Author: Dr Val Phua
Estimated reading time: 14 minutes
ICL surgery is a form of vision-correction surgery in which a specially designed lens is implanted inside the eye to correct short-sightedness and astigmatism.
Unlike LASIK, PRK or SMILE, ICL surgery does not reshape or remove tissue from the cornea. Instead, the implanted lens works together with the eye’s natural lens to focus light more accurately on the retina.
ICL surgery is frequently considered for people with moderate or high myopia, particularly when their prescription is beyond the preferred range for corneal laser surgery or when their corneas are thin or otherwise unsuitable for laser treatment. However, it may also be an option for selected patients with lower degrees of myopia.
Modern central-port ICLs have shown high levels of refractive accuracy, visual effectiveness and patient satisfaction in clinical studies. Nevertheless, ICL implantation is an operation inside the eye. Careful preoperative assessment, accurate lens sizing and lifelong eye follow-up remain important.
What Does ICL Stand For?
ICL stands for Implantable Collamer Lens.
It is a type of phakic intraocular lens:
- Phakic means that the eye’s natural lens remains in place.
- Intraocular means that the corrective lens is placed inside the eye.
- Collamer refers to the soft, flexible, collagen-containing polymer from which the lens is made.
The ICL is positioned behind the iris—the coloured part of the eye—and in front of the natural crystalline lens. It is therefore not normally visible to other people once it has been implanted.
Is an ICL the Same as an Intraocular Lens Used for Cataract Surgery?
No.
During cataract surgery, the cloudy natural lens is removed and replaced with an artificial intraocular lens.
During ICL surgery:
- The natural lens is not removed.
- The ICL is added in front of the natural lens.
- The natural lens can continue to change focus for near vision in younger patients.
For this reason, ICL surgery is sometimes described as an additive procedure, whereas laser vision correction reshapes the cornea and cataract surgery replaces the natural lens.
Is an ICL Like a Permanent Contact Lens?
The term “implantable contact lens” is sometimes used informally because an ICL corrects vision without being removed each day.
However, it is not placed on the surface of the eye like a contact lens. It is surgically implanted inside the eye and is designed to remain there long term.
How Does ICL Surgery Correct Vision?
In a short-sighted eye, light is focused in front of the retina rather than directly on it. This makes distant objects appear blurred.
The ICL contains the refractive power needed to redirect light so that it focuses more accurately on the retina.
A spherical ICL corrects myopia. A toric ICL can correct both myopia and astigmatism. Toric lenses must be positioned at the intended axis so that the astigmatism correction is properly aligned.
What Is an EVO ICL?
EVO is a modern generation of ICL that contains a small opening, known as a central port, in the centre of the lens.
This opening allows the eye’s natural fluid, called aqueous humour, to circulate through the lens. Earlier ICL designs without a central port commonly required a peripheral iridotomy before implantation. This involved using a laser to create small openings in the peripheral iris to reduce the risk of pupillary-block glaucoma.
With the EVO central-port design, a preoperative peripheral iridotomy is generally not required. Long-term studies of the central-port model have reported favourable visual and safety outcomes.
Who May Be Suitable for ICL Surgery?
ICL surgery may be considered for adults who:
- Have myopia, with or without astigmatism
- Have a reasonably stable spectacle prescription
- Wish to reduce their dependence on glasses or contact lenses
- Have corneas that may not be suitable for LASIK or SMILE
- Have moderate, high or very high myopia
- Have sufficient space within the front part of the eye
- Have an adequate corneal endothelial cell count
- Have healthy natural lenses without visually significant cataract
- Have realistic expectations about the likely benefits and limitations
Regulatory prescription ranges and age criteria differ between countries and lens models. Suitability should therefore be based on a complete eye examination rather than the spectacle prescription alone.
Is ICL Only for Very High Myopia?
No.
ICLs were traditionally associated mainly with high or extreme myopia because laser surgery becomes less suitable as the amount of corneal tissue that must be removed increases.
However, newer evidence indicates that central-port ICLs can also provide effective and predictable correction in appropriately selected patients with moderate and, in some settings, lower myopia. The decision should consider the prescription, corneal shape and thickness, eye anatomy, lifestyle, age and the relative risks of each procedure.
Can ICL Be Used When the Cornea Is Thin?
