Worked for 1m 27s
Author: Dr Val Phua
Estimated reading time: 17 minutes
Femto-LASIK is a form of laser vision correction in which a femtosecond laser creates the corneal flap and an excimer laser reshapes the cornea to correct the prescription.
It is also commonly called:
- Femtosecond LASIK
- Femto-LASIK
- All-laser LASIK
- Bladeless LASIK
The term “bladeless” means that a mechanical microkeratome blade is not used to create the corneal flap. Femto-LASIK still involves a surgical procedure, a permanent flap interface and permanent removal of corneal tissue.
The two lasers perform different jobs:
- The femtosecond laser creates a thin, hinged flap within the cornea.
- The flap is lifted.
- The excimer laser removes microscopic amounts of corneal tissue to correct myopia, hyperopia or astigmatism.
- The flap is repositioned without stitches.
Current FDA documentation recognises that a LASIK flap may be created with either a mechanical microkeratome or a femtosecond laser. Modern Femto-LASIK allows the surgeon to programme flap dimensions such as thickness, diameter, hinge position and side-cut geometry with greater precision than traditional blade-based methods.
Femto-LASIK offers:
- Rapid visual recovery
- Relatively little early discomfort
- Broad treatment flexibility
- Customised excimer-laser options
- A relatively straightforward enhancement pathway
- More predictable flap construction than traditional microkeratome LASIK
However, it still carries risks including:
- Dry eye
- Glare and halos
- Flap displacement or folds
- Interface inflammation
- Epithelial ingrowth
- Residual prescription
- Infection
- Corneal ectasia
- Rare loss of best-corrected vision
Femto-LASIK is not automatically the best procedure simply because it uses two lasers. The safest choice depends on the patient’s corneal structure, prescription, tear-film health, lifestyle and long-term visual priorities.
What Does “Femto” Mean?
“Femto” refers to the extremely short duration of each laser pulse.
One femtosecond is:
One quadrillionth of a second, or 10⁻¹⁵ seconds.
Femtosecond lasers deliver highly focused ultrashort pulses of near-infrared energy within the cornea.
At the precise focal point, the pulses create microscopic areas of tissue separation through a process known as photodisruption. Thousands of closely spaced laser spots are placed at a programmed depth, forming a smooth tissue plane from which the flap can be lifted.
Because the energy is focused within the transparent cornea, the femtosecond laser can create the flap without passing a blade across the corneal surface.
Is Femto-LASIK the Same as LASIK?
Femto-LASIK is a modern form of LASIK.
All LASIK procedures require:
- A corneal flap
- An excimer-laser treatment beneath the flap
- Repositioning of the flap after treatment
The difference is how the flap is created.
Traditional Microkeratome LASIK
A mechanical device containing a blade moves across the cornea to create the flap.
Femto-LASIK
A femtosecond laser creates the flap using programmed laser pulses.
The excimer-laser part of the operation may be similar in both techniques.
Therefore, “Femto-LASIK” describes the method of flap creation, not the refractive treatment profile used beneath the flap.
Is Femto-LASIK the Same as Bladeless LASIK?
Yes. The terms are generally used interchangeably.
“Bladeless LASIK” means that the flap is made with a femtosecond laser rather than a bladed microkeratome.
However, bladeless does not mean:
- No surgical instruments
- No corneal incision
- No flap
- No removal of corneal tissue
- No risk
- A reversible procedure
The eyelids are still held open with a speculum, the flap is lifted using surgical instruments and the excimer laser permanently removes corneal tissue.
Is Femto-LASIK an All-Laser Procedure?
It is commonly described as all-laser LASIK because two lasers perform the principal refractive steps.
Femtosecond Laser
Creates the corneal flap.
Excimer Laser
Reshapes the underlying corneal tissue.
The term does not mean that every part of the operation is completed without instruments or physical contact.
How Does Femto-LASIK Correct Vision?
The cornea provides much of the eye’s focusing power.
Femto-LASIK changes the corneal curvature so that light focuses more accurately on the retina.
Myopia
In myopia, light focuses in front of the retina.
The excimer laser removes more tissue from the central cornea, flattening it and reducing its focusing power.
Hyperopia
In hyperopia, the optical system does not provide enough focusing power.
The laser applies treatment in a more peripheral ring pattern, making the central cornea relatively steeper.
Astigmatism
In astigmatism, the cornea or optical system has different focusing powers along different directions.
The excimer laser applies different amounts of correction along different meridians to produce a more balanced optical shape.
Current FDA labelling for one modern excimer platform includes myopia, hyperopia and mixed astigmatism within device-specific ranges. These ranges should not be interpreted as universal limits because suitability also depends on corneal anatomy and tissue calculations.
How Is Femto-LASIK Performed?
A typical procedure includes the following stages.
Preoperative Confirmation
Before treatment, the surgical team confirms:
- Patient identity
- Eye to be treated
- Prescription
- Treatment plan
- Corneal measurements
- Laser calibration
- Intended optical zone
Anaesthetic eyedrops are applied, and the skin around the eye is cleaned.
