Author: Dr Val Phua
Estimated reading time: 11–13 minutes
What Are the Spots, Threads and Cobwebs Moving Across My Vision?
Eye floaters are small shapes that appear to drift through the field of vision.
They may look like:
- Black or grey dots
- Threads or strings
- Cobwebs
- Curved lines
- Rings
- Translucent clouds
- Small insects moving across the vision
Floaters are particularly noticeable when looking at a bright, plain background, such as a white wall, computer screen or clear sky.
Most longstanding floaters are caused by natural changes in the vitreous gel inside the eye and are not dangerous. However, a sudden onset or marked increase in floaters may indicate a posterior vitreous detachment, retinal tear, vitreous haemorrhage or retinal detachment.
Seek prompt dilated retinal examination if new floaters are accompanied by:
- Flashes of light
- A shower of black dots
- Blurred or reduced vision
- A dark curtain or shadow
- Recent eye trauma
Retinal tears and detachments are usually painless, so the absence of discomfort does not make sudden floaters safe to ignore.
What Causes a Floater to Appear?
The inside of the eye is filled with a transparent gel called the vitreous humour.
When we are young, the vitreous is relatively uniform and firmly attached to the retina. With age, it gradually becomes more liquefied and develops microscopic fibres or condensations.
These structures cast shadows onto the retina. The brain perceives the shadows as floaters.
The floater is therefore not normally located on the front surface of the eye. It lies within the vitreous cavity and moves when the eye moves.
Because the vitreous continues moving briefly after the eye stops, floaters may seem to drift away when you try to look directly at them.
Why Are Floaters Easier to See Against a Bright Background?
A uniform bright background creates strong contrast between the incoming light and the shadow cast by the vitreous opacity.
Floaters may therefore appear more obvious when looking at:
- A bright sky
- A white wall
- A blank document
- A computer screen
- A brightly lit room
They may be less noticeable in dim lighting or against a visually complex background.
This does not necessarily mean that the number of floaters is changing throughout the day.
What Do Ordinary Floaters Look Like?
Common age-related floaters may appear as:
Small Dots
These may be grey, black or translucent and move with the eye.
Threads or Cobwebs
Fine vitreous fibres may create curved or branching shadows.
Rings
A relatively large circular floater may appear after the vitreous separates from the optic nerve.
This is often called a Weiss ring and commonly occurs during posterior vitreous detachment.
Clouds or Haze
A cluster of vitreous opacities may create a translucent patch that moves across the vision.
A new dark or reddish cloud is more concerning because it may represent blood inside the eye.
What Is Posterior Vitreous Detachment?
Posterior vitreous detachment, or PVD, occurs when the vitreous gel separates from the retina.
This is a common age-related event and usually happens after the vitreous has become increasingly liquefied.
Typical symptoms include:
- Sudden new floaters
- A larger ring-shaped floater
- Flashes in the side vision
- Temporary visual haze
Most PVDs do not cause permanent visual damage. The American Society of Retina Specialists reports that approximately 85% of patients with PVD do not develop a significant complication, and the flashes and floaters often become less noticeable over the following months.
However, PVD can occasionally pull hard enough to tear the retina. For this reason, sudden floaters cannot be safely diagnosed as an uncomplicated PVD based on symptoms alone.
How Can a PVD Cause a Retinal Tear?
The vitreous is more firmly attached to certain areas of the retina.
As it separates, persistent traction may:
- Pull on the peripheral retina.
- Create a retinal tear.
- Rupture a small retinal blood vessel.
- Allow fluid to pass beneath the retina.
- Lead to a retinal detachment.
A large prospective community study found a retinal tear or rhegmatogenous retinal detachment in approximately 9.9% of patients presenting with symptomatic PVD. A further 3% developed a retinal tear during the following two months. Some tears were detected only through careful indirect examination with scleral depression.
These findings explain why an initial dilated examination—and follow-up in selected patients—remains important.
What Symptoms Suggest a Retinal Tear?
Warning symptoms include:
- A sudden onset of numerous floaters
- A dramatic increase in existing floaters
- A shower of pepper-like black dots
- New flashes of light
- A dark cloud or haze
- Reduced or blurred vision
The pepper-like dots may represent pigment cells or blood released when the retina tears.
A retinal tear can frequently be treated with laser or cryotherapy before it progresses to a detachment.
What Symptoms Suggest Retinal Detachment?
Seek emergency eye care if you notice:
- A dark curtain or veil
- A shadow entering from one side
- A missing section of peripheral vision
- A rapidly enlarging area of blur
- Sudden central visual loss
- New floaters and flashes followed by a visual-field defect
A retinal detachment occurs when fluid passes through a retinal tear and lifts the retina away from the back wall of the eye.