Potentially, yes.
Because ICL surgery does not remove central corneal tissue, it may be considered when the cornea is too thin for the proposed amount of laser correction.
However, a thin or abnormal cornea still requires proper investigation. Corneal tomography is important to identify keratoconus or other forms of corneal instability. ICL surgery corrects the refractive error but does not treat progressive keratoconus.
Can ICL Be Used for Astigmatism?
Yes. A toric ICL can correct both myopia and regular astigmatism.
The degree and type of astigmatism must be measured carefully. Irregular astigmatism from keratoconus, corneal scarring or other corneal disease may not be fully corrected by a toric ICL.
Who May Not Be Suitable for ICL Surgery?
ICL surgery may be unsuitable or require additional caution when there is:
- An unstable spectacle prescription
- Insufficient space in the anterior segment of the eye
- An inadequate endothelial cell count
- Existing cataract or significant natural-lens opacity
- Uncontrolled glaucoma or significant optic nerve damage
- Active inflammation or infection within the eye
- Certain iris or drainage-angle abnormalities
- Significant uncontrolled dry eye or eyelid disease
- Retinal disease that limits visual potential
- Pregnancy or breastfeeding, when the prescription may be unstable
- An unrealistic expectation of perfect vision in all circumstances
- An expectation that surgery will prevent future eye disease
The FDA patient information for EVO ICL identifies inadequate anterior chamber dimensions, low endothelial cell density, pregnancy or nursing, and moderate-to-severe glaucomatous optic nerve damage among its contraindications. Local criteria may differ and should be applied according to the lens used and the patient’s individual anatomy.
What Tests Are Needed Before ICL Surgery?
A detailed preoperative assessment is essential. The surgeon must determine both the correct optical power and the appropriate physical size of the ICL.
Refraction and Visual Acuity
The spectacle prescription is measured carefully to determine:
- The degree of myopia
- The amount and axis of astigmatism
- The best-corrected visual acuity
- Whether the prescription is stable
Cycloplegic refraction may be performed in selected patients to temporarily relax the eye’s focusing muscles.
Corneal Topography and Tomography
Scans are used to evaluate:
- Corneal shape
- Corneal thickness
- Astigmatism
- Signs of keratoconus or corneal instability
- Previous corneal surgery
Although ICL implantation does not substantially reshape the central cornea, pre-existing corneal disease may affect visual quality and long-term stability.
Anterior Chamber Measurements
The surgeon measures the space between the cornea and the natural lens. This helps determine whether there is sufficient room to safely position the ICL.
Measurements may include:
- Anterior chamber depth
- Angle anatomy
- White-to-white corneal diameter
- Sulcus-to-sulcus dimensions
- Other biometric measurements used for lens sizing
Accurate planning is important because the selected ICL size influences its final vault and position.
Endothelial Cell Count
The endothelium is a single layer of cells lining the inner surface of the cornea. These cells help keep the cornea clear.
An endothelial cell count is performed to ensure that there is an adequate reserve before intraocular surgery. The cells should continue to be monitored during long-term follow-up after ICL implantation.
Eye Pressure and Glaucoma Assessment
The eye pressure is measured, and the drainage angles and optic nerves are assessed.
Patients with glaucoma, narrow angles or unusual anterior-segment anatomy may require additional investigation or may not be suitable for ICL surgery.
Dilated Retinal Examination
The retina should be examined, particularly in patients with high myopia.
High myopia is associated with an increased lifetime risk of:
- Retinal holes
- Retinal tears
- Lattice degeneration
- Retinal detachment
- Myopic macular degeneration
- Other retinal changes
ICL surgery corrects the focusing error caused by myopia, but it does not shorten the eye or eliminate these underlying retinal risks.
Pupil Measurement
The size of the pupil in dim and normal lighting may be assessed.
Patients with relatively large pupils may be more aware of glare, halos or starbursts, particularly during the early postoperative period or when driving at night.
What Happens During ICL Surgery?
ICL surgery is usually performed as a day procedure.
Before the Operation
The eye is prepared with:
- Pupil-dilating drops
- Anaesthetic eyedrops
- Antiseptic cleaning
- Medication to reduce the risk of infection and inflammation
Sedation may be offered depending on the patient, surgical setting and anaesthetic plan.