Eyelid Speculum
A small instrument keeps the eyelids open.
The patient does not need to worry about blinking during treatment.
Femtosecond-Laser Docking
The eye is aligned beneath the femtosecond laser.
A curved or flat patient interface gently contacts the eye, and suction stabilises it.
During docking, the patient may feel:
- Pressure
- Tightness
- Temporary dimming or loss of vision
- A sensation that the eye is being held still
The pressure sensation lasts for a relatively short period.
Flap Creation
The femtosecond laser places microscopic pulses within the cornea to create:
- The horizontal flap plane
- The flap edge
- A hinge that remains attached
The laser does not remove the flap. It creates a precise separation plane so that the surgeon can lift it.
Transfer to the Excimer Laser
Depending on the surgical platform, the patient may remain under an integrated system or be moved beneath a separate excimer laser.
Flap Lifting
The surgeon gently separates and lifts the flap, exposing the underlying corneal stroma.
Excimer-Laser Treatment
The patient looks towards a fixation light while the excimer laser reshapes the cornea.
Modern systems may incorporate:
- Eye tracking
- Pupil tracking
- Iris registration
- Cyclotorsion compensation
- Wavefront-guided treatment
- Topography-guided treatment
- Wavefront-optimised profiles
Available features depend on the laser platform and treatment plan.
Flap Repositioning
The flap is returned to its original position.
The surgeon checks:
- Flap alignment
- Flap edge
- Surface smoothness
- Absence of debris or folds
The flap usually remains in place without stitches.
How Long Does Femto-LASIK Take?
The complete theatre process commonly takes several minutes per eye, although the actual laser delivery is much shorter.
Time is needed for:
- Positioning
- Suction and docking
- Flap creation
- Flap lifting
- Excimer treatment
- Flap replacement
- Final examination
The exact duration varies with the equipment, prescription and surgical workflow.
Is Femto-LASIK Painful?
Anaesthetic eyedrops are used, so sharp pain should not normally occur during surgery.
Patients may feel:
- Pressure during femtosecond docking
- Tightness around the eye
- Temporary vision dimming
- Water around the eye
- Mild awareness of movement
- Bright or flashing lights
The pressure experienced during flap creation is usually brief.
After surgery, patients may experience:
- Burning
- Watering
- Grittiness
- Light sensitivity
- Hazy vision
- A desire to rub the eyes
These symptoms are usually most noticeable during the first several hours.
Severe or increasing pain is not considered normal and requires prompt review.
How Quickly Does Vision Recover?
Femto-LASIK generally offers one of the fastest recoveries among laser vision correction procedures.
The First Several Hours
Vision is often:
- Hazy
- Misty
- Fluctuating
- Sensitive to bright light
Patients are usually advised to rest with their eyes closed.
The Following Day
Many patients have functional unaided vision and can manage routine indoor activities.
The surgeon checks:
- Flap position
- Corneal clarity
- Inflammation
- Eye pressure
- Ocular-surface healing
- Visual acuity
The First Week
Vision commonly continues to sharpen.
Patients may still notice:
- Dryness
- Glare
- Halos
- Fluctuation
- A difference between the two eyes
The First One to Three Months
Fine visual quality, tear-film stability and night vision generally continue to improve.
The final refractive result should not be judged solely from the first few days.
When Can You Return to Work?
Many patients can return to office-based work within one to three days.
More time may be needed when work involves:
- Dust
- Smoke
- Chemicals
- Strong airflow
- Prolonged screen use
- Night driving
- Heavy physical activity
- Risk of facial or eye injury
Frequent breaks and lubricating eyedrops may be needed when returning to screen work.
When Can You Drive?
Driving should resume only when:
- Vision meets legal requirements
- The patient feels visually comfortable
- Glare and fluctuation are manageable
- The postoperative examination is satisfactory
- The surgeon has confirmed that driving is safe
Good daytime eye-chart vision does not necessarily mean that night driving is immediately comfortable.
What Are the Main Benefits of Femto-LASIK?
More Predictable Flap Thickness
A femtosecond laser creates the flap according to programmed dimensions.
Compared with mechanical microkeratomes, femtosecond systems generally provide:
- More predictable thickness
- Greater uniformity
- More consistent flap diameter
- More controllable hinge position
- More adjustable side-cut geometry
An American Academy of Ophthalmology technology assessment concluded that femtosecond lasers are effective for LASIK flap creation and provide reliable visual outcomes. Comparative evidence has generally shown better flap-thickness predictability, although final visual acuity and refractive results may remain similar to microkeratome LASIK.
Reduced Risk of Certain Blade-Related Complications
Femtosecond flap creation avoids some microkeratome-related problems such as:
- Irregular blade passage
- Incomplete mechanical cuts
- Free caps
- Buttonhole flaps caused by blade mechanics
- Certain extreme flap-thickness variations
Femto-LASIK introduces its own laser-specific complications, so the replacement of a blade does not eliminate flap risk.
