Author: Dr Val Phua
Estimated reading time: 20 minutes
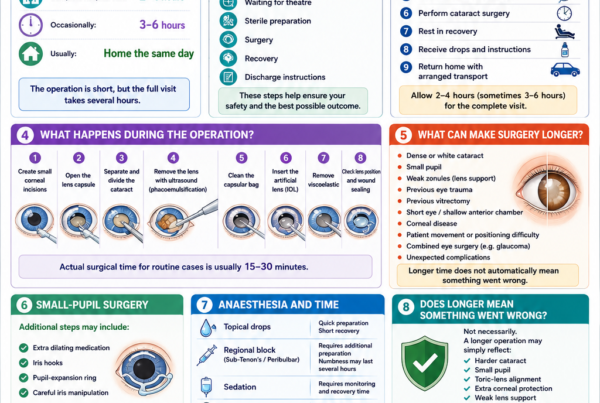
Cataract surgery is usually performed as a day procedure, which means that most patients can return home on the same day without staying overnight in hospital.
Although the operation itself is generally brief, the entire visit often takes several hours. Time is needed for registration, safety checks, pupil dilation, anaesthesia, preparation of the eye, the operation and postoperative observation.
It is normal to feel nervous before eye surgery. Many patients worry about whether the operation will be painful, whether they will see the instruments, whether they might move accidentally or whether their vision will be clear immediately afterwards.
Understanding what happens at each stage can make the experience feel more predictable and less intimidating.
This guide takes you through the typical sequence of events, beginning with your preparations at home and ending with your first evening after surgery.
The precise routine varies between surgical centres and may also depend on:
- Your general health
- The type and severity of your cataract
- Whether you have had previous eye surgery
- Whether you have glaucoma, corneal disease or retinal disease
- The type of anaesthesia being used
- Whether sedation is required
- The type of intraocular lens being implanted
- Whether your surgery is routine or technically complex
Always follow the instructions provided by your own ophthalmologist and surgical team, as these take priority over general advice.
Cataract Surgery Day at a Glance
The Usual Sequence of Events
A typical cataract surgery day involves the following stages:
- Preparing at home according to the instructions provided
- Arriving and registering at the surgical centre
- Confirming your identity, operative eye and planned lens
- Measuring your blood pressure, pulse and oxygen level
- Dilating the pupil with eye drops
- Reviewing the procedure with the surgical team
- Receiving anaesthetic eye drops and, when needed, sedation
- Entering the operating theatre
- Cleaning and covering the eye with a sterile drape
- Removing the cataract and implanting the artificial lens
- Resting in the postoperative recovery area
- Receiving eye drops, instructions and follow-up arrangements
- Returning home with an accompanying adult
You may spend much more time preparing and waiting than undergoing the operation itself. This is normal and does not indicate that anything has gone wrong.
How Long Should You Set Aside?
It is sensible to keep most of the day free, even when your surgery is scheduled in the morning.
The operating list may not always proceed at the exact appointment time because earlier patients may require additional attention or because emergency or complex cases occasionally take longer than expected.
Pupil dilation also varies between individuals. Some pupils enlarge quickly, while others require additional drops and more time.
Rather than focusing on the exact time at which the operation will begin, prepare for the visit as a complete process lasting several hours.
Before Leaving Home
Follow Your Fasting Instructions Carefully
You will be told whether you need to fast before surgery.
Fasting requirements depend partly on the type of anaesthesia planned. Some cataract operations are performed using anaesthetic eye drops alone, while others involve intravenous sedation, an anaesthetic injection around the eye or, less commonly, general anaesthesia.
Your instructions may specify:
- When to stop eating solid food
- Whether you may drink clear fluids
- When to stop drinking
- Whether morning medications may be taken with a small sip of water
- Whether special instructions apply because of diabetes
Do not assume that everyone undergoing cataract surgery follows the same fasting routine.
Some patients undergoing straightforward surgery with topical anaesthesia may not require the same fasting period as patients receiving sedation or general anaesthesia. However, you should never disregard the instructions given by your own surgical centre.
If you accidentally eat or drink during the fasting period, inform the surgical team. Do not conceal it because you are worried that your surgery may be postponed. The team needs accurate information to keep you safe.
