Author: Dr Val Phua
Estimated reading time: 15 minutes
High myopia can usually be corrected with spectacles, contact lenses or refractive surgery.
For appropriately selected adults, Implantable Collamer Lens surgery—commonly known as ICL surgery—can correct even very high degrees of short-sightedness without removing central corneal tissue.
However, it is important to understand what “correction” means.
Glasses, contact lenses, ICL surgery and laser vision correction can improve the way light is focused inside the eye. They can reduce blurred distance vision and dependence on spectacles.
They do not shorten an elongated eyeball or reverse the structural changes associated with high myopia.
A person may therefore achieve excellent unaided vision after surgery while still having a higher lifetime risk of:
- Retinal tears
- Retinal detachment
- Myopic macular degeneration
- Myopic traction maculopathy
- Glaucoma
- Cataract
High myopia can be optically corrected, but it cannot currently be completely cured by refractive surgery. [1,2]
What Is High Myopia?
Myopia, or short-sightedness, occurs when light entering the eye focuses in front of the retina rather than directly on it.
This usually happens because:
- The eye has grown longer than normal
- The cornea is too steep
- The natural lens contributes too much focusing power
- A combination of these factors is present
The International Myopia Institute defines:
- Myopia as a spherical equivalent refractive error of −0.50 dioptres or more
- High myopia as a spherical equivalent refractive error of −6.00 dioptres or more
Someone with a prescription of −6.00 D, −10.00 D or −15.00 D would therefore usually be described as highly myopic. [1]
Does High Myopia Always Mean Pathologic Myopia?
No.
High myopia describes the degree of refractive error.
Pathologic myopia refers to structural damage caused by excessive elongation of the eye. These changes may include:
- Posterior staphyloma
- Myopic macular atrophy
- Lacquer cracks
- Myopic choroidal neovascularisation
- Myopic traction maculopathy
- Myopic optic nerve changes
A person can have high myopia without currently having pathologic retinal changes. Conversely, structural complications do not correlate perfectly with the spectacle prescription alone.
This distinction matters because refractive surgery may correct the optical prescription but cannot reverse established macular or retinal damage. [2]
Can High Myopia Be Completely Corrected?
In many patients, the refractive error can be fully corrected.
A person with −10.00 D of myopia may potentially be corrected close to plano—or zero prescription—using:
- Spectacles
- Contact lenses
- ICL surgery
- SMILE
- LASIK
- PRK
- Cataract surgery or refractive lens exchange in selected older patients
However, the ability to correct the prescription does not guarantee:
- Perfect unaided vision
- An exact zero prescription
- Complete elimination of astigmatism
- Normal retinal or macular health
- Freedom from glare or halos
- No future need for spectacles
- No future progression of myopia
- No future cataract or presbyopia
The best achievable vision depends on both the accuracy of the optical correction and the underlying health of the cornea, natural lens, optic nerve, macula and retina.
What Is the Difference Between Correcting and Curing High Myopia?
Correcting High Myopia
Correction changes where light focuses.
Examples include:
- A spectacle lens bending light before it enters the eye
- A contact lens changing the focusing power at the corneal surface
- An ICL adding optical power inside the eye
- LASIK or SMILE reshaping the cornea
These treatments can make distant objects clearer.
Curing High Myopia
A true cure would need to reverse the abnormal elongation and structural stretching of the eye.
Current refractive surgery does not:
- Shorten the eyeball
- Restore stretched retinal tissue
- Reverse a posterior staphyloma
- Remove myopic macular degeneration
- Eliminate the future risk of retinal detachment
This is why regular retinal and glaucoma examinations remain important even when unaided vision is excellent after surgery. [2,3]
How Can High Myopia Be Corrected?
The main options include:
- Spectacles
- Contact lenses
- ICL surgery
- SMILE
- LASIK
- PRK
- Cataract surgery or refractive lens exchange in selected patients
The best option depends on much more than the spectacle prescription.
Important factors include:
- Corneal thickness and shape
- Dry-eye status
- Anterior chamber depth
- Endothelial cell count
- Natural-lens clarity
- Age and presbyopia
- Retinal and macular health
- Lifestyle and occupation
- Previous eye surgery
- The patient’s tolerance for different surgical risks
Spectacles for High Myopia
Spectacles are the simplest and safest method of correcting high myopia.