During the Operation
The surgeon generally:
- Makes a small incision at the edge of the cornea.
- Inserts the folded ICL through the incision.
- Allows the lens to unfold inside the eye.
- Positions its supporting footplates behind the iris.
- Aligns the lens correctly, particularly if it is toric.
- Removes any surgical viscoelastic material as required.
- Checks the ICL position, pupil and eye pressure.
The incision is usually small and self-sealing, so stitches are not routinely necessary. The FDA patient booklet states that the procedure commonly takes approximately 20 to 30 minutes or less, although actual operating time varies.
Is ICL Surgery Painful?
The eye is numbed with anaesthetic medication, so patients should not experience sharp pain during the procedure.
It is normal to notice:
- Bright lights
- Movement
- Mild pressure
- Water around the eye
- Temporary blurring
Mild irritation, light sensitivity or a foreign-body sensation can occur after surgery. Severe or increasing pain is not expected and requires urgent review.
Are Both Eyes Treated on the Same Day?
Some surgeons operate on both eyes during the same session, while others perform surgery on separate days.
The decision depends on:
- The surgeon’s protocol
- The surgical facility
- The patient’s health and preference
- The refractive and anatomical findings
- Local professional and regulatory guidance
What Is Vault?
Vault refers to the space between the back surface of the ICL and the front surface of the natural lens.
An appropriate vault helps maintain safe separation from both the natural lens and the structures at the front of the eye.
What Happens if the Vault Is Too Low?
A very low vault may increase contact or proximity between the ICL and the natural lens. This can increase concern about anterior subcapsular cataract formation, particularly with older lens models and with increasing patient age.
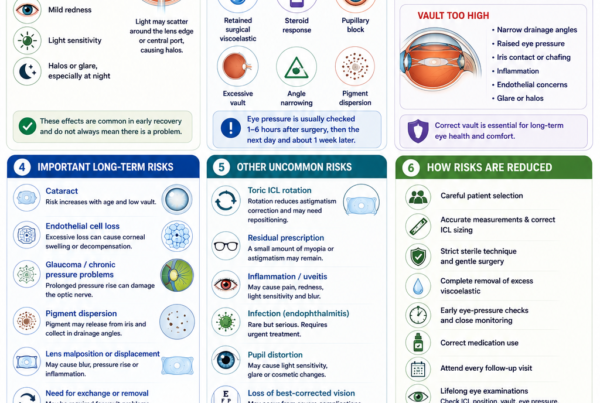
What Happens if the Vault Is Too High?
An excessively high vault may crowd the front part of the eye and contribute to:
- Narrowing of the drainage angle
- Raised eye pressure
- Iris contact
- Inflammation
- Glare or optical symptoms
Very high or very low vault may require closer observation, medication or lens exchange. Incorrect vault has been reported as an important reason for ICL exchange or removal.
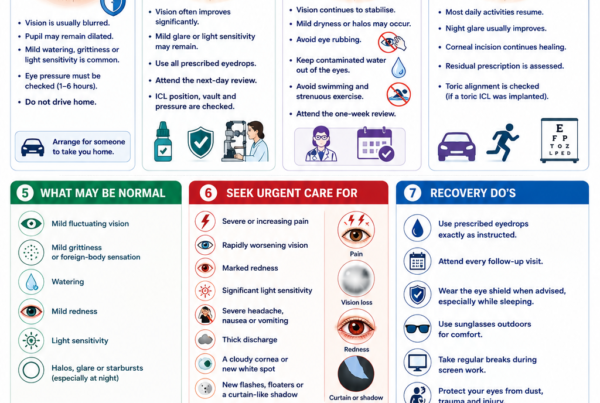
What Is Recovery Like After ICL Surgery?
Many patients notice a substantial improvement in distance vision within the first day. Vision may nevertheless fluctuate initially because of:
- Pupil dilation
- Mild inflammation
- Temporary corneal swelling
- Tear-film disturbance
- Residual medication
- Adjustment to the new optical correction
The eye pressure is usually checked soon after surgery because early pressure elevation needs to be identified and treated promptly. Follow-up is commonly arranged the next day and again during the early postoperative period.
During the First Few Days
Patients may experience:
- Mild grittiness
- Watering
- Light sensitivity
- Halos around lights
- Mild redness
- Temporary fluctuations in vision
Prescribed eyedrops commonly include an antibiotic and an anti-inflammatory medication. They should be used exactly as directed.
