does Every Retinal Tear Need Treatment?
No.
Treatment depends on factors such as:
- Whether the tear is symptomatic
- Tear type and size
- Presence of persistent vitreous traction
- Location
- Fluid extending beneath the retina
- Lattice degeneration
- High myopia
- Previous detachment in either eye
- Planned or previous eye surgery
- Ability to attend follow-up
Symptomatic tractional tears are commonly treated because of their risk of progressing to retinal detachment.
Selected low-risk, asymptomatic holes or tears may be observed when there is no active traction or surrounding fluid.
The decision should be made after examining the retina rather than solely from the name of the lesion.
How Is a Retinal Tear Treated?
Laser Photocoagulation
Laser is the most commonly used treatment for an accessible retinal tear.
The ophthalmologist applies rows of small laser burns around the tear. These burns produce controlled scars that adhere the retina to the underlying tissue and create a barrier around the opening.
The laser does not physically close the tear like stitching fabric. Instead, it strengthens the adhesion surrounding the tear so that fluid is less likely to spread beneath the retina.
What Happens During Laser Treatment?
The procedure generally involves:
- Dilating the pupil.
- Applying anaesthetic eye drops.
- Placing a special contact lens on the eye.
- Directing laser spots around the retinal tear.
- Checking that the tear has been adequately surrounded.
Patients may see bright flashes during treatment. Some experience brief discomfort, particularly when treating the far peripheral retina.
Laser treatment is usually performed in the clinic and does not normally require a hospital stay.
Cryotherapy
Cryotherapy, or cryopexy, uses a freezing probe applied to the white outer wall of the eye over the tear.
The cold creates controlled inflammation and scarring around the retinal break, helping secure the retina to the wall of the eye.
Cryotherapy may be selected when:
- The tear is very peripheral.
- The view through the pupil is limited.
- Laser delivery is technically difficult.
- The clinical situation favours treatment from outside the eye.
Local anaesthesia is used. Patients may feel pressure or cold, and the eyelid may be temporarily swollen afterwards.
What If the Retina Has Already Detached?
Laser or cryotherapy alone may not be sufficient when significant fluid has already passed beneath the retina.
Retinal-detachment surgery may involve:
- Pneumatic retinopexy
- Scleral buckle surgery
- Vitrectomy
- Laser or cryotherapy combined with surgery
The appropriate procedure depends on the tear’s position, the extent of detachment, whether the macula is involved and other features of the eye.
What Should I Expect After Retinal Laser?
Immediately after treatment, you may experience:
- Blurred vision from dilating drops
- Temporary dazzle from the laser
- Mild discomfort
- A dull ache
- Increased awareness of existing floaters
Arrange for someone to accompany you or drive you home if your vision is blurred.
Your ophthalmologist may recommend temporarily avoiding:
- Vigorous exercise
- Heavy lifting
- Contact sports
- Activities involving significant eye trauma
Restrictions vary according to the tear, amount of laser treatment and whether there is associated haemorrhage or retinal detachment. Follow the instructions given for your particular eye.
Will Laser Remove My Floaters and Flashes?
Not usually.
Laser treats the retinal tear but does not remove vitreous opacities.
Floaters may remain visible, although many become less noticeable over time as:
- The brain adapts to them.
- They move away from the visual axis.
- Blood or pigment gradually clears.
Flashes commonly become less frequent as the vitreous separation settles. However, a new increase in flashes or floaters requires repeat examination.
Can a Retinal Tear Occur After Successful Laser Treatment?
Yes.
Laser substantially reduces the risk of the treated tear progressing, but it cannot prevent:
- A new tear elsewhere
- Further vitreous separation
- Retinal detachment from another break
- Trauma-related retinal damage
Continued monitoring remains important, and any new symptoms should be assessed promptly even if the original tear was successfully treated.
How Often Will I Need Follow-Up?
The follow-up schedule depends on:
- The type and size of tear
- Whether treatment was performed
- Presence of vitreous haemorrhage
- Degree of ongoing vitreous traction
- High myopia or lattice degeneration
- Symptoms
- Findings in the other eye
A follow-up examination allows the ophthalmologist to confirm that the treatment adequately surrounds the tear and to look for new breaks.