Advantages include:
- No surgical risk
- Easy adjustment of the prescription
- Protection from wind and minor debris
- The ability to use specialised lens coatings
- Easy incorporation of reading or progressive correction
However, thick high-minus spectacle lenses may cause:
- Image minification
- Peripheral distortion
- A “swimming” sensation
- Reduced peripheral visual quality
- A visibly thick lens edge
- Apparent reduction in eye size
- Difficulty with sports or certain occupations
Modern high-index and aspheric lenses can reduce thickness and improve appearance, but they cannot eliminate every optical limitation of a very high prescription.
Contact Lenses for High Myopia
Contact lenses sit directly on the eye surface and usually produce less image minification and peripheral distortion than high-minus spectacles.
Options include:
- Soft contact lenses
- Toric soft contact lenses
- Rigid gas-permeable lenses
- Scleral lenses
- Customised lenses for very high prescriptions
Contact lenses may provide a wider field of clear vision and better visual performance during sport.
However, they require proper hygiene and may cause:
- Dryness
- Contact lens intolerance
- Allergic or inflammatory reactions
- Giant papillary conjunctivitis
- Corneal abrasions
- Corneal infection
- Permanent visual loss from severe microbial keratitis
Sleeping, swimming or showering while wearing contact lenses increases the risk of infection.
Can ICL Surgery Correct High Myopia?
Yes.
ICL surgery is particularly useful for moderate, high and very high myopia.
During the procedure, a soft corrective lens is placed:
- Behind the iris
- In front of the natural crystalline lens
The ICL works together with the eye’s natural lens to focus light accurately on the retina.
Unlike LASIK, PRK and SMILE, ICL surgery does not require central corneal tissue to be removed.
This is one reason ICL is frequently considered when:
- The prescription is very high
- The cornea is relatively thin
- Laser surgery would require excessive tissue removal
- Corneal tomography is unsuitable for laser correction
- Preserving the central cornea is a priority
- Dry-eye concerns make laser treatment less attractive
Long-term studies of modern central-port ICLs have reported good efficacy, predictability and refractive stability in moderate-to-extreme myopia. [5–9]
How High a Prescription Can ICL Correct?
The available range depends on:
- The ICL model
- Local regulatory approval
- Available lens powers
- The amount of astigmatism
- The patient’s internal eye anatomy
- The surgeon’s clinical judgement
As an example, United States FDA labelling for EVO ICL describes:
- Full correction of myopia from −3.00 D to −15.00 D
- Reduction of myopia up to −20.00 D
Approved ranges and available lens powers may differ in Singapore and other countries. [4]
What Happens if the Prescription Is Higher Than the Available ICL Power?
For extremely high prescriptions, an ICL may sometimes provide a partial correction rather than complete correction.
For example, a patient with an exceptionally high prescription may be left with a smaller residual prescription that can be managed using:
- Thinner spectacles
- Contact lenses
- Corneal laser enhancement in selected eyes
- Another staged treatment strategy
The aim may be to reduce a very high prescription to a much more manageable level rather than guarantee complete spectacle independence.
Why Is ICL Often Preferred for Very High Myopia?
No Central Corneal Tissue Is Removed
Corneal laser procedures correct myopia by removing tissue and flattening the central cornea.
The higher the prescription, the more tissue generally needs to be removed.
ICL corrects high myopia by adding a lens inside the eye, so its optical power is not dependent on removing an equivalent amount of corneal tissue.
It Can Treat a Wider Myopic Range
ICL can correct prescriptions beyond the preferred treatment range of many corneal laser procedures.
It May Preserve Better Optical Quality
Large corneal corrections can induce:
- Spherical aberration
- Coma
- Changes in the effective optical zone
- Glare
- Halos
- Reduced contrast sensitivity
Systematic reviews comparing ICL with excimer-laser surgery or SMILE in moderate-to-high myopia have found comparable refractive efficacy, with some evidence of better corrected vision, contrast sensitivity or higher-order aberration profiles after ICL. [11,12]
These results should not be interpreted as proof that ICL is superior for every patient. Many comparative studies were observational or involved earlier generations of refractive technology.
The ICL Can Usually Be Removed or Exchanged
An ICL can usually be surgically removed or exchanged if medically necessary.