Customisable Flap Design
The surgeon can usually programme:
- Flap thickness
- Flap diameter
- Hinge width
- Hinge position
- Side-cut angle
- Flap shape
This allows the flap plan to be adapted to:
- Corneal diameter
- Pupil size
- Treatment zone
- Corneal thickness
- Surgeon preference
- Expected enhancement strategy
Fast Visual Recovery
Because most of the surface epithelium remains intact, visual recovery is usually faster and early discomfort is generally less than after PRK or TransPRK.
Broad Refractive Treatment Options
The excimer-laser step may treat:
- Myopia
- Hyperopia
- Regular astigmatism
- Mixed astigmatism
- Monovision targets
The available range varies with the platform, regulatory approval and individual corneal measurements.
Customised Excimer-Laser Treatment
Femto-LASIK may be combined with:
- Wavefront-guided treatment
- Topography-guided treatment
- Wavefront-optimised treatment
- Aspheric treatment profiles
- Iris registration
- Cyclotorsion compensation
These options may be useful when addressing specific optical or corneal characteristics.
Relatively Straightforward Enhancement
When a residual prescription remains, the original flap may sometimes be lifted and further excimer treatment performed.
Other options include:
- PRK over the previous flap
- Spectacles
- Contact lenses
- Observation
Flap lifting is not automatically appropriate, particularly many years later, because the risk of epithelial ingrowth may increase.
Is Femto-LASIK Better Than Traditional Blade LASIK?
Femto-LASIK has largely replaced microkeratome LASIK in many modern refractive practices because it provides more controllable flap geometry.
However, comparative evidence does not show that every final visual outcome is dramatically better.
Systematic reviews have generally found:
- Similar final unaided visual acuity
- Similar corrected visual acuity
- Similar refractive accuracy
- Better flap-thickness predictability with femtosecond lasers
- Possible reductions in some induced optical aberrations
- Different complication profiles
A Cochrane review and earlier meta-analyses concluded that femtosecond and mechanical flap creation both produced effective LASIK outcomes, although the certainty of evidence for some comparisons was limited.
The practical advantages of Femto-LASIK are mainly:
- Greater flap planning control
- Reduced dependence on blade mechanics
- More predictable flap dimensions
- Potentially fewer selected flap complications
It should not be marketed as risk-free or as providing perfect vision merely because the flap is laser-created.
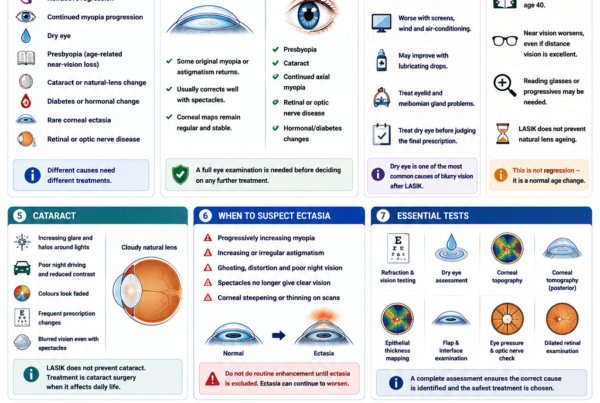
Does Femto-LASIK Cause Dry Eye?
Yes. Dry eye is one of the most common concerns after LASIK.
Creating the flap cuts across corneal nerves involved in:
- Corneal sensation
- Tear secretion
- Blinking
- Ocular-surface regulation
The excimer-laser treatment also affects stromal nerves.
During recovery, patients may experience:
- Burning
- Grittiness
- Watering
- Fluctuating vision
- Light sensitivity
- Contact lens intolerance
- Difficulty with prolonged screen use
A prospective study of patient-reported outcomes found that dry-eye symptoms generally improved over six months after myopic Femto-LASIK, although objective tear-film measurements did not always correlate with symptom improvement.
Is Dry Eye Always Temporary?
No.
For many patients, dryness improves substantially over weeks or months.
A smaller group may have prolonged symptoms, particularly when there was pre-existing:
- Meibomian gland dysfunction
- Aqueous tear deficiency
- Blepharitis
- Allergy
- Contact lens intolerance
- Reduced corneal sensation
- High screen exposure
- Autoimmune-related ocular-surface disease
Dry-eye risk should be assessed and treated before surgery.
Does a Thinner Flap Reduce Dry Eye?
A thinner flap may preserve more deeper corneal tissue and may reduce the number of stromal nerves transected.
Some studies have reported better corneal-sensation or tear-film recovery with thinner flaps, although flap thickness is not the only determinant of postoperative dryness. Flap diameter, hinge position, ablation depth and pre-existing ocular-surface health also matter.
Creating the thinnest technically possible flap is not automatically best. The flap must remain:
- Structurally intact
- Easy to lift
- Free from folds
- Appropriate for the treatment plan
Is Femto-LASIK Better Than SMILE for Dry Eye?