Do not wait for the scheduled appointment if you develop:
- More flashes
- A sudden increase in floaters
- Blurred or reduced vision
- A new shadow or curtain
Can Retinal Tears Be Prevented?
Many retinal tears occur naturally as the vitreous separates with age and cannot be completely prevented.
You can reduce avoidable risk by:
- Wearing protective eyewear during high-risk sports or work
- Seeking assessment after significant eye trauma
- Attending recommended dilated retinal examinations
- Recognising flashes, floaters and curtains as warning symptoms
- Seeking prompt care rather than waiting for symptoms to resolve
People with high myopia, lattice degeneration or previous retinal tears should follow the review schedule recommended by their ophthalmologist.
Frequently Asked Questions
Is a retinal tear an emergency?
A suspected retinal tear requires prompt assessment because it may progress to retinal detachment.
Sudden flashes, new floaters or numerous black dots should be examined urgently. A curtain, shadow or reduced vision requires immediate eye care.
Does a retinal tear cause pain?
Usually not.
Retinal tears and detachments are generally painless, which is why new visual symptoms should never be ignored simply because the eye feels comfortable.
Can a retinal tear heal by itself?
Some low-risk tears or holes develop surrounding pigmentation or adhesion and may remain stable without treatment.
However, it is not safe to assume that a new tear will heal on its own. The retina must first be examined to determine its risk.
Is retinal laser painful?
Anaesthetic drops are used. Many patients experience only bright flashes and mild discomfort, although treatment of very peripheral tears can be more uncomfortable.
How long does retinal laser take?
The laser itself is often completed within a relatively short clinic procedure, but additional time is needed for pupil dilation, examination and post-treatment checks.
Can I fly after retinal laser?
Retinal laser alone does not usually involve a gas bubble, but travel advice depends on the clinical condition.
Air travel is prohibited when certain intraocular gas bubbles are present after retinal surgery. Confirm with your ophthalmologist before travelling.
Can I exercise after retinal laser?
Your doctor may advise temporary restriction of strenuous exercise or heavy lifting. The duration depends on the tear, treatment and associated findings.
Can I drive after treatment?
Vision may be blurred from dilating drops and bright laser exposure. Do not drive until vision has recovered sufficiently and your ophthalmologist considers it safe.
Can retinal laser damage my vision?
Laser intentionally creates small peripheral retinal scars. Serious complications are uncommon when treatment is appropriately performed, but no procedure is entirely risk-free.
The risk of treatment is weighed against the potentially greater risk of retinal detachment.
Will I need laser in both eyes?
Only retinal lesions considered to require treatment are lasered.
Having a tear in one eye does not automatically mean the other eye should be treated, but both eyes should be examined.
The Bottom Line
A retinal tear is a break in the retina, most commonly caused when the vitreous gel separates and pulls on the peripheral retina.
Warning symptoms include:
- Sudden new floaters
- Flashes of light
- A shower of black dots
- Blurred vision
- A shadow or curtain
These symptoms require prompt dilated retinal examination because an uncomplicated posterior vitreous detachment cannot be reliably distinguished from a retinal tear based on symptoms alone.
When a high-risk tear is found before the retina detaches, laser or cryotherapy can create a protective scar around it and significantly reduce the chance of progression.
Treatment does not eliminate all future risk. New tears may develop elsewhere, so continued monitoring and awareness of warning symptoms remain essential.
Sudden flashes and floaters should be checked promptly. A curtain, shadow or loss of vision is an emergency.
References
- Kim SJ, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern. Ophthalmology. 2025.
- American Society of Retina Specialists. Retinal Tears.
- National Eye Institute. Vitreous Detachment. Updated December 2024.
- National Eye Institute. Laser Surgery and Freeze Treatment for Retinal Tears. Updated December 2024.
- National Eye Institute. Retinal Detachment. Updated November 2025.
- Nixon TRW, et al. Posterior Vitreous Detachment and Retinal Tear: A Prospective Study of Community Referrals. Eye. 2023.