Author: Dr Val Phua
Estimated reading time: 10–12 minutes
Retinal Detachment Is a Medical Emergency
A retinal detachment occurs when the retina separates from its normal position along the back wall of the eye.
The retina is the light-sensitive tissue responsible for converting light into signals that travel through the optic nerve to the brain. Once detached, it cannot function normally and may become permanently damaged if treatment is delayed.
Common warning symptoms include:
- A sudden increase in floaters
- Flashes of light
- A dark shadow or curtain in the vision
- Loss of peripheral vision
- Sudden blurred or reduced vision
Retinal detachment is usually painless. The absence of pain does not mean that it is safe to wait.
If you notice a curtain, shadow or missing area of vision, arrange an urgent ophthalmic assessment immediately. Early treatment can prevent the detachment from spreading and offers the best chance of preserving sight.
What Is the Retina?
The retina is a thin layer of specialised nerve tissue lining the inside of the back of the eye.
It receives light focused through the cornea and lens and converts it into electrical signals.
The centre of the retina is called the macula. It provides the detailed central vision needed for:
- Reading
- Recognising faces
- Driving
- Seeing colour
- Performing fine visual tasks
The remainder of the retina provides peripheral or side vision.
When part of the retina detaches, the corresponding area of vision may become blurred, dark or absent.
What Is a Retinal Detachment?
The retina normally lies against the underlying tissues that supply it with oxygen and nutrients.
A detachment occurs when the retina lifts away from this supporting layer—similar to wallpaper peeling away from a wall.
The detached retina begins to function poorly. If the detachment spreads towards the macula, central vision may be permanently affected even after successful surgery.
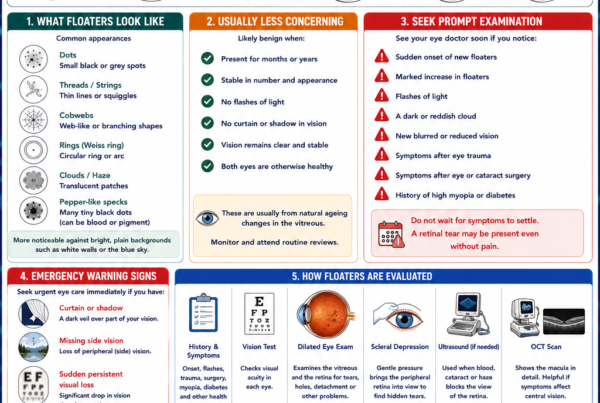
What Symptoms Should I Watch For?
Sudden New Floaters
Floaters may appear as:
- Black dots
- Threads
- Cobwebs
- Curved lines
- Rings
- A shower of small specks
A few longstanding floaters are common. The more concerning symptom is a sudden onset or marked increase in floaters.
Numerous pepper-like dots may represent pigment or blood released when the retina tears.
Flashes of Light
Flashes may appear as:
- Lightning streaks
- Arcs of light
- Camera-like flashes
- Flickering in the side vision
They often occur when the vitreous gel inside the eye pulls on the retina.
Flashes alone do not prove that a detachment is present, but they require examination because the same process may create a retinal tear.
A Curtain, Veil or Shadow
A dark curtain or shadow moving across the vision is one of the classic symptoms of retinal detachment.
It may begin:
- From one side
- From above
- From below
- As a missing patch of peripheral vision
The shadow may progressively move towards the centre as more retina detaches.
This requires emergency eye assessment.
Sudden Blurred or Reduced Vision
Vision may become blurred because:
- The macula has detached.
- Blood has entered the vitreous.
- Numerous floaters obstruct the visual axis.
- A large area of retina is no longer functioning.
Persistent visual reduction should never be attributed automatically to ordinary floaters.
No Symptoms
A small peripheral detachment may occasionally cause no noticeable symptoms and be discovered during a dilated retinal examination.
This is one reason regular retinal examinations are important for selected high-risk patients.
What Is the Difference Between a Retinal Tear and a Retinal Detachment?
A retinal tear is a break in the retinal tissue.
At this stage, the surrounding retina may still be attached. Laser or cryotherapy can often create a protective scar around the tear and prevent fluid from spreading underneath it.
A retinal detachment occurs when fluid has already passed through a tear and lifted the retina away from the wall of the eye.
Once a significant detachment has developed, laser around the tear alone is usually insufficient. Surgery is generally required to reposition the retina.
The Three Main Types of Retinal Detachment
Rhegmatogenous Retinal Detachment
This is the most common type.