SMILE generally causes less early disruption of the anterior corneal nerve network because it avoids a broad hinged flap.
Comparative reviews generally report:
- Less early dry-eye disturbance after SMILE
- Faster corneal-sensation recovery after SMILE
- Similar final visual acuity
- Faster initial visual recovery after Femto-LASIK
The difference in dryness may become smaller over time, and SMILE can still cause dry eye.
What Is the LASIK Flap?
The flap is a thin layer of anterior corneal tissue that remains attached by a hinge.
It contains:
- Epithelium
- Bowman’s layer
- Anterior stromal tissue
- Corneal nerves
After excimer treatment, the flap is replaced over the underlying cornea.
The surface seals relatively quickly, but the deeper stromal interface remains a permanent anatomical plane.
Does the LASIK Flap Heal Completely?
The flap becomes stable enough for ordinary life, but it does not return to the structure of an untouched cornea.
Healing is strongest around the flap edge. The central interface remains relatively weak compared with unoperated corneal tissue.
This explains why:
- The flap may be lifted for an enhancement
- Severe trauma can occasionally move it years later
- Flap-specific complications remain possible long term
Patients should not assume that “healed” means the flap has disappeared.
Can the Flap Move Years Later?
Severe direct trauma can occasionally displace or wrinkle a LASIK flap years after surgery.
The risk is low during ordinary daily activities but more relevant for:
- Boxing
- Martial arts
- Rugby
- Water polo
- Wrestling
- Military training
- Police or tactical work
- Occupations involving repeated facial trauma
SMILE or PRK may be preferred when avoiding a permanent flap is a major priority.
What Are the Risks of Femto-LASIK?
Femto-LASIK is generally safe in appropriately selected patients, but no elective corneal surgery is risk-free.
Under-correction, Overcorrection or Residual Astigmatism
The final prescription may not be exactly zero.
Possible reasons include:
- Biological healing
- Measurement variation
- High original prescription
- Treatment decentration
- Cyclotorsion
- Tear-film instability
- Ongoing myopia progression
Management may include:
- Observation
- Spectacles
- Contact lenses
- Enhancement
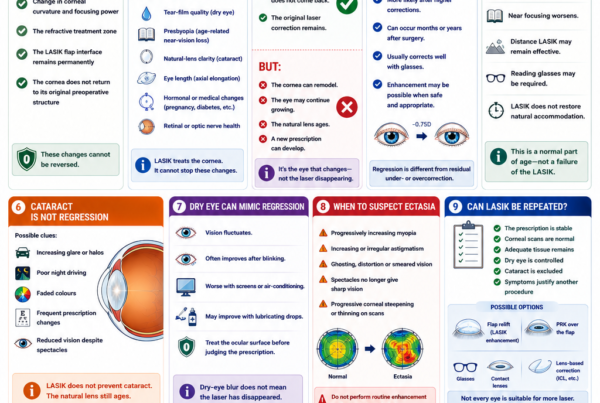
Refractive Regression
Some of the corrected myopia or hyperopia may return over time.
Risk may be greater with:
- High initial correction
- Younger age
- Continuing axial eye growth
- Hyperopic treatment
- Corneal remodelling
- Natural-lens changes
A long-term result that changes does not necessarily mean that the laser treatment has “worn off.” The eye itself may have continued to change.
Dry Eye
Dryness may affect comfort and visual quality.
It can range from mild temporary symptoms to persistent ocular-surface disease or, rarely, neuropathic corneal pain.
Glare, Halos and Starbursts
Patients may notice:
- Halos around headlights
- Starbursts
- Glare
- Ghost images
- Reduced contrast
- Difficulty driving at night
Risk is influenced by:
- Pupil size
- Optical-zone size
- Degree of correction
- Treatment centration
- Residual astigmatism
- Tear-film instability
- Higher-order aberrations
Flap Folds or Striae
Fine folds may form when the flap is not lying completely smoothly.
Minor folds may cause no visual problem.
Significant central folds can cause:
- Blurred vision
- Irregular astigmatism
- Ghosting
- Reduced corrected vision
Treatment may require lifting, smoothing or repositioning the flap.
Flap Displacement
The flap can shift if the eye is rubbed or traumatised during early healing.
Patients should avoid:
- Eye rubbing
- Forceful eyelid squeezing
- Direct pressure on the eye
- Contact sports until cleared
- Accidental contact from children or pets
Epithelial Ingrowth
Surface epithelial cells may grow beneath the flap edge.
Small areas may remain stable and require observation.
Progressive epithelial ingrowth can cause:
- Irregular astigmatism
- Flap melting
- Visual disturbance
- Inflammation
Treatment may require lifting the flap and removing the epithelial cells.
Epithelial ingrowth appears to occur less often after primary femtosecond flap creation than after some microkeratome procedures, but the risk increases after flap relifting or enhancement.
Diffuse Lamellar Keratitis
Diffuse lamellar keratitis, or DLK, is sterile inflammation within the flap interface.
It may appear as fine inflammatory cells beneath the flap.