Activity After Surgery
Patients are generally advised to:
- Avoid rubbing or pressing the eyes
- Keep water, soap and shampoo out of the eyes initially
- Avoid eye makeup for the period advised
- Avoid swimming and hot tubs until permitted
- Avoid strenuous exercise and contact sports during early healing
- Wear the supplied eye shield when instructed
- Attend every scheduled follow-up visit
Driving should only resume when vision meets the legal requirement and the surgeon confirms that it is safe.
What Results Can Patients Expect?
The objective of ICL surgery is to reduce dependence on glasses or contact lenses. It does not guarantee perfect vision or lifelong freedom from glasses.
In the pivotal US study cited by the FDA, 75.9% of implanted eyes achieved 20/20 or better uncorrected distance vision at six months, and 98.9% achieved 20/32 or better. Outcomes depend on the preoperative prescription, eye health, lens calculation, healing and the visual potential of the eye.
A 2025 meta-analysis of central-port ICL studies concluded that these lenses demonstrated high efficacy, refractive predictability and safety for moderate-to-high myopia, with a low incidence of serious adverse events across the included prospective studies.
Long-term studies have also reported good refractive stability and visual outcomes at ten years. However, the risk of age-related cataract, endothelial cell change and other eye disease continues over time, so long-term follow-up remains necessary.
What Are the Advantages of ICL Surgery?
It Does Not Remove Central Corneal Tissue
Unlike LASIK, PRK and SMILE, ICL surgery does not use a laser to reshape the central cornea.
This may be beneficial when:
- The cornea is relatively thin
- The prescription is high
- The amount of required laser tissue removal would be excessive
- Corneal shape raises concern about laser suitability
It Can Correct a Wide Range of Myopia
ICL surgery can correct degrees of myopia that may be outside the preferred treatment range of some corneal laser procedures.
The Natural Lens Remains in Place
Younger patients retain the natural lens and its existing ability to focus at different distances.
However, the natural lens will still undergo age-related changes, including presbyopia and eventually cataract.
The Lens Can Be Removed or Exchanged
The ICL can usually be surgically removed or exchanged if medically necessary.
This may be required because of:
- Inappropriate vault
- A significant residual prescription
- Toric misalignment
- Cataract development
- Raised eye pressure
- Other complications
Nevertheless, ICL surgery should not be described as completely or effortlessly reversible. Removal requires another intraocular operation, and returning the eye to its exact preoperative state cannot be guaranteed. The FDA patient booklet similarly notes that the residual effect on the eye after removal is not fully known.
It May Provide Good Optical Quality
Because the central cornea is not flattened by tissue removal, ICL may provide favourable contrast sensitivity and optical quality in appropriately selected patients, particularly at higher prescriptions.
Comparative studies have found both ICL and modern laser procedures to be effective. Some analyses report advantages for phakic lenses in refractive accuracy, corrected vision or optical quality in moderate-to-high myopia, but the best choice depends on patient selection and the specific procedures being compared.
What Are the Limitations of ICL Surgery?
ICL surgery:
- Is an operation inside the eye
- Is usually more expensive than corneal laser surgery
- Requires accurate anatomical measurements and lens sizing
- Requires long-term monitoring
- Does not prevent presbyopia
- Does not prevent cataract
- Does not eliminate retinal risks associated with high myopia
- May not eliminate the need for glasses in every situation
- May require further surgery if the lens power, position or vault is unsuitable
Some patients may still require glasses for:
- Fine distance vision
- Night driving
- Residual astigmatism
- Reading after presbyopia develops
- Tasks requiring exceptionally sharp vision
What Are the Risks of ICL Surgery?
Most appropriately selected patients recover without serious complications. However, no intraocular operation is risk-free.
Raised Eye Pressure
Eye pressure may increase because of:
- Retained surgical viscoelastic
- Postoperative inflammation
- A steroid response
- Pupillary block
- Excessive ICL vault
- Narrowing of the drainage angle
- Pre-existing glaucoma susceptibility
Early pressure rises may occur soon after surgery, which is why postoperative pressure checks are important. Management may include eyedrops, oral medication, removal of retained viscoelastic, an iridotomy or lens exchange, depending on the cause.