Possible reasons include:
- Incorrect lens power
- Inappropriate vault
- Toric lens rotation
- Raised eye pressure
- Cataract development
- Inflammation
- Patient intolerance
However, removal requires another intraocular operation.
It is more accurate to describe ICL as removable rather than completely reversible. The eye cannot be guaranteed to return precisely to its preoperative condition.
Can ICL Improve Vision Beyond What Glasses Provide?
Some highly myopic patients gain lines of best-corrected visual acuity after ICL implantation.
Possible contributing factors include:
- Reduced spectacle minification
- Better retinal image size
- A wider effective visual field
- Less peripheral distortion
- Improved optical quality
- More accurate correction of high astigmatism
A large clinical series found that gains in best-corrected visual acuity occurred more frequently as the preoperative degree of myopia increased. However, improvement beyond preoperative spectacle-corrected vision is not guaranteed. [10]
Vision may remain limited by:
- Amblyopia
- Myopic macular degeneration
- Macular scarring
- Optic nerve damage
- Irregular astigmatism
- Previous retinal detachment
- Myopic traction maculopathy
- Cataract
Who May Be Suitable for ICL?
A suitable candidate typically has:
- Stable myopia, with or without regular astigmatism
- A prescription within the available lens range
- An adequately deep anterior chamber
- Open drainage angles
- A healthy corneal endothelial cell count
- A clear natural lens
- Acceptable eye pressure
- No active infection or inflammation
- Adequate retinal and optic nerve health
- Realistic expectations
- Willingness to attend long-term follow-up
Suitability is determined by a comprehensive examination rather than the prescription alone.
Who May Not Be Suitable for ICL?
ICL may be unsuitable when there is:
- An unstable prescription
- A shallow anterior chamber
- Narrow drainage angles
- An inadequate endothelial cell count
- Significant cataract
- Moderate or advanced glaucoma
- Active uveitis
- Active eye infection
- Progressive keratoconus
- Pregnancy or breastfeeding
- Vision-limiting retinal disease
- Unrealistic expectations
- Inability to attend long-term reviews
Older age and low postoperative vault have been associated with a greater risk of cataract in long-term ICL cohorts. [9]
What Results Can Be Expected After ICL Surgery?
Modern ICL studies have generally reported:
- High levels of refractive predictability
- Good unaided visual acuity
- Stable correction over time
- High patient satisfaction
- Low rates of serious complications in appropriately selected patients
The United States FDA clinical trial of the EVO and EVO+ spherical and toric ICLs found high levels of unaided distance vision and refractive accuracy. Long-term studies have reported continued efficacy and stability at eight and ten years. [5–9]
Results depend on:
- Preoperative visual potential
- Accuracy of the lens-power calculation
- Astigmatism measurement
- Lens size and vault
- Toric lens alignment
- Retinal health
- Healing
- Prescription stability
No operation can guarantee an exact zero prescription.
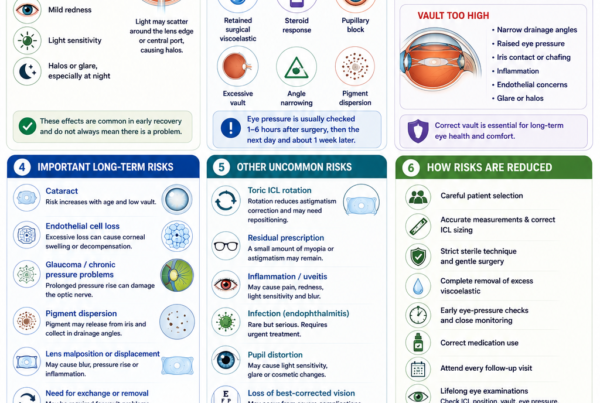
What Are the Main Risks of ICL Surgery?
ICL is an operation inside the eye. Although serious complications are uncommon in appropriately selected patients, they can occur.
Raised Eye Pressure
Eye pressure may rise because of:
- Retained surgical viscoelastic
- Inflammation
- Steroid response
- Excessive vault
- Narrowing of the drainage angles
- Pupillary block
- Pigment release
Early pressure checks are therefore important.
Incorrect Vault
Vault is the space between the ICL and the natural lens.
A very low vault may increase the risk of contact with the natural lens and cataract formation.