“Rhegmatogenous” means that a retinal break, hole or tear is present.
The process usually occurs as follows:
- The vitreous gel becomes more liquefied with age.
- The vitreous separates from the retina.
- Persistent traction creates a retinal tear.
- Fluid passes through the tear.
- The fluid collects beneath the retina and lifts it away.
Risk factors include high myopia, lattice degeneration, previous cataract surgery, trauma and a previous retinal detachment.
Tractional Retinal Detachment
A tractional detachment occurs when scar tissue on the surface of the retina contracts and physically pulls the retina away from the back of the eye.
It may develop in:
- Proliferative diabetic retinopathy
- Retinal vein occlusion
- Retinopathy of prematurity
- Previous inflammation or infection
- Other conditions that cause retinal scarring
Unlike a rhegmatogenous detachment, there may initially be no retinal tear.
Diabetic retinopathy is the most common cause of tractional retinal detachment.
Exudative Retinal Detachment
An exudative or serous detachment occurs when fluid leaks beneath the retina without a retinal break.
Possible causes include:
- Inflammation inside the eye
- Abnormal or leaking blood vessels
- Eye injury
- Certain tumours
- Severe hypertension-related disease
- Age-related macular degeneration
- Coats disease
Treatment is directed mainly at the underlying cause rather than simply sealing a retinal tear.
Who Is at Greater Risk?
Anyone can develop a retinal detachment, but risk is increased by:
- High myopia
- Increasing age
- Lattice degeneration
- Previous retinal tear or detachment
- Retinal detachment in the other eye
- Family history of retinal detachment
- Previous cataract or other intraocular surgery
- Significant eye trauma
- Diabetic retinopathy
- Certain inherited eye or connective-tissue disorders
Regular monitoring does not prevent every detachment, but it may detect retinal tears or suspicious peripheral changes before central vision is affected.
Why Does High Myopia Increase the Risk?
A highly myopic eye is usually longer than average.
As the eye elongates:
- The retina becomes stretched.
- Peripheral retinal thinning becomes more common.
- Lattice degeneration may develop.
- Vitreous separation may occur at a younger age.
- Retinal tears and detachment become more likely.
LASIK, SMILE, PRK or ICL surgery correct the focusing error but do not shorten the eyeball. A person who previously had high myopia therefore retains the associated retinal risk.
Can Cataract Surgery Cause Retinal Detachment?
Most patients undergo cataract surgery without retinal complications.
However, previous cataract surgery is a recognised risk factor for rhegmatogenous retinal detachment, particularly in younger patients and those with long, highly myopic eyes.
New flashes, floaters or a visual-field shadow after cataract surgery require prompt retinal examination and should not be dismissed as part of normal recovery.
Can Eye Trauma Cause a Detachment?
Yes.
A blunt impact can temporarily deform the eye, creating a retinal tear or retinal dialysis. A penetrating injury can directly damage the retina.
Examples include:
- A ball striking the eye
- Contact sports
- Falls
- Workplace injuries
- Road-traffic accidents
- Assault
- Penetrating foreign bodies
Retinal damage may be detected immediately or develop later. Significant eye trauma should therefore be evaluated even when initial central vision seems relatively good.
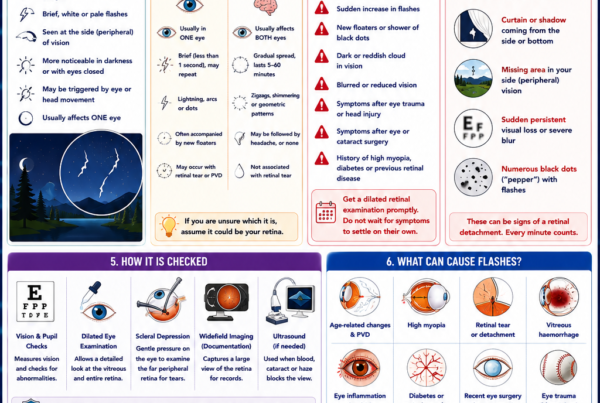
How Is Retinal Detachment Diagnosed?
Dilated Retinal Examination
Dilating drops enlarge the pupil so that the retina can be examined carefully.
The ophthalmologist assesses:
- The extent and location of the detachment
- The retinal tear or tears
- Whether the macula is still attached
- Vitreous traction
- Bleeding inside the eye
- Lattice degeneration
- The condition of the other eye
Scleral depression may be used to bring the far peripheral retina into view. It may feel uncomfortable but helps identify small or multiple breaks.