The condition is generally painless but can cause permanent visual loss if treatment is delayed.
When Should New Floaters Be Examined?
Arrange a prompt, preferably same-day, dilated retinal examination if you develop:
- Sudden new floaters
- A marked increase in longstanding floaters
- Flashes of light
- Numerous black dots
- A dark cloud
- Blurred or reduced vision
- A curtain or shadow
- Symptoms after eye trauma
- New symptoms after cataract or other eye surgery
Do not wait for the symptoms to disappear before seeking care.
A retinal tear may remain present even if flashes settle or floaters temporarily become less noticeable.
Are Longstanding Stable Floaters Dangerous?
Longstanding floaters that have remained unchanged for months or years are generally less concerning than sudden new symptoms.
However, arrange a routine examination if:
- The floaters have never been assessed.
- They interfere substantially with reading or driving.
- One eye is significantly more affected.
- Vision is persistently hazy.
- You have high myopia.
- You have undergone retinal or cataract surgery.
- You have diabetes or another retinal condition.
A new change from your usual baseline should always be treated as a fresh symptom.
What Else Can Cause Floaters?
Age-Related Vitreous Degeneration
The most common cause is gradual degeneration and liquefaction of the vitreous with age.
These floaters commonly develop slowly and become more noticeable over time.
High Myopia
A highly myopic eye is usually longer than average.
The stretched eye tends to undergo vitreous liquefaction and PVD earlier. High myopia is also associated with:
- Lattice degeneration
- Peripheral retinal thinning
- Retinal tears
- Retinal detachment
- Myopic macular degeneration
Patients who previously had LASIK, SMILE, PRK or ICL surgery remain at increased retinal risk if their original myopia was high. Vision-correction surgery changes the focusing power of the eye but does not shorten its axial length.
Vitreous Haemorrhage
Blood inside the vitreous may cause:
- Numerous dark floaters
- Red or brown clouds
- Cobweb-like shadows
- Smoky vision
- Marked visual reduction
Possible causes include:
- A retinal tear
- Proliferative diabetic retinopathy
- Retinal vein occlusion
- Eye trauma
- Abnormal retinal blood vessels
Vitreous haemorrhage requires prompt examination because the blood may conceal a retinal tear or detachment.
Eye Inflammation
Inflammatory cells within the vitreous may be perceived as floaters.
Possible associated symptoms include:
- Eye pain
- Redness
- Light sensitivity
- Blurred vision
Inflammation inside the eye, or uveitis, requires treatment directed at the underlying cause.
Retinal Tears and Detachment
A retinal tear may release blood or pigment into the vitreous, creating sudden floaters.
A retinal detachment may subsequently cause a curtain or missing visual field.
Diabetes
Advanced diabetic retinopathy can produce fragile abnormal blood vessels that bleed into the vitreous.
A person with diabetes who develops sudden dark floaters or hazy vision should not wait for their next routine diabetic screening appointment.
Retinal Vein Occlusion
Poor retinal circulation may stimulate abnormal blood vessels that later bleed into the vitreous.
Floaters may therefore arise weeks or months after the original vein occlusion.
Eye Trauma
Blunt or penetrating trauma can cause:
- Vitreous haemorrhage
- Retinal tears
- Retinal dialysis
- Retinal detachment
- Inflammation
- Lens or corneal damage
An injured eye should be examined even if central vision initially appears good.
Previous Eye Surgery
Floaters may become noticeable after cataract surgery because:
- The clearer artificial lens makes existing vitreous opacities more visible.
- A PVD may develop around the time of surgery.
- Pre-existing high myopia increases retinal risk.
- Rarely, a retinal tear, inflammation or bleeding has developed.
New flashes, floaters or a curtain after eye surgery require prompt retinal assessment.
Can Children Have Floaters?
Children may occasionally describe spots or shapes in their vision.
Possible causes include:
- Benign vitreous opacities
- Migraine-related visual phenomena
- Inflammation
- Trauma
- Retinal disease
- High myopia
Persistent, one-sided or sudden symptoms in a child should be examined, particularly when accompanied by reduced vision, flashes, pain or redness.
Are Floaters the Same as Visual Migraine?
No.
Floaters are usually small shapes that move with the eye and remain within the same eye.