A very high vault may:
- Narrow the drainage angle
- Raise eye pressure
- Cause iris contact
- Produce inflammation
- Contribute to glare or halos
Cataract
The natural lens remains inside the eye and may develop cataract with age.
Cataract risk may be influenced by:
- Age
- Low vault
- Eye anatomy
- Surgical contact with the natural lens
- Length of follow-up
A long-term study found that older age and lower postoperative vault were associated with an increased likelihood of cataract development. The numerical rate from an individual study should not be treated as the expected rate for every modern EVO ICL patient. [9]
Endothelial Cell Loss
The endothelial cells line the inner surface of the cornea and help keep it clear.
Long-term monitoring is required because excessive cell loss could eventually contribute to corneal swelling or decompensation.
Toric ICL Rotation
A toric ICL must remain aligned with the intended astigmatism axis.
Significant rotation may result in:
- Residual astigmatism
- Ghosting
- Blurred vision
- Reduced visual quality
Repositioning or lens exchange may occasionally be required.
Inflammation or Infection
Mild postoperative inflammation is expected and is treated with prescribed medication.
Severe intraocular infection—known as endophthalmitis—is rare but potentially sight-threatening.
Urgent treatment is required for increasing pain, redness, light sensitivity or rapidly worsening vision.
Can LASIK Correct High Myopia?
LASIK can correct high myopia in selected patients.
However, as the intended correction increases:
- More corneal tissue must be removed
- The effective optical zone may become more challenging
- Regression may become more likely
- Residual myopia may be more common
- Corneal stability must be considered carefully
- Glare, halos and contrast-sensitivity changes may become more relevant
Older ten-year studies of LASIK for high and very high myopia reported useful long-term vision but also documented refractive regression and retreatment. Modern laser platforms, optical zones and planning techniques have changed substantially, so historical numerical results should not be applied directly to every present-day patient. [15,16]
LASIK may still be appropriate when:
- The cornea is sufficiently thick
- Corneal tomography is normal
- The residual stromal bed is adequate
- The percentage of tissue altered is acceptable
- Dry eye is controlled
- The expected optical result is favourable
Can SMILE Correct High Myopia?
Yes.
SMILE can correct high myopia in selected patients with suitable corneas.
During SMILE, a femtosecond laser creates a lenticule within the cornea. The surgeon removes this tissue through a small incision, changing the shape and focusing power of the cornea.
Long-term studies have reported stable correction after SMILE, including high-myopia cohorts. Mild regression has nevertheless been observed in some patients. [13,14]
Higher corrections require removal of a thicker corneal lenticule.
SMILE may be less suitable when:
- The cornea is thin
- Tomography is abnormal
- Keratoconus is suspected
- The prescription exceeds the platform’s treatment range
- The expected residual corneal tissue is inadequate
- Significant irregular astigmatism is present
Comparative studies generally find both SMILE and ICL effective for high myopia.
ICL may offer better contrast sensitivity or fewer induced higher-order aberrations in some studies, while SMILE avoids intraocular surgery and implant-related risks. [12]
Can PRK Correct High Myopia?
PRK is a surface-laser procedure that reshapes the cornea without creating a LASIK flap.
It may be considered when:
- The prescription is within an appropriate range
- The cornea is unsuitable for a flap
- The patient has a lifestyle in which a flap is undesirable
- Adequate corneal tissue remains
For high myopia, potential limitations include:
- Greater tissue removal
- A longer recovery
- More postoperative discomfort
- Corneal haze
- Refractive regression
- Delayed visual stabilisation
Mitomycin C and modern laser profiles have reduced the risk of haze, but PRK is not necessarily the preferred option for very high myopia.
Can Lens-Replacement Surgery Correct High Myopia?
Yes.
During refractive lens exchange, the natural lens is removed and replaced with an artificial intraocular lens.
This can correct high myopia even when ICL or corneal laser treatment is unsuitable.
However, removing a clear natural lens has important consequences.
Loss of Natural Focusing Ability
Younger patients lose the natural lens’s ability to change focus for near vision.
Retinal Detachment Risk
Highly myopic eyes already have an increased risk of retinal detachment.
Removing the natural lens may further influence that risk, particularly in younger patients with long axial lengths.
A systematic review found a higher incidence of retinal detachment following refractive lens exchange than following routine cataract surgery within the included studies and follow-up periods. [20]
Refractive lens exchange is therefore usually considered more cautiously in young highly myopic patients with clear natural lenses.