Cataract Formation
The natural lens remains inside the eye and can develop cataract with age.
An anterior subcapsular cataract may occasionally develop after ICL surgery, particularly when:
- The vault is low
- The patient is older
- The anterior chamber is relatively shallow
- There is surgical trauma to the natural lens
- The ICL has been present for many years
Much of the longest-term cataract literature includes earlier ICL models without a central port, so complication rates cannot always be applied directly to current EVO lenses. Nevertheless, the possibility of cataract remains and should be discussed before surgery.
Endothelial Cell Loss
Intraocular surgery can affect the endothelial cells that keep the cornea clear.
Significant ongoing cell loss could eventually lead to corneal swelling or reduced clarity. This is uncommon in properly selected and monitored patients, but it is one reason why endothelial cell measurements and long-term reviews are recommended.
Incorrect Lens Size or Vault
Despite careful measurements, the postoperative ICL position cannot be predicted perfectly.
A lens that produces an unsuitable vault may need:
- Observation
- Additional imaging
- Pressure-lowering treatment
- Repositioning
- Exchange for a different size
- Removal
In one seven-year retrospective series involving 2,283 central-port ICL implantations, 2% required exchange or removal, with inappropriate vault being the most frequent indication. This rate is study-specific and should not be interpreted as a universal estimate.
Toric ICL Rotation
A toric ICL must remain aligned with the intended astigmatism axis.
If it rotates significantly, the patient may experience:
- Residual astigmatism
- Blurred vision
- Ghosting
- Reduced visual quality
The lens may need to be surgically rotated back into position or exchanged.
Residual Prescription or Refractive Change
A small amount of myopia or astigmatism may remain after surgery.
Options may include:
- Glasses
- Contact lenses
- Observation
- ICL rotation or exchange
- Corneal laser enhancement in selected patients
The eye can also undergo natural refractive changes with time.
Glare, Halos and Night-Vision Symptoms
Patients may notice:
- Halos
- Glare
- Starbursts
- Light scatter
- Difficulty with night driving
These symptoms often become less noticeable as the pupil returns to normal and the visual system adapts. However, they may persist in some patients, particularly when the pupil is large relative to the optical zone or when there is residual refractive error.
Inflammation
Mild postoperative inflammation is expected and is treated with anti-inflammatory eyedrops.
Excessive or persistent inflammation may require additional medication and investigation. Rarely, the iris, cornea, drainage structures or other parts of the eye may be affected.
Infection
Endophthalmitis is a rare but potentially sight-threatening infection inside the eye.
Warning symptoms include:
- Increasing pain
- Increasing redness
- Rapidly worsening vision
- Marked light sensitivity
- Increasing discharge or swelling
Urgent treatment is required. Infection, severe inflammation and other uncommon intraocular complications are included in the FDA patient safety information.
Retinal Tear or Retinal Detachment
Patients with high myopia already have an increased lifetime risk of retinal tears and retinal detachment because of the structure and length of the eye.
Long-term comparative studies have not demonstrated that central-port ICL implantation necessarily increases retinal-detachment prevalence beyond the underlying risk from high myopia. However, ICL surgery does not remove that risk. New flashes, floaters, a curtain-like shadow or sudden loss of vision require urgent retinal assessment.
Loss of Best-Corrected Vision
Although uncommon, it is possible to lose lines of best-corrected vision because of infection, inflammation, glaucoma, cataract, corneal damage, retinal disease or another complication.
The possibility of serious and permanent visual loss should be understood before any elective intraocular procedure.
ICL Surgery Versus LASIK or SMILE
There is no single procedure that is best for everyone.
ICL May Be Favoured When:
- Myopia is high
- Corneal tissue is insufficient for the proposed laser correction
- Corneal shape makes laser surgery less suitable
- Preserving central corneal structure is a priority
- Previous dry-eye symptoms make corneal nerve disruption a concern
- A large optical correction is required
LASIK or SMILE May Be Favoured When:
- The prescription is within a suitable range
- Corneal shape and thickness are appropriate
- The patient prefers to avoid intraocular surgery
- The patient is not anatomically suitable for ICL
- The risks of an implanted intraocular device outweigh the benefits
ICL avoids laser ablation of the central cornea but introduces intraocular risks such as cataract, pressure elevation, infection and sizing-related complications. Laser surgery avoids placing a permanent lens within the eye but changes the corneal structure and can contribute to dry eye, ectasia or flap-related issues, depending on the technique.