Migraine-related visual symptoms are more likely to involve:
- Shimmering zigzag lines
- Expanding geometric patterns
- Flickering lights
- A temporary blurred or missing area
- Symptoms affecting the same side of vision in both eyes
- Gradual development over several minutes
- Resolution within approximately an hour
New visual symptoms should still be assessed when the diagnosis is uncertain, especially if they are confined to one eye or associated with persistent visual loss.
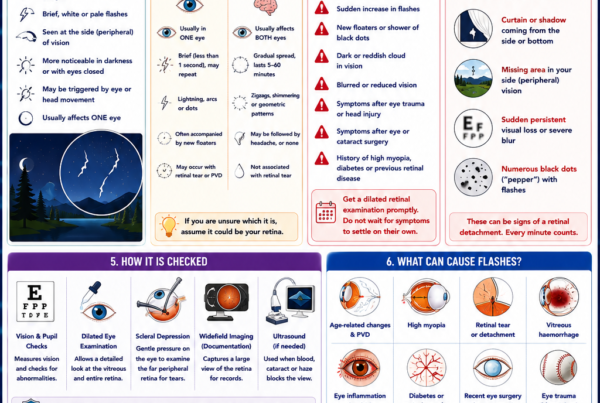
How Are Floaters Examined?
Medical and Symptom History
Your ophthalmologist may ask:
- When the floaters began
- Whether they appeared suddenly or gradually
- Whether flashes are present
- Whether there is a curtain or shadow
- Whether vision has changed
- Whether there was recent trauma or surgery
- Whether you have high myopia, diabetes or previous retinal disease
The timing and pattern help determine urgency but do not replace retinal examination.
Visual-Acuity Testing
Vision is checked in each eye.
Good central vision does not exclude a peripheral retinal tear.
Pupil Examination
The pupil responses are assessed for evidence of significant retinal or optic-nerve dysfunction.
Slit-Lamp Examination
The front of the eye and the anterior vitreous are examined.
The presence of:
- Blood
- Pigment cells
- Inflammatory cells
- Abnormal iris vessels
may provide clues to the underlying diagnosis.
Dilated Retinal Examination
Dilating drops enlarge the pupil so that the vitreous and retina can be examined.
The ophthalmologist looks for:
- Posterior vitreous detachment
- Retinal tears
- Retinal holes
- Lattice degeneration
- Retinal detachment
- Vitreous haemorrhage
- Diabetic or vascular retinal disease
A thorough peripheral retinal examination is the most important assessment for sudden floaters.
Scleral Depression
Scleral depression involves applying gentle pressure through the eyelid or onto the outer eye while examining the retina.
This brings the far peripheral retina into view and may reveal tears that are difficult to see with ordinary examination alone.
The examination can feel unusual or briefly uncomfortable, but it is valuable when an acute tear is suspected. The prospective PVD study found that some retinal tears were visible only with indirect ophthalmoscopy and scleral depression.
Widefield Retinal Photography
Widefield imaging may document a large area of retina and is helpful for:
- Recording retinal findings
- Locating a visible tear
- Comparing future examinations
- Patient education
However, a camera may not capture the entire extreme peripheral retina. Widefield imaging should not automatically replace a careful dilated examination with scleral depression when a tear is suspected.
Ocular Ultrasound
Ultrasound may be required when the retina cannot be seen clearly because of:
- Dense vitreous haemorrhage
- Cataract
- Corneal opacity
- Severe inflammation
It may detect a retinal detachment or other large abnormalities.
A small retinal tear may remain difficult to identify, so repeat examinations may be required as the view improves.
Optical Coherence Tomography
OCT produces detailed cross-sectional images of the macula.
It can identify:
- Vitreomacular traction
- Epiretinal membrane
- Macular hole
- Macular swelling
- Other central retinal conditions
A normal macular OCT does not exclude a tear in the far peripheral retina.
Do Floaters Go Away?
Floaters may become less noticeable with time.
This can happen because:
- The vitreous opacity moves away from the visual axis.
- The floater settles lower in the eye.
- The brain gradually learns to ignore the shadow.
- Blood or inflammatory material clears.
- Flashes subside as vitreous separation completes.
The floater may still remain physically present even when the patient notices it less often.
PVD-related flashes and floaters commonly become less intrusive over several weeks or months, although some floaters remain visible indefinitely.
Can Looking Up and Down Move a Floater?
Moving the eye may temporarily shift a floater away from the centre of vision.
However, the vitreous continues moving after the eye stops, so the opacity may drift back.
Eye movements do not remove or dissolve the floater.
Can Eye Drops Remove Floaters?
No ordinary eye drop has been proven to dissolve age-related vitreous floaters.
Drops applied to the eye’s surface do not reach the vitreous in a concentration that removes collagen condensations.