Symptoms may include:
- Hazy vision
- Light sensitivity
- Discomfort
- Reduced visual quality
Mild DLK may respond to intensive steroid treatment.
More severe disease may require lifting and irrigating the flap.
Prompt diagnosis is important because untreated severe DLK can cause tissue damage and loss of vision.
Interface Infection
Infection beneath a LASIK flap is rare but potentially sight-threatening.
Warning symptoms include:
- Increasing pain
- Worsening redness
- Rapidly declining vision
- Discharge
- Marked light sensitivity
- A visible white corneal spot
Urgent assessment and intensive antimicrobial treatment are required.
Incomplete Flap or Suction Loss
The femtosecond laser requires stable docking and suction.
If suction is lost, the flap may be:
- Incomplete
- Irregular
- Unable to be safely lifted
Depending on the stage of treatment, the surgeon may:
- Re-dock the eye
- Adjust the laser plan
- Postpone the operation
- Convert to another procedure
Opaque Bubble Layer
The femtosecond laser creates microscopic gas bubbles while separating corneal tissue.
An opaque bubble layer may temporarily form if gas accumulates within the cornea.
It can:
- Obscure certain landmarks
- Interfere with eye tracking
- Make flap lifting more difficult
- Temporarily affect visualisation
It usually resolves without long-term harm.
Vertical Gas Breakthrough
Rarely, gas generated during flap creation may escape vertically towards the corneal surface.
This can interfere with flap formation and may be more likely when there is:
- Corneal scarring
- Previous surgery
- A break in Bowman’s layer
- Unusual corneal anatomy
Transient Light Sensitivity Syndrome
Some patients develop significant light sensitivity days or weeks after femtosecond flap creation despite relatively little visible inflammation.
This is known as transient light sensitivity syndrome.
It generally responds to topical steroids and usually resolves, but it remains a recognised femtosecond-laser-specific complication.
Rainbow Glare
Rainbow glare is a rare visual effect in which patients see coloured bands around bright lights.
It is believed to arise from diffraction caused by the regular pattern of femtosecond laser spots on the back surface of the flap.
Symptoms often improve with time, but persistent cases have been reported.
Interface Fluid Syndrome
Markedly raised eye pressure can cause fluid to collect beneath the flap.
This may mimic interface inflammation and may produce falsely low pressure readings when pressure is measured over the central fluid pocket.
Prompt recognition is important because treatment requires lowering the eye pressure rather than simply increasing steroids.
Corneal Ectasia
Corneal ectasia is progressive weakening and bulging of the cornea.
It may cause:
- Increasing myopia
- Irregular astigmatism
- Ghosting
- Reduced corrected vision
- Need for rigid or scleral lenses
- Need for corneal cross-linking
- Rarely, corneal transplantation
The flap and excimer ablation both affect the corneal structure.
Risk is reduced by careful assessment of:
- Corneal topography
- Corneal tomography
- Corneal thickness
- Epithelial thickness
- Residual stromal tissue
- Percentage of tissue altered
- Age
- Prescription
- Keratoconus susceptibility
Femto-LASIK should not be performed simply because a thin, predictable flap can be created. The underlying cornea must still be structurally suitable.
Can Femto-LASIK Cause Blindness?
Severe permanent visual loss is rare but possible.
Potential causes include:
- Severe infection
- Advanced corneal ectasia
- Severe interface inflammation
- Corneal scarring
- Irregular astigmatism
- Other uncommon complications
Most complications can be treated more effectively when recognised early.
Who May Be Suitable for Femto-LASIK?
A typical suitable candidate has:
- An adult, stable prescription
- Myopia, hyperopia or regular astigmatism within the treatment range
- Healthy corneal topography and tomography
- Adequate corneal thickness
- Safe residual stromal tissue after flap and ablation
- A stable ocular surface
- No active infection or inflammation
- No significant cataract
- Realistic expectations
- Willingness to attend follow-up
- A lifestyle compatible with a permanent flap
Under one current FDA-approved excimer-laser indication, patients must be at least 18 years old and have a refractive change no greater than approximately 0.50 D during the preceding year. Exact criteria vary by platform and jurisdiction.
Who May Not Be Suitable?
Femto-LASIK may be unsuitable when there is:
- Keratoconus
- Pellucid marginal degeneration
- Suspicious or progressive corneal tomography
- Insufficient corneal tissue
- Unstable refraction
- Severe dry eye
- Active eye infection or inflammation
- Significant corneal scarring
- Active autoimmune disease affecting healing
- Poorly controlled diabetes
- Pregnancy or breastfeeding
- Significant cataract
- Uncontrolled or advanced glaucoma
- Vision-limiting retinal or optic nerve disease
- Unrealistic expectations
A patient who is unsuitable for blade-based LASIK is not automatically made suitable merely by using a femtosecond laser.
Is Femto-LASIK Suitable for Thin Corneas?
Possibly, but the femtosecond laser does not make an unsafe cornea safe.