Optical Coherence Tomography
OCT produces detailed cross-sectional images of the retina.
It is particularly helpful for determining whether fluid has reached the macula and for assessing the retinal layers after surgery.
Widefield Retinal Photography
Widefield imaging documents the extent of the detachment and the location of tears.
However, photography may not show the entire far peripheral retina and does not replace a careful clinical examination when an acute detachment is suspected.
Ocular Ultrasound
Ultrasound may be required when the retina cannot be seen directly because of:
- Vitreous haemorrhage
- Dense cataract
- Corneal opacity
- Severe inflammation
It can identify whether the retina is detached and provide information about the shape and extent of the detachment.
What Does “Macula-On” or “Macula-Off” Mean?
Macula-On Retinal Detachment
A macula-on detachment means that the central retina remains attached.
Central vision may still be relatively good even though a curtain or shadow is affecting the peripheral field.
The main objective is to repair the detachment before it reaches the macula. These cases are generally prioritised urgently because preserving an attached macula usually provides a better visual prognosis.
Macula-Off Retinal Detachment
A macula-off detachment means that fluid has already spread beneath the central retina.
Central vision is usually blurred or markedly reduced.
Successful surgery can improve vision, but the final result may not return to its previous level because the macular photoreceptors have already been separated from their supporting tissues.
Earlier repair of a recent macula-off detachment is generally associated with better visual outcomes than prolonged delay, although the exact timing is individualised according to the detachment and the patient’s clinical situation.
How Urgently Is Surgery Needed?
Every suspected retinal detachment requires urgent assessment.
The operation may be performed immediately, within 24 hours or within the following few days depending on:
- Whether the macula is attached
- How quickly the detachment is progressing
- Location and number of tears
- Duration of symptoms
- Presence of proliferative vitreoretinopathy
- Whether the other eye sees well
- The type of detachment
- Medical and anaesthetic considerations
Patients should not delay assessment in an attempt to judge urgency themselves. The timing decision can only be made after examining the retina.
How Is Retinal Detachment Treated?
The purpose of surgery is to:
- Identify and seal every retinal break.
- Relieve traction on the retina.
- Drain or displace fluid beneath the retina.
- Reposition the retina against the wall of the eye.
- Hold it in place while healing occurs.
The main surgical options are pneumatic retinopexy, scleral buckle and vitrectomy. Some patients require a combination.
Pneumatic Retinopexy
Pneumatic retinopexy involves injecting a gas bubble into the eye.
The patient holds their head in a specific position so that the bubble presses against the retinal tear. The tear is then sealed with laser or cryotherapy.
It is most suitable for selected uncomplicated detachments with tears in favourable locations.
Advantages may include:
- Clinic-based treatment in selected cases
- Smaller procedure
- Faster initial recovery
- Less change to the eye’s external shape
However, it requires strict positioning and is not suitable for every tear pattern. Additional laser or surgery may be needed if the retina does not remain attached.
Scleral Buckle Surgery
A scleral buckle is a soft silicone band placed around part or all of the outside of the eye.
The buckle gently indents the eye wall towards the retinal tear, reducing vitreous traction and helping the retinal surfaces meet.
Cryotherapy is often used to seal the tear, and fluid beneath the retina may be drained.
The buckle usually remains permanently in place. It is not normally visible from the outside.
Scleral buckling may be particularly useful in:
- Younger phakic patients
- Detachments with selected peripheral breaks
- Retinal dialysis
- Certain detachments without extensive vitreous complexity
The procedure may change the spectacle prescription, often making the eye more myopic.
Vitrectomy
Vitrectomy is now commonly used for retinal-detachment repair.
Small instruments are inserted through the white part of the eye to:
- Remove the vitreous gel
- Release traction
- Drain subretinal fluid
- Flatten the retina
- Apply laser around retinal tears
- Insert a gas bubble or silicone oil
The internal bubble supports the retina while laser scars form around the breaks.
Vitrectomy may be preferred when there are:
- Multiple or posterior retinal tears
- Vitreous haemorrhage
- A large or complex detachment
- Proliferative vitreoretinopathy
- Previous cataract surgery
- Significant vitreous traction
- Giant retinal tears
- Associated macular or vitreous disease
Combined Surgery
Some detachments are best treated with both a scleral buckle and vitrectomy.
The buckle supports the peripheral retina externally, while vitrectomy relieves internal traction and allows direct treatment of the breaks.
The choice depends on retinal anatomy rather than one procedure being universally superior.