Take Regular Medication as Directed
Many regular medications can be continued on the day of cataract surgery, but there are important exceptions.
Your ophthalmologist or anaesthetist should advise you specifically about:
- Blood-pressure medication
- Diabetes tablets
- Insulin
- Blood-thinning medication
- Antiplatelet medication
- Diuretics
- Prostate medication
- Herbal remedies
- Vitamins and supplements
- Weight-loss or diabetes injections that affect stomach emptying
Do not stop blood-thinning medication on your own.
Stopping medication such as aspirin, clopidogrel, warfarin or other anticoagulants may increase the risk of a heart attack, stroke or blood clot in some patients. The decision must be individualised according to your medical history and the planned type of anaesthesia.
Bring an updated medication list if you take several medications or cannot remember their names and doses.
Managing Diabetes on the Morning of Surgery
Patients with diabetes may require modified instructions because fasting can affect blood glucose levels.
You may be advised to:
- Omit or reduce a dose of diabetes medication
- Adjust your insulin dose
- Check your blood glucose before leaving home
- Bring your glucose meter
- Bring diabetes medication for use after the procedure
- Bring a suitable snack for after surgery
Do not make major medication changes without professional advice.
Tell the surgical team if you experience sweating, trembling, confusion, dizziness or other symptoms that could indicate low blood sugar.
Bathe and Wash Your Face Normally
You can usually shower or bathe before coming to the surgical centre unless told otherwise.
Wash your face gently and remove any debris or makeup around the eyelids. Good facial and eyelid hygiene helps reduce contamination around the surgical area.
Avoid allowing hair products, oils or creams to collect near the eye.
Avoid Makeup, Facial Creams and False Eyelashes
On the day of surgery:
- Do not wear eye makeup
- Avoid mascara and eyeliner
- Avoid heavy facial creams near the eyes
- Do not apply eyelid tape
- Remove false eyelashes if instructed
- Avoid strongly scented perfume or hair products
Cosmetics and adhesive products around the eyelids may interfere with cleaning and sterile preparation.
Some surgical centres may ask patients with eyelash extensions to remove them before surgery. Ask in advance if this applies to you.
Wear Comfortable Clothing
Choose loose and comfortable clothing.
A shirt or top that opens at the front is often more convenient than clothing that must be pulled tightly over the head. Avoid high collars that make it difficult to position monitoring equipment or reach your arm for an intravenous line.
The operating theatre may feel cool, although blankets are normally available.
Avoid bringing unnecessary valuables, large amounts of cash or expensive jewellery.
Do Not Wear Contact Lenses Unless Instructed
If you use contact lenses, you will usually have stopped wearing them before the measurements used to calculate your intraocular lens.
Do not insert a contact lens into the eye scheduled for surgery on the morning of the operation.
Ask your ophthalmologist whether you may wear a contact lens in the other eye. This can depend on whether the other eye will be needed for vision immediately after surgery and whether the lens could interfere with theatre preparation.
Bring the Necessary Documents and Medication
Depending on the surgical centre, you may need to bring:
- Your identification document
- Appointment or admission documents
- Insurance or payment documents
- A current medication list
- Your usual inhalers or essential medication
- Existing eye drops
- Allergy information
- A glasses case
- Sunglasses for the journey home
You may also be asked to bring the postoperative medication that was dispensed in advance.
Arrange for Someone to Accompany You Home
You should not drive yourself home after cataract surgery.
Your pupil may still be enlarged, your vision may be blurred and your depth perception may be temporarily altered. If you receive sedation, your reaction time and judgement may also remain affected for several hours.
Arrange for a responsible adult to:
- Accompany you home
- Help you collect medication
- Listen to the discharge instructions
- Assist with your first doses of eye drops
- Remain contactable during the first evening
Public transport may be possible for some patients when accompanied, but a private car or taxi is often more comfortable immediately after surgery.
Arriving at the Surgical Centre
Registration and Admission
When you arrive, the reception or nursing staff will confirm your identity and admission details.
You may be asked to provide or verify:
- Your full name
- Identification number
- Date of birth
- Address and contact information
- Emergency contact
- Medical conditions
- Medication history
- Drug allergies
- Previous eye operations
- The eye being treated
You may be given a wristband or another form of patient identification.