A predictable thin flap may preserve more residual stromal tissue than an unexpectedly thick mechanical flap.
However, the surgeon must still consider:
- Total corneal thickness
- Corneal shape
- Posterior corneal elevation
- Pachymetry distribution
- Flap thickness
- Laser-ablation depth
- Optical-zone diameter
- Residual stromal-bed thickness
- Percentage of tissue altered
- Epithelial mapping
- Biomechanical risk
PRK, TransPRK, SMILE or ICL may provide a safer option depending on the findings.
Is Femto-LASIK Suitable for High Myopia?
Sometimes.
Higher corrections require more excimer-laser tissue removal.
This may increase:
- Ectasia concern
- Regression
- Glare and halos
- Induced optical aberrations
- Enhancement limitations
A patient with high myopia and a thick, regular cornea may be suitable.
Another patient with a lower prescription may be unsuitable because of abnormal tomography or inadequate tissue.
ICL should be considered when corneal laser treatment would remove excessive tissue.
Is Femto-LASIK Suitable for Dry Eyes?
Mild or moderate dry eye may sometimes be treated before surgery.
The ocular surface should be stable before final:
- Refraction
- Corneal topography
- Corneal tomography
- Wavefront measurements
Severe or persistent dry-eye disease may rule out Femto-LASIK.
Treatment may include:
- Preservative-free lubricants
- Warm compresses
- Eyelid hygiene
- Meibomian gland treatment
- Allergy treatment
- Anti-inflammatory therapy
- Temporary discontinuation of contact lenses
Is Femto-LASIK Suitable for Contact Sports?
Possibly, but flap trauma must be considered.
Patients involved in repeated direct-impact activities may prefer:
- SMILE
- PRK
- TransPRK
because these procedures do not create a hinged LASIK flap.
The decision should account for the type, intensity and lifetime duration of the sport.
What Tests Are Needed Before Femto-LASIK?
Refraction and Visual Acuity
The examination measures:
- Myopia or hyperopia
- Astigmatism
- Best-corrected visual acuity
- Prescription stability
Cycloplegic Refraction
Dilating drops may be used to relax accommodation and confirm the true prescription.
Corneal Topography
Topography measures the curvature of the front corneal surface and helps detect:
- Corneal asymmetry
- Irregular astigmatism
- Keratoconus patterns
- Contact lens warpage
Corneal Tomography
Tomography evaluates:
- Anterior corneal elevation
- Posterior corneal elevation
- Thickness distribution
- Pachymetry progression
- The thinnest corneal point
- Ectasia susceptibility
Corneal Thickness and Tissue Calculations
The surgeon estimates:
- Intended flap thickness
- Ablation depth
- Optical-zone requirements
- Residual stromal-bed thickness
- Percentage of tissue altered
- Remaining structural reserve
Epithelial Thickness Mapping
Epithelial mapping may reveal:
- Early keratoconus compensation
- Contact lens-related distortion
- Localised stromal irregularity
- Previous surgical changes
Corneal Biomechanical Assessment
Biomechanical measurements may add information about corneal deformation.
No biomechanical test can guarantee that ectasia will not occur.
Dry-Eye and Eyelid Assessment
The surgeon evaluates:
- Tear-film stability
- Corneal staining
- Meibomian glands
- Blepharitis
- Allergy
- Tear production
- Eyelid closure
Pupil Measurement
Pupil size helps with counselling about:
- Night vision
- Halos
- Glare
- Optical-zone planning
Eye Pressure and Optic Nerve
Baseline pressure and optic nerve findings should be documented.
LASIK changes corneal thickness and biomechanics, which can make future pressure measurements read artificially lower.
Natural-Lens Examination
The surgeon checks for:
- Cataract
- Early lens changes
- Lens-related prescription shifts
- Other causes of glare
Dilated Retinal Examination
This is particularly important for moderate and high myopia.
Femto-LASIK corrects the cornea but does not remove the underlying retinal risks associated with an elongated myopic eye.
Why Must Contact Lenses Be Stopped Before Testing?
Contact lenses can temporarily change:
- Corneal curvature
- Astigmatism
- Tear-film stability
- Epithelial thickness
- Refraction
- Corneal maps
The required contact lens-free period depends on:
- Soft or rigid lenses
- Toric lenses
- Overnight wear
- Duration of contact lens use
- Evidence of corneal warpage
Final surgery should not be planned until repeated measurements are stable.
Femto-LASIK vs SMILE
Femto-LASIK
- Creates a hinged flap
- Uses femtosecond and excimer lasers
- Provides very rapid visual recovery
- Can treat myopia, hyperopia and selected astigmatism
- Offers wavefront- and topography-guided options
- Generally has a more straightforward enhancement pathway
- Causes more early corneal nerve disruption
SMILE
- Does not create a hinged flap
- Uses a femtosecond laser to create a lenticule
- Mainly treats myopia and myopic astigmatism
- May cause less early dry eye
- May suit contact-sport patients
- Has more complex enhancement options
Comparative evidence generally shows similarly good final visual and refractive outcomes, with faster early recovery after Femto-LASIK and less early dryness after SMILE.