Gas Bubble Versus Silicone Oil
Gas Bubble
Gas gradually dissolves and is replaced by the eye’s natural fluid.
While gas remains in the eye:
- Vision is significantly blurred.
- A moving horizontal line may be visible as the bubble shrinks.
- Head positioning may be required.
- Flying and significant altitude changes are prohibited.
- Nitrous oxide anaesthesia must be avoided.
Reduced atmospheric pressure causes the gas to expand and can produce a dangerous rise in eye pressure. Nitrous oxide can also rapidly enlarge an intraocular gas bubble. Flying and nitrous oxide must be avoided until the treating ophthalmologist confirms that the bubble has completely disappeared.
Silicone Oil
Silicone oil may be used for more complex detachments or when longer-term internal support is required.
Unlike gas, it does not dissolve by itself and may require a second operation for removal.
Silicone oil may be chosen when:
- Proliferative vitreoretinopathy is present
- The detachment is complex
- Long-term tamponade is required
- Postoperative positioning may be difficult
- Air travel cannot be avoided
- The eye has suffered severe trauma
Silicone oil can be associated with cataract, raised eye pressure, corneal complications and emulsification.
Why Is Head Positioning Required?
The gas or oil bubble floats to the highest part of the eye.
Positioning places the bubble against the retinal tear so that it supports the correct area while healing occurs.
Depending on the tear location, patients may be asked to:
- Look down
- Lie on one side
- Avoid lying on their back
- Maintain a face-down posture for specified periods
Not every operation requires face-down positioning. Follow the surgeon’s exact instructions rather than general advice from another patient.
What Should I Expect After Surgery?
Common early symptoms include:
- Blurred vision
- Mild to moderate discomfort
- Redness
- Eyelid swelling
- Watering
- A gritty sensation
- Temporary double vision
- Awareness of a gas bubble
Prescription drops commonly include antibiotics, steroids and pupil-dilating medication.
Vision may take weeks or months to improve, particularly if the macula was detached.
What Activities Should I Avoid?
Restrictions vary, but patients may temporarily be advised to avoid:
- Heavy lifting
- Strenuous exercise
- Contact sports
- Swimming
- Eye rubbing
- Driving
- Air travel when gas is present
- Mountain travel or major altitude changes with gas
- Scuba diving with gas
- Sleeping in certain positions
Follow the individual postoperative instructions because the tear location, procedure and internal tamponade differ between patients.
When Can I Drive Again?
Do not drive while:
- Vision is significantly reduced.
- A gas bubble obstructs vision.
- Dilating drops are active.
- Double vision is present.
- You cannot meet the legal driving-vision standard.
- Your surgeon has not cleared you.
Even when visual acuity improves, peripheral vision and depth perception may remain temporarily affected.
How Successful Is Retinal-Detachment Surgery?
Modern retinal-detachment treatment is anatomically successful in approximately nine out of ten patients overall, although some eyes require more than one operation.
Anatomical success means that the retina is reattached. It does not guarantee that vision will return to its pre-detachment level.
What Determines the Final Vision?
Visual recovery depends on:
- Whether the macula detached
- Duration of macular detachment
- Vision before surgery
- Size and complexity of the detachment
- Presence of proliferative vitreoretinopathy
- Retinal tears and trauma
- Other macular or optic-nerve disease
- Surgical complications
- Age and healing response
When the macula remains attached, vision often remains close to its preoperative level. If the macula was detached, vision usually improves following successful repair but some permanent reduction or distortion may remain.
Why Can Vision Remain Distorted After Successful Surgery?
Even after the retina is anatomically reattached, patients may notice:
- Wavy lines
- Objects appearing smaller or larger
- Reduced contrast
- Colour differences
- Distortion
- Poorer night vision
- A persistent missing patch
Possible causes include:
- Previous macular detachment
- Photoreceptor damage
- Residual subretinal fluid
- Epiretinal membrane
- Retinal displacement
- Macular swelling
- Other pre-existing retinal disease
Visual improvement may continue gradually over many months.
Can the Retina Detach Again?
Yes.
Re-detachment may occur because of:
- A new retinal tear
- An inadequately sealed break
- Scar-tissue contraction
- Proliferative vitreoretinopathy
- Trauma
- Incomplete healing
New flashes, floaters, shadows or visual reduction after surgery require prompt assessment.
What Is Proliferative Vitreoretinopathy?
Proliferative vitreoretinopathy, or PVR, is the formation and contraction of scar tissue on or beneath the retina.