It may become more appropriate when:
- The patient is older
- Presbyopia is established
- Early cataract is present
- ICL anatomy is unsuitable
- The advantages outweigh the retinal and accommodative risks
Can High Myopia With Astigmatism Be Corrected?
Yes.
Possible options include:
- Toric spectacles
- Toric contact lenses
- Toric ICL
- SMILE
- LASIK
- PRK
- Toric intraocular lenses during cataract or lens-replacement surgery
A toric ICL can correct regular myopia and astigmatism within the available lens range.
Irregular astigmatism caused by keratoconus, corneal scarring or other corneal disease may not be fully corrected by a standard toric lens.
In these cases, the patient may still require:
- Rigid contact lenses
- Scleral lenses
- Spectacles
- Corneal treatment
- A combined surgical strategy
Can Extremely High Myopia Above −15.00 D Be Corrected?
Often, yes.
The available approaches depend on the eye anatomy and the lens powers available.
Options may include:
- A high-power ICL
- Partial correction with an ICL
- ICL combined with a later corneal laser enhancement
- Contact lenses
- Customised spectacles
- Lens-replacement surgery in selected older patients
Long-term studies have reported effective ICL correction in moderate-to-extreme myopia, although complication risk and limitations imposed by retinal disease become increasingly important as the degree of myopia and axial length increase. [6]
A very high prescription does not necessarily mean that the full prescription should always be surgically corrected.
The safest objective may sometimes be a substantial reduction rather than complete elimination of glasses.
Can Surgery Restore 6/6 Vision in High Myopia?
Potentially, but not always.
If the retina, macula, optic nerve and cornea are healthy, a highly myopic patient may achieve 6/6 or better vision with accurate correction.
Vision may remain below 6/6 when there is:
- Myopic macular degeneration
- Amblyopia
- Macular scarring
- Myopic traction maculopathy
- Previous retinal detachment
- Optic nerve damage
- Cataract
- Irregular astigmatism
- Corneal disease
A useful predictor is the best vision achieved with properly measured spectacles or contact lenses before surgery.
Refractive surgery generally cannot produce vision beyond the eye’s underlying visual potential, although some highly myopic patients may gain lines because an ICL avoids spectacle minification. [10]
Does Correcting High Myopia Prevent Retinal Detachment?
No.
Retinal-detachment risk in high myopia is mainly related to:
- Axial elongation
- Thinning and stretching of the peripheral retina
- Lattice degeneration
- Vitreous changes
- Retinal holes or tears
- Age-related posterior vitreous detachment
Changing the spectacle prescription does not reverse these anatomical factors.
Studies comparing ICL-treated eyes with other highly myopic eyes have not shown convincing evidence that modern central-port ICL itself adds substantial long-term retinal-detachment risk.
However, retinal detachment can still occur because the underlying highly myopic eye remains at risk. [17]
Does ICL Cure the Retinal Risks of High Myopia?
No.
An ICL corrects focus. It does not treat:
- Lattice degeneration
- Retinal holes
- Retinal tears
- Posterior staphyloma
- Myopic macular atrophy
- Myopic choroidal neovascularisation
- Myopic traction maculopathy
- Glaucoma
A highly myopic patient with excellent unaided postoperative vision still requires regular retinal and optic nerve examinations.
What Retinal and Macular Problems Are Associated With High Myopia?
Retinal Tears and Detachment
The elongated eye places greater mechanical stress on the peripheral retina.
Warning symptoms include:
- Sudden new floaters
- Flashes of light
- A curtain or shadow across the vision
- Sudden loss of peripheral vision
- Rapidly worsening vision
Myopic Macular Degeneration
Stretching and thinning of the tissues at the back of the eye can cause:
- Chorioretinal atrophy
- Lacquer cracks
- Macular haemorrhage
- Myopic choroidal neovascularisation
- Permanent central visual loss
Myopic Traction Maculopathy
Abnormal traction within a highly myopic eye can result in:
- Macular retinoschisis
- Foveal detachment
- Lamellar macular hole
- Full-thickness macular hole
- Macular-hole retinal detachment
The condition may remain stable or progress, so OCT monitoring may be required. [18,19]
Glaucoma
High myopia is associated with an increased risk of glaucoma and can make optic nerve and OCT interpretation more challenging.