Femto-LASIK vs PRK or TransPRK
Femto-LASIK
- Creates a flap
- Faster recovery
- Less postoperative pain
- Lower surface-haze risk
- More flap-related complications
- More early nerve disruption
PRK or TransPRK
- No flap
- Epithelium must regrow
- More pain
- Slower visual recovery
- Corneal haze risk
- Preserves more load-bearing stromal tissue
- May be preferred when trauma is a concern
Is Femto-LASIK Permanent?
Yes.
The excimer laser permanently removes corneal tissue.
The flap can be lifted, but the tissue removed beneath it cannot be restored.
Vision can nevertheless change later because of:
- Continuing myopia progression
- Corneal remodelling
- Presbyopia
- Cataract
- Hormonal changes
- Diabetes-related refractive shifts
- Other eye disease
Does Femto-LASIK Prevent Presbyopia?
No.
Presbyopia occurs because the natural crystalline lens loses flexibility with age.
Femto-LASIK reshapes the cornea but does not restore natural accommodation.
Patients corrected fully for distance will generally need reading glasses as presbyopia develops.
A monovision strategy may be considered:
- One eye is corrected for distance
- The other retains mild myopia for near or intermediate vision
A contact lens trial is advisable before permanent monovision treatment.
Does Femto-LASIK Prevent Cataract?
No.
The natural lens remains inside the eye and continues to age.
When cataract develops, cataract surgery remains possible, but previous laser vision correction must be considered when calculating the cataract intraocular-lens power.
Patients should retain their refractive surgery records where possible.
How Long Do Femto-LASIK Results Last?
The corneal tissue removal is permanent.
Long-term LASIK studies extending beyond ten years generally show good safety and continued visual benefit in appropriately selected patients, although refractive regression and enhancement become more common with higher corrections and longer follow-up. Much of the longest-term evidence includes older platforms and does not exclusively represent current Femto-LASIK technology.
The result may change because:
- The eye continues to elongate
- The cornea remodels
- Presbyopia develops
- Cataract alters the prescription
- Other eye disease develops
Frequently Asked Questions About Femto-LASIK
Is Femto-LASIK the Same as Bladeless LASIK?
Yes. The flap is created with a femtosecond laser rather than a mechanical blade.
Does Femto-LASIK Use Two Lasers?
Usually, yes.
The femtosecond laser creates the flap, and the excimer laser corrects the prescription.
Does the Femtosecond Laser Correct the Prescription?
Not during standard Femto-LASIK.
Its main role is to create the corneal flap.
The excimer laser performs the refractive reshaping.
Is Femto-LASIK Better Than Traditional LASIK?
It provides more predictable and customisable flap construction.
Final visual acuity and refractive accuracy may be similar when both procedures are uncomplicated.
Is Femto-LASIK Pain-Free?
Sharp pain should not occur during surgery because anaesthetic drops are used.
Pressure occurs during docking, and burning or watering may occur for several hours afterwards.
How Fast Is Recovery?
Many patients have functional vision by the following day.
Dryness, glare and visual fluctuation may continue for weeks.
Can Femto-LASIK Treat Astigmatism?
Yes, regular astigmatism can be treated within the platform’s suitable range.
Can Femto-LASIK Treat Hyperopia?
Yes, compatible excimer-laser platforms can treat selected hyperopia and hyperopic astigmatism.
Is Femto-LASIK Suitable for High Myopia?
Possibly, when enough healthy corneal tissue remains.
ICL may be safer if the laser treatment would remove excessive tissue.
Is Femto-LASIK Suitable for Thin Corneas?
Possibly, but a predictable thin flap does not make every thin cornea suitable.
PRK, SMILE or ICL may provide a better structural safety margin.
Does Femto-LASIK Cause Dry Eye?
Temporary dryness is common.
Persistent symptoms can occur, especially when dry-eye or eyelid-gland disease was present before surgery.
Can the Flap Move?
It can move during early healing if the eye is rubbed or injured.
Severe trauma can rarely disturb it years later.
Can I Rub My Eyes After Femto-LASIK?
Eye rubbing should be avoided during early recovery.
Habitual vigorous rubbing should also be discouraged long term.
Does the Flap Disappear?
No.
The flap remains as a permanent corneal interface.
Can Femto-LASIK Be Reversed?
No.
The laser-removed stromal tissue cannot be replaced.
Can Femto-LASIK Cause Ectasia?
Yes, although the risk is low after appropriate screening.
Abnormal corneal structure or excessive tissue removal increases concern.
Can Femto-LASIK Cause Halos?
Yes.
Halos, glare and starbursts may occur, particularly during early recovery or in dim lighting.
Can I Still Need Glasses?
Yes.
Glasses may still be needed for:
- Residual prescription
- Night driving
- Fine visual tasks
- Reading after presbyopia
- Future refractive change
Can Femto-LASIK Be Enhanced?