Systematic reviews comparing phakic lenses with laser surgery in moderate-to-high myopia have generally found both approaches effective, with some evidence favouring phakic lenses for refractive accuracy or preservation of corrected vision. Many of the comparative studies are older and involve previous generations of both procedures, so contemporary treatment should remain individualised.
Does ICL Surgery Correct Presbyopia?
A standard distance-correcting ICL does not stop or reverse presbyopia.
Presbyopia is the age-related reduction in the natural lens’s ability to focus on near objects. It usually becomes noticeable during the forties and continues to progress.
A patient who sees well at near without glasses by removing their myopic spectacles may lose this unaided near vision when both eyes are fully corrected for distance.
Possible strategies include:
- Reading glasses after surgery
- Leaving a small amount of myopia in one eye
- Monovision
- Other presbyopia-correcting approaches where appropriate
Monovision uses one eye mainly for distance and the other for nearer tasks. It can reduce spectacle dependence but may affect depth perception, contrast and night vision. A contact lens simulation is often useful before choosing monovision. Studies have reported favourable outcomes in selected presbyopic myopes treated with ICL monovision, but it is not suitable for everyone.
What Happens if Cataract Develops Later?
If a visually significant cataract develops:
- The ICL is usually removed.
- The cloudy natural lens is removed.
- A cataract intraocular lens is implanted.
Previous ICL surgery does not usually prevent cataract surgery, but the cataract surgeon needs to account for the ICL, the patient’s previous refractive history and the underlying high-myopia-related risks.
Does ICL Surgery Cure High Myopia?
ICL surgery corrects the optical blur caused by myopia. It does not reverse the anatomical elongation of a highly myopic eye.
Patients remain at increased risk of conditions associated with high myopia, including:
- Retinal tears and detachment
- Myopic macular degeneration
- Glaucoma
- Cataract
- Other peripheral retinal changes
Regular dilated eye examinations remain important even when unaided vision is excellent after surgery.
When Should You Seek Urgent Care After ICL Surgery?
Contact your surgeon urgently if you develop:
- Severe or increasing eye pain
- Rapidly worsening vision
- Increasing redness
- Marked light sensitivity
- Nausea or vomiting with eye pain
- A severe headache
- Increasing discharge
- A new white spot on the cornea
- A distorted or non-reactive pupil
- Sudden flashes or floaters
- A curtain or shadow across the vision
- Trauma to the operated eye
Do not wait for the next scheduled review when symptoms are rapidly worsening.
Frequently Asked Questions About ICL Surgery
How Long Does an ICL Last?
The lens is designed to remain inside the eye long term. It does not have a routine expiry date after implantation.
It may nevertheless need to be removed or exchanged if cataract, unsuitable vault, pressure problems, refractive change or another complication develops.
Can You Feel the ICL Inside the Eye?
The lens is positioned behind the iris and does not normally produce a sensation once the eye has healed.
Can Other People See the ICL?
Usually not. The lens is transparent and sits behind the coloured iris.
Can the ICL Fall Out?
It cannot fall out in the way that a surface contact lens can. It is positioned inside the eye.
Significant movement or rotation is uncommon but possible, particularly with toric lenses or after trauma.
Can I Rub My Eyes After ICL Surgery?
Eye rubbing should be avoided during the postoperative healing period.
Habitual vigorous rubbing should also be discouraged long term because of its effects on the cornea and eye surface.
Will I Still Need Glasses?
Many patients become substantially less dependent on glasses, but some may still require them for:
- Reading
- Night driving
- Fine visual tasks
- Residual refractive error
- Future prescription changes
Can I Have LASIK After ICL?
A corneal laser enhancement may be possible for selected patients with residual refractive error, provided the cornea is suitable.
This combined approach is sometimes referred to as bioptics. It requires a separate assessment and should not be assumed before the initial ICL operation.
Can an ICL Be Removed?
Yes, it can usually be surgically removed.
However, removal is another intraocular procedure and should not be considered risk-free. The eye may not return precisely to its preoperative state.
Will Pregnancy Affect an ICL?