Repeated Safety Checks Are Normal
Different members of the team may repeatedly ask:
- Which eye is being operated on?
- What procedure are you having?
- Do you have any allergies?
- Are you fasting?
- Have you taken your usual medications?
- Do you have any new symptoms?
- Who is taking you home?
This repetition is deliberate.
Multiple independent checks reduce the chance of errors and allow every team member to confirm the correct patient, procedure and operative eye.
Confirmation of the Intraocular Lens Plan
The team will review the artificial lens selected for your surgery.
This may include confirming:
- The power of the intraocular lens
- The intended refractive target
- Whether the aim is distance, intermediate or near vision
- Whether monovision is planned
- Whether a toric lens is being used for astigmatism
- Whether an extended-depth-of-focus or multifocal lens is planned
The lens power is normally calculated before the day of surgery using eye measurements known as biometry.
If you remain uncertain about your visual target or lens choice, raise the question before entering the operating theatre.
The day of surgery is not the ideal time to make a rushed change, but it is always better to clarify a genuine concern than to remain silent.
Marking the Operative Eye
The eye scheduled for surgery may be marked near the eyebrow or temple.
This mark forms part of the surgical safety process and is usually made before sedation.
For a toric intraocular lens, additional markings or digital image-guidance systems may be used to help the surgeon position the lens along the correct axis of astigmatism.
Changing and Securing Personal Belongings
You may be asked to change into a surgical gown, cap or shoe covers.
Some facilities allow patients to remain in their own clothing underneath a gown. Remove spectacles, jewellery, dentures or hearing aids only when instructed.
A hearing aid may sometimes be left in the ear opposite the operative eye so that you can hear instructions during surgery. Discuss this with the nursing team.
Preoperative Medical Assessment
Checking Your Blood Pressure and Vital Signs
Before surgery, the nurses may measure your:
- Blood pressure
- Pulse
- Oxygen saturation
- Temperature
- Blood glucose, when indicated
A mildly elevated blood pressure is common because many patients feel anxious.
A single raised reading does not necessarily mean that surgery will be cancelled. The team may allow you to rest and repeat the measurement.
Very high blood pressure, chest pain, severe breathlessness or other concerning symptoms may require further medical evaluation before proceeding.
Tell the Team About Any Change in Your Health
Inform the surgical team if you have developed any new illness since your last consultation.
Important symptoms include:
- Fever
- Cough
- Flu-like symptoms
- Shortness of breath
- Chest pain
- Vomiting or diarrhoea
- Recent hospital admission
- New weakness or neurological symptoms
- A newly diagnosed medical condition
- A recent change in medication
Also report any redness, pain, discharge or infection affecting either eye.
These symptoms do not automatically mean that surgery must be postponed. The decision depends on their severity, the type of anaesthesia planned and the urgency of the operation.
Review by the Anaesthetist
Not every cataract patient requires a separate anaesthetic consultation.
However, an anaesthetist may review you if:
- Intravenous sedation is planned
- An injection around the eye is required
- General anaesthesia is planned
- You have significant medical conditions
- You have difficulty lying flat
- You are extremely anxious
- You have a movement disorder or severe tremor
- You previously had difficulty during eye surgery
Tell the anaesthetist about previous reactions to anaesthesia, severe nausea after surgery, sleep apnoea, difficult intravenous access or allergies.
Preparing the Eye for Surgery
Pupil-Dilating Eye Drops
Several rounds of eye drops may be placed into the operative eye.
These drops enlarge the pupil, allowing the surgeon to access the cataract and lens capsule more safely.
The drops may:
- Sting briefly
- Cause blurred vision
- Increase sensitivity to light
- Make near vision difficult
- Leave the pupil enlarged for several hours
Some patients require repeated drops because their pupils dilate slowly. Diabetes, certain eye conditions, previous inflammation and some medications may affect pupil dilation.
Other Preoperative Eye Drops
Depending on the surgeon’s protocol, you may also receive:
- Anaesthetic drops
- Antiseptic drops
- Anti-inflammatory drops
- Antibiotic drops
- Drops to help maintain pupil dilation
The exact combination differs between institutions.
Waiting for the Pupil to Dilate
You will usually wait in a preoperative area while the drops take effect.