Possibly.
The flap may sometimes be relifted, or a surface-laser enhancement may be performed.
Suitability depends on corneal thickness, maps and prescription stability.
Is Femto-LASIK Suitable for Contact Sports?
It can be, but the permanent flap must be considered.
SMILE or surface ablation may be preferred when repeated direct eye trauma is likely.
Can Femto-LASIK Cause Blindness?
Severe permanent visual loss is rare but possible following serious infection, ectasia, scarring or another major complication.
Do I Still Need Eye Examinations?
Yes.
Regular examinations remain important for:
- Dry eye
- Eye pressure
- Glaucoma
- Cataract
- Corneal health
- Retinal health
- Myopia-related complications
Key Takeaway
Femto-LASIK is a modern form of LASIK in which:
- A femtosecond laser creates a thin corneal flap.
- The flap is lifted.
- An excimer laser reshapes the underlying cornea.
- The flap is repositioned without stitches.
Its potential advantages include:
- Predictable flap thickness and geometry
- No mechanical blade for flap creation
- Rapid visual recovery
- Relatively little early discomfort
- Broad treatment flexibility
- Wavefront- and topography-guided options
- A relatively straightforward enhancement pathway
Its limitations include:
- A permanent corneal flap
- Early dry-eye disturbance
- Flap displacement or folds
- Interface inflammation
- Epithelial ingrowth
- Glare and halos
- Corneal ectasia risk
- Permanent removal of corneal tissue
Femto-LASIK is generally suitable only when the patient has:
- A stable prescription
- Healthy corneal topography and tomography
- Adequate corneal tissue
- A controlled ocular surface
- No significant cataract or uncontrolled eye disease
- Realistic expectations
The use of a femtosecond laser improves flap control but does not make an unsuitable cornea safe for LASIK.
For some patients, SMILE, PRK, TransPRK or ICL may provide a better safety profile.
The safest procedure is determined by the complete examination—not by whether the clinic uses the newest laser or describes the treatment as “bladeless.”
References
- US Food and Drug Administration. ZEISS MEL 90 LASIK Patient Information Booklet. Updated 2024.
- US Food and Drug Administration. What Should I Expect Before, During and After LASIK Surgery?
- Farjo AA, Sugar A, Schallhorn SC, et al. Femtosecond Lasers for LASIK Flap Creation: A Report by the American Academy of Ophthalmology. 2013. PMID: 23174396.
- Dos Santos AM, Torricelli AAM, Marino GK, et al. Femtosecond Laser-Assisted LASIK Flap Complications. 2016. PMID: 26812715.
- Sahay P, Bafna RK, Reddy JC, Vajpayee RB, Sharma N. Complications of Laser-Assisted In Situ Keratomileusis. 2021. PMID: 34146007.
- Kahuam-López N, Navas A, Castillo-Salgado C, et al. Mechanical Microkeratome Versus Femtosecond Laser in LASIK for Myopia. Cochrane review, 2020. PMID: 32255519.
- Zhang ZH, Jin HY, Suo Y, et al. Femtosecond Laser Versus Mechanical Microkeratome for LASIK: A Meta-analysis. 2011. PMID: 22108110.
- Chen S, Feng Y, Stojanovic A, Jankov MR II, Wang Q. IntraLase Femtosecond Laser Versus Mechanical Microkeratomes in LASIK: Systematic Review and Meta-analysis. 2012. PMID: 22233436.
- Rush S, Rush RB. Patient-Reported Dry Eye Outcomes After Myopic Femtosecond LASIK. 2023. PMID: 37521150.
- Tamimi A, Abusharha A, Alabdulkader B, et al. Post-LASIK Dry Eye Disease: A Comprehensive Review of Complications and Management. 2023.
- Ahluwalia A, et al. Comparing Femtosecond LASIK and Small-Incision Lenticule Extraction. 2025. PMID: 40279261.
- Liu M, Chen Y, Wang D, et al. Clinical Outcomes After SMILE and Femtosecond Laser-Assisted LASIK for Myopia and Myopic Astigmatism. 2016. PMID: 26684046.
- Kamburoğlu G, Ertan A. Epithelial Ingrowth After Femtosecond Laser-Assisted LASIK. 2008. PMID: 19034125.
- Tăbăcaru B, Stanca HT. Intraoperative Flap-Related Complications in Femto-LASIK Surgery. 2020.
- Yan MK, Chang JS, Chan TC. Refractive Regression After LASIK. 2018. PMID: 29700964.
- Alió JL, Muftuoglu O, Ortiz D, et al. Ten-Year Follow-up of LASIK for Myopia. 2008. PMID: 18154754.
- Ikeda T, Shimizu K, Igarashi A, et al. Twelve-Year Follow-up of LASIK for Moderate to High Myopia. 2017.
- Castro-Luna G, Jiménez-Rodríguez D, Alió JL. Long-Term Safety and Effectiveness of LASIK and PRK for Myopia. 2020. PMID: 33255392.