The scar tissue can:
- Wrinkle the retina
- Reopen retinal tears
- Create new traction
- Prevent the retina from lying flat
- Cause recurrent detachment
PVR is an important cause of complex retinal detachment and may require further vitrectomy, membrane removal, scleral buckling or silicone-oil tamponade.
Possible Complications of Surgery
Potential complications include:
- Cataract progression
- Raised or reduced eye pressure
- Infection
- Bleeding
- Recurrent retinal detachment
- PVR
- Macular swelling
- Epiretinal membrane
- Double vision
- Refractive changes
- Corneal damage
- Loss of vision
The risks of surgery are weighed against the much greater risk of permanent visual loss from leaving a detachment untreated.
Can Retinal Detachment Be Prevented?
Not every detachment can be prevented.
Risk may be reduced by:
- Recognising sudden flashes and floaters
- Seeking examination promptly
- Treating high-risk retinal tears
- Wearing protective eyewear during hazardous work or sport
- Attending recommended retinal examinations
- Maintaining good diabetic control
- Seeking assessment after significant eye trauma
Regular examinations are especially important for patients with high myopia, previous retinal tears or detachment, significant lattice degeneration or retinal disease in the other eye.
Frequently Asked Questions
Is retinal detachment painful?
Usually not.
Retinal detachment affects the light-sensitive retina and commonly produces visual symptoms without pain.
Can a detached retina heal by itself?
A true retinal detachment does not normally reattach permanently without treatment.
A small, localised detachment may occasionally be surrounded with laser, but most significant detachments require surgery.
Can retinal laser repair an established detachment?
Laser can seal retinal tears and may wall off selected small detachments.
Once a large amount of fluid has lifted the retina, surgery is usually required to reposition it.
Will surgery restore all my vision?
Not always.
The best outcomes occur when the macula remains attached. When central vision was already affected, surgery aims first to reattach the retina and prevent further loss; visual improvement may be incomplete.
Will my floaters disappear after surgery?
Vitrectomy removes much of the vitreous and may reduce floaters. However, new visual phenomena can arise from gas, residual vitreous, blood or postoperative changes.
How long will the gas bubble remain?
The duration depends on the type and concentration of gas. Some bubbles disappear within weeks, while longer-acting gases may remain for several weeks or occasionally longer. Your surgeon will advise when it has completely resolved.
Can I fly with a small gas bubble remaining?
No.
Even a small bubble may expand at altitude. Do not fly until your ophthalmologist confirms that the bubble is completely gone.
Can I have general anaesthesia with a gas bubble?
Inform every doctor, dentist and anaesthetist that there is gas inside your eye.
Nitrous oxide—sometimes called laughing gas—must not be used while an intraocular gas bubble remains because it may cause dangerous expansion and pressure elevation.
Does a previous detachment increase the risk in the other eye?
Yes.
The other eye may share risk factors such as high myopia, lattice degeneration or abnormal vitreoretinal adhesions. It should be examined and monitored as advised.
The Bottom Line
Retinal detachment is a medical emergency in which the retina separates from the back wall of the eye.
Warning signs include:
- Sudden new floaters
- Flashes of light
- A shower of black dots
- A curtain or shadow
- Sudden blurred or missing vision
The most common form begins with a retinal tear that allows fluid beneath the retina. Treatment may involve pneumatic retinopexy, scleral buckle surgery, vitrectomy or a combination of procedures.
The final visual outcome depends heavily on whether the macula remains attached and how long it has been detached.
Do not wait for pain. Do not wait for the curtain to reach the centre. Sudden flashes, floaters or a visual-field shadow require urgent dilated retinal examination.
References
- National Eye Institute. Retinal Detachment. Updated November 2025.
- American Society of Retina Specialists. Retinal Detachment.
- National Eye Institute. Types and Causes of Retinal Detachment. Updated December 2024.
- National Eye Institute. Surgery for Retinal Detachment. Updated December 2024.
- Wiedemann P, et al. When to Repair a Retinal Detachment? International Journal of Retina and Vitreous. 2024.
- Sothivannan A, et al. Impact of Time to Surgery on Visual Outcomes for Rhegmatogenous Retinal Detachment. American Journal of Ophthalmology. 2022.
- Xiong J, et al. A Review of Rhegmatogenous Retinal Detachment: Past, Present and Future. 2025.
- Yan X, et al. Surgical Managements for Rhegmatogenous Retinal Detachment: A Network Meta-analysis. 2024.