This period can feel longer than expected, particularly when you are anxious. Bring a companion if permitted, and let the nurses know if you feel unwell or need assistance.
Avoid rubbing the eye after the drops have been inserted.
Final Review by the Surgeon
The ophthalmologist may review you shortly before surgery to:
- Confirm the operative eye
- Check pupil dilation
- Review the lens plan
- Confirm the intended visual target
- Answer final questions
- Perform additional markings when required
This is also an appropriate time to mention if you have difficulty lying flat, feel extremely anxious or are worried that you may cough or move.
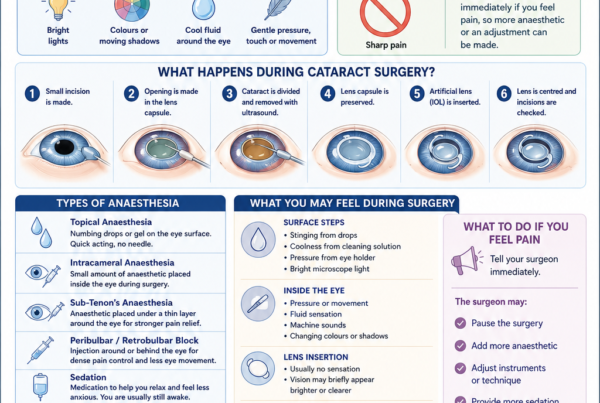
Anaesthesia for Cataract Surgery
Topical Anaesthesia
Many modern cataract operations are performed using topical anaesthesia.
Anaesthetic eye drops numb the surface of the eye without requiring an injection around it. You remain awake and can usually see light and colours during the procedure.
Topical anaesthesia generally allows rapid recovery, but it requires the patient to remain reasonably calm and cooperative.
Some sensation of pressure, touch or fluid may still be present even when the surface is adequately numb.
Intracameral Anaesthesia
The surgeon may place a small amount of anaesthetic medication inside the front part of the eye during surgery.
This is known as intracameral anaesthesia and may supplement the topical eye drops.
You will not usually be aware of this being administered.
Sub-Tenon’s or Regional Anaesthesia
Some patients receive anaesthetic medication around the eye.
A sub-Tenon’s block is delivered into a tissue space surrounding the eye. Other forms of regional anaesthesia include peribulbar or retrobulbar injections, although practice varies.
These techniques may provide stronger anaesthesia and reduce eye movement. They may be considered when:
- Surgery is expected to be complex
- The patient has difficulty controlling eye movement
- Topical anaesthesia is unsuitable
- The surgeon expects the operation to take longer
- The patient has previously experienced significant discomfort
Both topical and sub-Tenon’s anaesthesia are established approaches for cataract surgery. The most suitable method depends on the patient, surgeon and expected complexity of the procedure.
Intravenous Sedation
Sedation may be offered if you are particularly anxious.
It can help you feel calm and drowsy, but it is not the same as general anaesthesia. You will usually:
- Continue breathing independently
- Remain able to respond to instructions
- Have some awareness of the operation
- Remember all, part or very little of the experience
Sedation must be carefully adjusted. Excessive sedation may make it harder for you to cooperate, keep your head still or respond to the surgeon.
Research suggests that appropriately administered sedation can reduce fear and the intensity of visual experiences during cataract surgery under topical anaesthesia.
General Anaesthesia
General anaesthesia is not routinely required for most adult cataract operations.
It may be considered for:
- Young children
- Adults unable to cooperate
- Severe movement disorders
- Significant cognitive impairment
- Severe claustrophobia
- Extreme anxiety that cannot be managed otherwise
- Selected complex or combined procedures
General anaesthesia requires additional preparation, fasting and postoperative monitoring.
Entering the Operating Theatre
Moving onto the Operating Bed
You will be asked to lie on your back on a narrow, reclining operating bed.
Your head will be supported with a pillow or specially shaped headrest. The team may adjust your shoulders, neck and knees to make the position more comfortable.
Tell the staff if you have:
- Neck pain
- Back pain
- Arthritis
- Breathing difficulty when flat
- Heart failure
- Reflux
- Claustrophobia
- Tremor
- Parkinson’s disease
- A frequent cough
- Difficulty keeping your head still
Do not wait until the sterile drape has been placed before mentioning a positioning problem.