Cataract
Highly myopic patients may develop cataract earlier. Cataract surgery in a long eye also requires careful intraocular lens calculation and retinal counselling. [3]
What Tests Are Needed Before Correcting High Myopia Surgically?
A comprehensive assessment may include:
Refraction and Visual Acuity
To determine:
- The exact myopic prescription
- Astigmatism
- Best-corrected vision
- Prescription stability
Corneal Topography and Tomography
To assess:
- Corneal shape
- Corneal thickness
- Keratoconus risk
- Suitability for laser surgery
- Previous corneal changes
Corneal Biomechanical Assessment
Selected patients may undergo additional testing to evaluate corneal deformation and structural risk.
Tear-Film and Eyelid Assessment
To identify:
- Dry eye
- Blepharitis
- Meibomian gland dysfunction
- Allergy
- Contact lens-related inflammation
Anterior Chamber Measurements
Particularly important for ICL surgery:
- Anterior chamber depth
- Drainage-angle anatomy
- Internal eye width
- White-to-white diameter
- Sulcus-to-sulcus measurements
- Natural-lens position
Endothelial Cell Count
This confirms that the cornea has an adequate endothelial cell reserve before intraocular surgery.
Eye Pressure and Optic Nerve Assessment
To identify glaucoma or ocular hypertension.
Dilated Retinal Examination
To look for:
- Lattice degeneration
- Retinal holes
- Retinal tears
- Retinal detachment
- Myopic macular degeneration
- Other peripheral retinal abnormalities
Macular OCT
OCT may be used to identify:
- Myopic traction maculopathy
- Retinoschisis
- Macular holes
- Epiretinal membrane
- Choroidal neovascularisation
- Macular atrophy
Should Retinal Problems Be Treated Before ICL Surgery?
Some retinal tears or high-risk lesions may require treatment before elective refractive surgery.
Other findings may only require observation.
The decision depends on:
- Symptoms
- The type of lesion
- Its location
- The presence of vitreoretinal traction
- Previous retinal detachment
- The condition of the opposite eye
- The retinal specialist’s assessment
Not every area of lattice degeneration requires preventive laser treatment.
A dilated retinal examination helps establish the retinal condition before surgery and provides a baseline for future monitoring.
Can High Myopia Continue to Progress After Surgery?
Yes.
ICL, LASIK, SMILE and PRK correct the prescription measured at the time of surgery. They do not necessarily stop further axial elongation or age-related refractive change.
Progression is more likely when:
- The prescription was not stable before surgery
- The patient is a young adult
- Axial length is still increasing
- There is a strong family history
- Other ocular or systemic factors are present
Surgery is normally delayed until the prescription is reasonably stable.
A future residual prescription may be managed with:
- Spectacles
- Contact lenses
- ICL exchange
- Toric ICL repositioning
- Laser enhancement
- Observation
Can Children With High Myopia Have ICL Surgery?
ICL surgery is not a routine treatment for childhood myopia.
Children and teenagers with high myopia usually require:
- Accurate spectacles
- Contact lenses in selected cases
- Amblyopia treatment when needed
- Assessment for inherited or systemic conditions
- Myopia-control treatment
- Regular retinal and ocular-health examinations
High myopia appearing at a very young age may be associated with:
- Retinal disorders
- Lens abnormalities
- Corneal disease
- Connective-tissue conditions
- Developmental syndromes
- Prematurity
- Genetic conditions
The International Myopia Institute recommends a detailed ocular and systemic assessment for young children with high myopia. [21]
Refractive surgery in children is generally reserved for exceptional situations in which conventional optical treatment has failed and the potential benefit justifies the risk.
Which Procedure Is Usually Best for High Myopia?
There is no universal prescription at which one procedure automatically becomes best.
A broad clinical approach may be:
Moderate High Myopia With a Thick, Normal Cornea
Possible options include:
- SMILE
- LASIK
- PRK
- ICL
The choice depends on corneal measurements, dry-eye status, lifestyle and risk preference.
High Myopia With a Thin or Laser-Unsuitable Cornea
ICL may be preferred if:
- The anterior chamber is sufficiently deep
- The drainage angles are open
- The endothelial cell count is adequate
- The natural lens is clear
Very High Myopia
ICL is often the preferred surgical option because it does not require extreme corneal tissue removal.