Drops may treat associated dry eye or inflammation but do not eliminate ordinary vitreous opacities.
Do Vitamins or Supplements Help?
No vitamin, herbal preparation or nutritional supplement has been proven to dissolve common vitreous floaters.
Products claiming to remove floaters should be approached cautiously, particularly when they encourage patients to delay retinal examination after sudden symptoms.
Can Screen Use Cause Floaters?
Computer and smartphone use do not generally create vitreous floaters.
Screens may make existing floaters easier to notice because of:
- Bright uniform backgrounds
- Prolonged visual concentration
- Increased awareness
- Eye strain or dry-eye-related blur
Screen breaks may improve comfort but do not remove vitreous opacities.
How Are Floaters Treated?
Observation
Observation is appropriate for most ordinary floaters once a retinal tear, haemorrhage, inflammation and other significant disease have been excluded.
Patients are advised to:
- Monitor for new symptoms
- Attend recommended follow-up
- Return urgently for more floaters, flashes or a curtain
- Allow time for neuroadaptation
No specific treatment is normally required for an uncomplicated PVD.
Laser Treatment for a Retinal Tear
Laser does not treat the floater itself.
If examination reveals a high-risk retinal tear, laser photocoagulation may be placed around the tear to create a protective adhesion and reduce the risk of retinal detachment.
The floaters may remain after successful laser because the vitreous opacity or blood has not been removed.
Vitrectomy for Severe Floaters
Vitrectomy is an operation in which small instruments are inserted through the white part of the eye to remove the vitreous gel and its opacities.
Because most of the vitreous is removed, vitrectomy can provide substantial relief from visually disabling floaters.
It may be considered when:
- Floaters have persisted for a substantial period.
- Retinal disease has been excluded or treated.
- Symptoms significantly impair reading, driving or work.
- The patient understands the surgical risks.
- Observation and adaptation have been unsuccessful.
Risks include:
- Cataract progression
- Retinal tear
- Retinal detachment
- Macular swelling
- Epiretinal membrane
- Infection
- Bleeding
- Raised or reduced eye pressure
- Loss of vision
Vitrectomy is therefore not recommended simply because a few floaters are annoying. The severity of symptoms must justify the risks of intraocular surgery.
YAG Laser Vitreolysis
YAG vitreolysis uses laser energy to disrupt or fragment selected vitreous opacities.
It is most commonly considered for a discrete, well-defined floater located safely away from the retina and natural lens, such as a prominent Weiss ring.
A small randomised clinical trial of 52 patients with symptomatic Weiss-ring floaters found greater self-reported improvement after YAG vitreolysis than after sham treatment at six months. However, the trial was small and was not designed to detect uncommon complications.
Important limitations include:
- Not every floater is suitable.
- Diffuse clouds or numerous fine opacities may respond poorly.
- Several sessions may be needed.
- Symptoms may improve without disappearing.
- Long-term comparative safety evidence remains limited.
- Potential complications include retinal injury, retinal tear, pressure elevation, inflammation and lens damage.
Current AAO summary guidance states that there is no consensus on floater treatment and that evidence remains insufficient to guide management universally.
Patients considering vitreolysis should first undergo a complete retinal examination and discuss the uncertainties, alternatives and potential risks with an appropriately trained ophthalmologist.
Is Vitrectomy Better Than Laser Vitreolysis?
The procedures are very different.
Vitrectomy
- Physically removes most vitreous opacities
- More predictable for diffuse or numerous floaters
- Involves intraocular surgery
- Carries cataract, retinal-detachment and infection risks
YAG Vitreolysis
- Attempts to fragment or displace selected opacities
- Avoids surgical entry into the eye
- Best suited to carefully selected floaters
- May provide partial rather than complete improvement
- Has less extensive long-term safety evidence
There is no single best option for every patient.
For most people, observation remains the safest approach.
Why Are Floaters Sometimes Distressing Despite Good Eye-Chart Vision?
Floaters may affect visual quality without substantially reducing high-contrast visual acuity.
Patients may experience difficulty with:
- Reading against a white page
- Using spreadsheets
- Viewing computer screens
- Driving in bright light
- Tracking moving objects
- Maintaining concentration
- Working in visually demanding occupations
The symptoms are genuine even when the patient can read the smallest eye-chart letters.
Treatment decisions should consider functional impairment while remaining proportionate to the risks of intervention.
What Follow-Up Is Needed After an Acute PVD?