Monitoring Equipment
Monitoring equipment may be attached to you, including:
- A blood-pressure cuff
- A finger oxygen sensor
- Heart-monitoring stickers
- An intravenous cannula
The cuff may tighten periodically during the operation.
You may hear beeping from the monitoring equipment. These sounds are expected and do not necessarily indicate a problem.
Cleaning the Skin and Eye
The skin around your eye and the surface of the eye are cleaned with an antiseptic solution, commonly povidone-iodine.
The solution may feel cool or slightly uncomfortable. It can temporarily stain the skin around the eyelids yellow or brown.
Preoperative povidone-iodine antisepsis is one of the most strongly supported measures for reducing the risk of postoperative endophthalmitis, a rare but serious infection inside the eye.
Placement of the Sterile Drape
A sterile drape is placed over your face, leaving only the operative eye exposed.
Some patients worry that they will feel unable to breathe beneath the drape. Fresh air or oxygen is usually directed underneath it, and the drape is arranged to keep it away from the nose and mouth.
Tell the team immediately if you feel:
- Short of breath
- Claustrophobic
- Nauseated
- Unusually hot
- Unable to tolerate the position
The team can often adjust the drape or airflow.
Keeping the Eyelids Open
A small instrument called an eyelid speculum gently holds the eyelids apart.
You do not need to concentrate on keeping the eye open, and you cannot accidentally blink onto the surgical instruments.
You may be aware of mild pressure from the speculum, but it should not cause sharp pain.
What Happens During Cataract Surgery?
Creating the Corneal Incisions
The surgeon creates one or more very small openings near the edge of the cornea, the clear front window of the eye.
These incisions provide access to the cataract.
Modern cataract incisions are usually designed to seal naturally. Stitches are therefore not routinely required, although the surgeon may place a stitch if additional wound security is needed.
Filling the Eye with a Protective Gel
A clear, gel-like substance called an ophthalmic viscosurgical device is placed inside the front of the eye.
This helps:
- Maintain space inside the eye
- Protect the corneal endothelial cells
- Stabilise the anterior chamber
- Assist with lens implantation
The gel is generally removed before the operation is completed.
Opening the Lens Capsule
The cataract sits inside a thin, transparent membrane called the lens capsule.
The surgeon creates a circular opening in the front of this capsule. This step is called a capsulotomy or capsulorhexis.
The back and outer portions of the capsule are usually preserved because they form a natural support structure for the artificial lens.
Separating the Cataract
Fluid is gently introduced around the cataract to help separate it from the surrounding capsule.
This makes it easier for the surgeon to rotate and remove the cloudy lens material safely.
Breaking Up the Cataract
In standard phacoemulsification surgery, a fine ultrasonic instrument divides the cataract into smaller pieces.
The instrument simultaneously uses controlled ultrasound energy, irrigation and suction.
The amount of energy required depends partly on how dense or hard the cataract is. A soft cataract generally requires less energy than a very advanced, dense cataract.
Removing the Cataract Material
The cataract fragments are removed through the small incision.
After the firmer central portion has been removed, the surgeon carefully clears the softer outer lens material.
The transparent posterior capsule is normally left in place.
Inserting the Intraocular Lens
The intraocular lens, or IOL, is usually folded inside a delivery cartridge.
It is inserted through the small corneal incision and unfolds once inside the eye.
The surgeon positions the lens within the remaining capsule, usually in the same general location as the natural lens.
The IOL may be designed to:
- Provide clear distance vision
- Provide a planned degree of near vision
- Create monovision
- Correct corneal astigmatism
- Extend the range of vision
- Reduce dependence on reading glasses in selected patients
The artificial lens is intended to remain permanently inside the eye. It does not usually need to be cleaned, maintained or replaced.
Aligning a Toric Lens
If you are receiving a toric IOL to correct astigmatism, the surgeon rotates it to the planned axis.
Accurate alignment is important because a toric lens becomes less effective if it rotates significantly away from the intended position.
The surgeon may use preoperative ink markings, microscope guidance or a digital alignment system.
Removing the Protective Gel
The ophthalmic viscosurgical gel is removed using irrigation and aspiration.