Older Patient With Cataract
Cataract surgery may be more appropriate because it treats both the refractive error and the cloudy natural lens.
Older Patient Without Cataract
The choice between ICL, corneal surgery and refractive lens exchange requires careful consideration of:
- Presbyopia
- Cataract risk
- Retinal-detachment risk
- Natural-lens clarity
- Anterior chamber dimensions
- Expected duration before cataract surgery
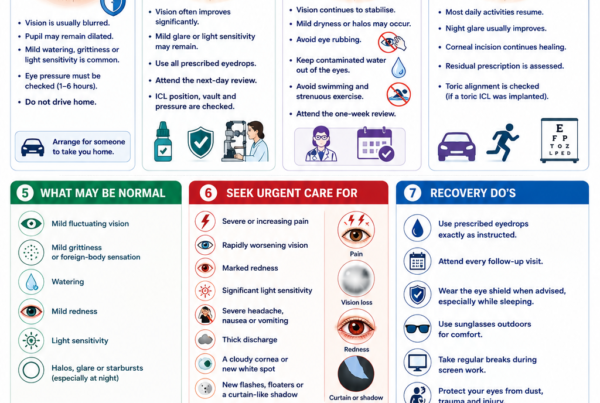
When Should a Highly Myopic Person Seek Urgent Eye Care?
Seek urgent assessment for:
- Sudden new floaters
- Repeated flashes of light
- A curtain or shadow across the vision
- Sudden peripheral visual-field loss
- Sudden central distortion
- A new dark or blank central spot
- Sudden loss of vision
- Eye pain with nausea or headache
- Significant trauma
- Rapidly worsening vision after surgery
New flashes, floaters or a curtain-like shadow may indicate a retinal tear or retinal detachment.
Sudden central distortion or a dark central spot may indicate myopic choroidal neovascularisation or another macular complication.
Frequently Asked Questions About Correcting High Myopia
Can −6.00 D Myopia Be Corrected?
Yes.
Possible options include spectacles, contact lenses, LASIK, SMILE, PRK and ICL, depending on the cornea and internal eye anatomy.
Can −10.00 D Myopia Be Corrected?
Yes.
ICL is commonly considered at this level because it can correct the prescription without requiring substantial corneal tissue removal.
SMILE or LASIK may still be appropriate in selected patients with sufficiently thick and regularly shaped corneas.
Can −15.00 D Myopia Be Corrected?
Often, yes.
ICL is frequently the main surgical consideration. The exact correction depends on available lens powers, astigmatism and eye anatomy.
Can −20.00 D Myopia Be Corrected?
The prescription may be fully or partially corrected depending on the available lens, local approval and the eye’s anatomy.
United States FDA labelling for EVO ICL describes full correction to −15.00 D and reduction of myopia up to −20.00 D. Other markets may have different ranges. [4]
Is ICL Better Than LASIK for High Myopia?
ICL is often more suitable when the prescription is high because it avoids removal of large amounts of corneal tissue.
LASIK may remain appropriate when the cornea is thick, tomography is normal and the expected tissue removal is acceptable.
Is ICL Better Than SMILE for High Myopia?
Both can be effective.
ICL may have advantages in contrast sensitivity, optical quality and preservation of corneal tissue.
SMILE avoids intraocular surgery, cataract risk related to an implant, vault problems and implant-specific endothelial monitoring. [12]
Can ICL Correct High Astigmatism?
A toric ICL can correct regular astigmatism within its available power range.
Very high or irregular astigmatism may require another strategy.
Will I Still Need Glasses After ICL?
Possibly.
Spectacles may still be needed for:
- Reading
- Night driving
- Fine visual tasks
- Residual myopia
- Residual astigmatism
- Future prescription changes
Does ICL Stop Myopia From Getting Worse?
No.
It corrects the existing refractive error but does not necessarily stop further axial elongation.
Does ICL Prevent Retinal Detachment?
No.
The underlying retinal risk associated with high myopia remains.
Can ICL Be Removed?
Usually, yes.
Removal or exchange requires another intraocular operation and should not be considered risk-free.
Can ICL Correct Myopia After LASIK or SMILE?
Potentially.
ICL may be considered when a residual or recurrent prescription remains and further corneal tissue removal is undesirable.