Pregnancy does not normally cause the implanted lens itself to fail. However, hormonal and fluid changes during pregnancy can temporarily affect refraction and corneal measurements.
Elective refractive surgery is therefore generally postponed during pregnancy and breastfeeding until measurements are stable.
Do I Still Need Regular Eye Examinations?
Yes.
Long-term reviews may assess:
- Vision and refraction
- Eye pressure
- ICL position and vault
- The drainage angle
- The natural lens for cataract
- Corneal endothelial cells
- Retinal health
The FDA patient information recommends ongoing monitoring for cataract, intraocular pressure and endothelial health for as long as the lens remains in the eye.
Key Takeaway
ICL surgery corrects myopia and astigmatism by placing a soft corrective lens behind the iris and in front of the eye’s natural lens.
It can be an excellent option for appropriately selected patients, particularly those with moderate-to-high myopia or corneas that are less suitable for laser vision correction. The procedure preserves central corneal tissue, can correct a wide range of prescriptions and frequently provides rapid visual recovery.
However, it remains an operation inside the eye. Potential risks include raised eye pressure, inappropriate vault, cataract, endothelial cell loss, glare, inflammation, infection and the need for further surgery.
A detailed assessment of the cornea, anterior chamber, endothelial cells, natural lens, eye pressure and retina is essential. Regular long-term reviews remain important even when the initial visual result is excellent.
References
- US Food and Drug Administration. EVO/EVO+ Visian Implantable Collamer Lens: Recently Approved Device.
- US Food and Drug Administration. EVO ICL Patient Information Booklet.
- Larivoir NB, et al. Efficacy, Predictability, and Safety of Phakic Implantable Collamer Lenses With a Central Port: A Meta-analysis. 2025. PubMed.
- Packer M. The EVO ICL for Moderate Myopia: Results From the US FDA Clinical Trial. 2022. PubMed.
- Parkhurst G, et al. Three-Year Results From the United States FDA Prospective Multicentre Clinical Study of the EVO ICL. 2025. PubMed Central.
- Nakamura T, et al. Posterior Chamber Phakic Intraocular Lens Implantation for Myopia and Myopic Astigmatism: A 10-Year Follow-up Study. 2019. PubMed.
- Alfonso-Bartolozzi B, et al. Ten-Year Follow-up of Posterior Chamber Phakic Intraocular Lenses With Central-Port Design. 2024. PubMed.
- Kim YH, et al. Long-Term Outcome and Related Risk Factors in Implantable Collamer Lens Surgery. 2025. PubMed.
- Thompson V, et al. Implantable Collamer Lens Procedure Planning: A Review of Sizing and Vault. 2024. PubMed Central.
- Gong D, et al. Causes and Management Strategies for Elevated Intraocular Pressure After ICL Implantation. 2024. PubMed.
- Gimbel HV, et al. Incidence of Implantable Collamer Lens-Induced Cataract. 2018. PubMed.
- Packer KT, et al. US Military Implantable Collamer Lens Surgical Outcomes: An 11-Year Retrospective Review. 2022. PubMed.
- Alhamzah A, et al. Indications for Exchange or Explantation of Phakic ICL With a Central Port. 2021. PubMed.
- Goes S, et al. Posterior Chamber Toric Implantable Collamer Lenses Versus LASIK for Myopic Astigmatism: A Systematic Review. 2022. PubMed.
- Chen H, et al. Excimer Laser Versus Phakic Intraocular Lenses for Myopia and Astigmatism: A Meta-analysis of Randomised Controlled Trials. 2018. PubMed.
- Chen D, et al. Comparison of Visual Outcomes and Optical Quality After SMILE and ICL V4c Implantation. 2022. PubMed.
- Arrevola-Velasco L, et al. Ten-Year Prevalence of Rhegmatogenous Retinal Detachment Following ICL Implantation for High Myopia. 2023. PubMed.
- Ye Y, et al. Long-Term Follow-up of Monovision Surgery Using ICL V4c for Myopia With Presbyopia. 2022. PubMed.
- Du J, et al. Efficacy and Safety of ICL V4c Implantation in Low and High Myopia. 2023. PubMed.
- Yoon HY, et al. Causes and Outcomes of Implantable Collamer Lens Exchange. 2024. PubMed.