Removing the gel helps reduce the risk of an early rise in eye pressure.
Sealing the Incisions
The surgeon checks that the incisions are secure.
Fluid may be used to hydrate the edges of the wound so that they seal. A stitch can be placed if the incision does not appear sufficiently stable.
Administering Medication
Medication may be placed inside or around the eye at the end of surgery.
Depending on the surgeon’s protocol, this may include:
- An intracameral antibiotic
- Anti-inflammatory medication
- Pupil-modifying medication
- Eye drops or ointment
Evidence supports the use of appropriate intracameral antibiotic prophylaxis as one possible strategy for reducing postoperative endophthalmitis, although the specific drug and protocol vary between institutions.
Final Checks
Before finishing, the surgeon confirms:
- The IOL is well positioned
- The pupil and anterior chamber are stable
- The incisions are secure
- There is no significant leakage
- The pressure and shape of the eye appear satisfactory
The eyelid speculum and sterile drape are then removed.
What Will You See During Cataract Surgery?
Bright Microscope Lights
Most patients see a bright light from the operating microscope.
The light may appear:
- White
- Blue
- Red
- Yellow
- Pink
- Multicoloured
Its brightness may change during different stages of the procedure.
Colours, Shadows and Patterns
You may notice:
- Moving colours
- Circular patterns
- Shadows
- Blurred shapes
- Flashes
- Changes in brightness
- A kaleidoscope-like effect
These experiences are expected and do not mean that you are seeing the operation clearly.
Most patients retain some light perception during cataract surgery under local anaesthesia, and many report colours, movement or other visual sensations.
Will You See the Surgical Instruments?
Most patients do not see the instruments in clear anatomical detail.
You may occasionally notice vague shadows or shapes, but the view is usually blurred and dominated by the microscope light.
Knowing in advance that these visual sensations can occur may make them less frightening.
What Happens When the Cataract Is Removed?
The light may temporarily become dimmer, brighter or more diffuse during different stages of the operation.
When the artificial lens is inserted, some patients notice a sudden change in brightness or clarity, while others notice no obvious change.
Every patient’s visual experience is different.
What Will You Feel During Surgery?
Pressure and Touch
You may feel:
- Gentle pressure
- Water around the eye
- Mild pulling
- Awareness of touch
- Cool fluid on the face
- The blood-pressure cuff tightening
These sensations can occur even when the eye is adequately anaesthetised.
Should Cataract Surgery Hurt?
You should not normally experience severe or sharp pain.
Mild discomfort or pressure can occur, particularly during certain stages of the operation. Pain perception varies between patients and also depends on the anaesthetic technique used.
Tell the surgeon immediately if you feel significant pain. Additional anaesthetic can often be administered.
Do not remain silent because you are worried about disturbing the operation.
Sounds in the Operating Theatre
You may hear:
- The surgeon speaking
- Nurses confirming information
- Beeping from monitoring equipment
- Sounds from the phacoemulsification machine
- Fluid or suction sounds
The theatre team may discuss surgical settings or instruments. This is normal communication and does not necessarily indicate a complication.
Following the Surgeon’s Instructions
The surgeon may ask you to:
- Look towards the microscope light
- Look slightly up, down, left or right
- Keep your head still
- Relax your shoulders
- Avoid squeezing your eyelids
- Warn the team before coughing
You do not need to maintain perfect fixation throughout every second of the operation.
Follow the instructions as calmly as possible and avoid trying to analyse every sensation.
What If You Accidentally Move?
Small movements are common and can usually be managed.
Do not suddenly sit up, turn your head or reach towards your face.
If you need to move because of discomfort, tell the surgeon first. The operation can often be paused at a safe point.
What If You Need to Cough or Sneeze?
Tell the surgeon as soon as you feel a cough or sneeze developing.
Do not try to suppress a powerful cough without warning. The surgeon can stop working momentarily, withdraw the instruments when appropriate and allow you to cough safely.
Planned movement is much safer than sudden, unexpected movement.
What If You Feel Panicked?
Tell the team immediately.
They may be able to:
- Reassure you
- Adjust the airflow
- Modify the drape
- Reposition your head
- Give additional sedation
- Pause briefly when safe
Most episodes of anxiety settle once the patient understands what is happening and receives reassurance.