The follow-up plan depends on:
- Retinal findings
- Presence of vitreous haemorrhage
- High myopia
- Lattice degeneration
- Previous retinal tear or detachment
- Previous eye surgery
- Severity of symptoms
- Whether a complete peripheral examination was possible
One or more follow-up examinations may be recommended during the first several weeks or months after symptomatic PVD because delayed tears can occur.
Do not wait for the scheduled appointment if you develop a sudden increase in floaters, new flashes, reduced vision or a curtain.
Warning Signs Requiring Urgent Assessment
Seek prompt eye care for:
- A sudden onset of new floaters
- A sudden increase in existing floaters
- A shower of black or pepper-like dots
- New flashes of light
- A dark or reddish cloud
- Sudden blurred or reduced vision
- A curtain, shadow or missing visual field
- Symptoms following eye injury
- New symptoms after cataract or retinal surgery
A curtain or shadow should be treated as an emergency.
Frequently Asked Questions
Are floaters normal?
A few stable floaters are common, particularly with increasing age or myopia.
Sudden new floaters are not automatically dangerous, but they require examination because a retinal tear cannot be excluded from symptoms alone.
Why do floaters move when I move my eyes?
The opacities are suspended within the vitreous gel. They move with the gel when the eye moves and may continue drifting briefly afterwards.
Why can I not look directly at a floater?
When you move your eye towards it, the vitreous opacity also shifts, causing the shadow to move away.
Will rubbing my eyes remove floaters?
No.
Rubbing does not remove vitreous opacities and may irritate or injure the eye.
Can dehydration cause floaters?
Ordinary dehydration has not been shown to create vitreous collagen floaters. Drinking more water does not dissolve them.
Are floaters caused by high blood pressure?
High blood pressure does not usually cause ordinary age-related floaters.
Severe hypertension or vascular disease may contribute to retinal bleeding, which can produce sudden dark floaters and requires assessment.
Can stress make floaters worse?
Stress does not normally create vitreous opacities, but anxiety and heightened visual attention may make existing floaters more noticeable.
Can cataract surgery remove floaters?
No.
Cataract surgery removes the cloudy natural lens, not the vitreous gel. Existing floaters may become more visible after surgery because the optical media are clearer.
Can floaters return after vitrectomy?
Most existing opacities are removed, but small residual vitreous, blood, inflammatory material or later retinal disease may produce new visual phenomena.
Is a ring-shaped floater dangerous?
A ring-shaped floater may represent a Weiss ring from PVD.
The ring itself is not necessarily dangerous, but the associated vitreous separation may have caused a retinal tear. A new ring should therefore be examined promptly.
Why do I still have floaters after retinal laser?
Laser seals the retinal tear but does not remove the vitreous opacity, pigment or blood that created the floater.
Can floaters affect both eyes?
Yes.
Age-related vitreous change commonly occurs in both eyes, although it may happen at different times and with different severity.
The Bottom Line
Eye floaters are shadows cast on the retina by opacities within the vitreous gel.
Most longstanding floaters are benign and gradually become less noticeable.
The important warning is a sudden change.
Seek prompt dilated retinal examination for:
- New floaters
- A marked increase in floaters
- Flashes of light
- A shower of black dots
- Blurred vision
- A dark cloud
- A curtain or shadow
Most uncomplicated posterior vitreous detachments settle without treatment, but approximately one in ten patients presenting with symptomatic PVD may already have an associated retinal tear or detachment.
Treatment is directed at the cause:
- Observation for uncomplicated floaters
- Laser or cryotherapy for a retinal tear
- Surgery for retinal detachment
- Treatment of bleeding or inflammation
- Vitrectomy in carefully selected patients with severely disabling floaters
- YAG vitreolysis only after careful selection and discussion of the limited evidence
Longstanding stable floaters are usually harmless. Sudden new floaters are a warning symptom until the retina has been properly examined.
References
- Kim SJ, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern. Ophthalmology. 2025.
- National Eye Institute. Vitreous Detachment. Updated December 2024.
- National Eye Institute. Floaters.
- National Eye Institute. Retinal Detachment. Updated November 2025.
- American Society of Retina Specialists. Posterior Vitreous Detachment.
- American Society of Retina Specialists. Retinal Tears.
- Nixon TRW, et al. Posterior Vitreous Detachment and Retinal Tear: A Prospective Study of Community Referrals. Eye. 2024.
- American Society of Retina Specialists. Vitrectomy for Floaters.
- Shah CP, Heier JS. YAG Laser Vitreolysis Versus Sham YAG Vitreolysis for Symptomatic Vitreous Floaters: A Randomised Clinical Trial. JAMA Ophthalmology. 2017.