The cause of the refractive change must first be identified.
What Happens if Cataract Develops After ICL?
The ICL is usually removed, the cloudy natural lens is removed and a cataract intraocular lens is implanted.
Will I Need Eye Checks Even if My Vision Is Perfect?
Yes.
Long-term examinations should continue to assess:
- The retina
- The macula
- The optic nerve
- Eye pressure
- The natural lens
- ICL vault and position
- Corneal endothelial cells
Key Takeaway
High myopia can usually be corrected.
Spectacles and contact lenses provide effective non-surgical correction. LASIK, SMILE and PRK may be suitable when the cornea is sufficiently thick, regularly shaped and structurally stable.
ICL surgery is often particularly useful for moderate, high and very high myopia because it can correct a wide range of prescriptions without removing central corneal tissue.
However, no refractive procedure cures the underlying elongated eye.
Even after excellent surgical correction, highly myopic patients remain at increased risk of:
- Retinal tears
- Retinal detachment
- Myopic macular degeneration
- Myopic traction maculopathy
- Glaucoma
- Cataract
The best treatment depends on the prescription, corneal anatomy, internal eye dimensions, natural-lens clarity, age, retinal health and individual visual needs.
A comprehensive assessment is essential before deciding whether ICL, laser vision correction or another option offers the safest balance of benefits and risks.
References
- Flitcroft DI, He M, Jonas JB, et al. IMI—Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investigative Ophthalmology & Visual Science. 2019. PubMed Central
- Ohno-Matsui K, Wu PC, Yamashiro K, et al. IMI Pathologic Myopia. Investigative Ophthalmology & Visual Science. 2021. PubMed Central
- Du Y, et al. Complications of High Myopia: An Update From Clinical Manifestations to Underlying Mechanisms. 2024. PubMed
- US Food and Drug Administration. EVO/EVO+ Visian Implantable Collamer Lens—Approval Information and Instructions for Use. FDA
- Packer M, et al. Evaluation of the EVO/EVO+ Sphere and Toric Visian Implantable Collamer Lens. 2022. PubMed
- Wan Q, et al. Long-Term Observation of V4c Implantable Collamer Lenses in Moderate to Extreme High Myopia. 2024. PubMed
- Kamiya K, et al. Eight-Year Outcomes of Posterior Chamber Phakic ICL Implantation With Central-Port Technology. 2021. PubMed Central
- Alfonso-Bartolozzi B, et al. Ten-Year Follow-up of Posterior Chamber Phakic Intraocular Lenses With Central-Port Design. 2024. PubMed
- Kim YH, et al. Long-Term Outcome and Related Risk Factors in Implantable Collamer Lens Surgery. 2025. PubMed
- Zaldivar R, et al. Visual Acuity Improvement in Low, Moderate and High Myopia After ICL Surgery. 2023. PubMed Central
- Barsam A, Allan BDS. Excimer Laser Refractive Surgery Versus Phakic Intraocular Lenses for the Correction of Moderate-to-High Myopia. PubMed
- Li HY, Ye Z, Li ZH. Postoperative Efficacy, Safety, Predictability and Visual Quality of ICL Implantation Versus SMILE: A Meta-analysis. 2023. PubMed
- Damgaard IB, et al. Seven-Year Results of Small-Incision Lenticule Extraction for High Myopia. 2021. PubMed
- Blum M, et al. Ten-Year Results of Small-Incision Lenticule Extraction. 2019. PubMed
- Alió JL, et al. Ten-Year Follow-up of LASIK for High Myopia. 2008. PubMed
- Yan MK, Chang JS. Refractive Regression After LASIK. 2018. PubMed
- Xu W, et al. Long-Term Outcomes of Retinal Detachment in Phakic Eyes After ICL Implantation. 2020. PubMed
- Cheong KX, et al. An Evidence-Based Review of Myopic Traction Maculopathy. 2022. PubMed
- Lai TT, et al. Lamellar Macular Hole in Highly Myopic Eyes: Development, Evolution and Treatment. 2024. PubMed
- Passaro ML, et al. Retinal Detachment Incidence After Refractive Lens Exchange and Cataract Surgery: A Systematic Review. 2025. PubMed
- International Myopia Institute. IMI—Management and Investigation of High Myopia in Infants and Young Children. 2023. PubMed Central