Immediately After Surgery
Eye Protection
Your eye may be covered with:
- A transparent plastic shield
- An eye pad
- Protective glasses
- A combination of a pad and shield
Practices vary according to the anaesthetic used, the surgeon’s preference and the individual patient.
Evidence regarding routine eye protection after uncomplicated cataract surgery is variable, so follow the specific instructions provided by your surgeon rather than assuming that every patient needs the same protection.
Moving to the Recovery Area
You will be helped off the operating bed and brought to a recovery area.
Stand up slowly. Your balance may be temporarily affected by blurred vision, anxiety, fasting or sedation.
The nurses may monitor:
- Blood pressure
- Pulse
- Oxygen level
- Alertness
- Nausea
- Pain
- General comfort
Food and Drink
Once it is safe, you may be offered water or a light snack.
Patients with diabetes may need their blood glucose checked or may need to resume food and medication according to the anaesthetic team’s instructions.
Vision Immediately After Surgery
Do not expect the operated eye to be perfectly clear straight away.
Your vision may initially be:
- Blurred
- Hazy
- Misty
- Bright
- Washed out
- Slightly distorted
- Sensitive to light
- Tinted blue or another colour
- Obscured by an eye pad
Possible reasons include:
- Residual dilating drops
- Mild corneal swelling
- Tear-film disturbance
- Ointment on the eye
- Inflammation
- Temporary changes in eye pressure
- The eye adjusting to the new lens
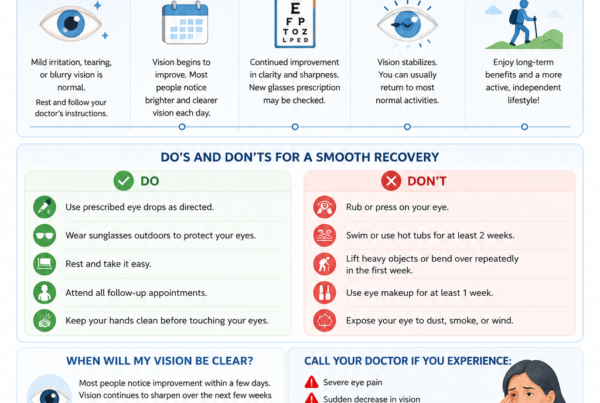
Some patients notice improved brightness almost immediately. Others require several days or longer before vision becomes clearer.
Normal Early Sensations
During the first several hours, you may notice:
- Mild grittiness
- Watering
- Slight stinging
- A foreign-body sensation
- Mild aching
- Light sensitivity
- Mild redness
- Awareness of the eyelid or shield
These symptoms should generally remain mild and gradually improve.
Severe pain is not considered a routine part of recovery and should be reported.
Before You Leave the Surgical Centre
Review of Your General Condition
Before discharge, the team will check that you are:
- Awake and comfortable
- Medically stable
- Able to stand or walk safely
- Not experiencing severe nausea
- Not experiencing unexpected pain
- Accompanied home when required
Some centres check the operated eye before discharge, while others arrange the first examination at a later follow-up visit.
Postoperative Eye Drops
You will usually be prescribed anti-inflammatory eye drops.
Depending on the surgeon’s protocol, you may also receive:
- Antibiotic eye drops
- A combined antibiotic-steroid preparation
- A non-steroidal anti-inflammatory drop
- Lubricating eye drops
- Eye-pressure-lowering drops
Before leaving, confirm:
- The name of each drop
- Which eye it is for
- How many times a day it should be used
- When the first dose should be given
- How long it should be continued
- Whether the frequency will be reduced gradually
- Whether your existing eye drops should continue
Leave approximately five minutes between different types of eye drops unless instructed otherwise.
How to Instil Eye Drops
To use eye drops:
- Wash and dry your hands.
- Tilt your head backwards or lie down.
- Gently pull the lower eyelid down.
- Place one drop into the space between the eyelid and eye.
- Avoid touching the eye or eyelashes with the bottle tip.
- Close the eye gently rather than squeezing it.
- Wipe away excess liquid with a clean tissue.
- Replace the bottle cap immediately.
One properly placed drop is usually sufficient. The eye cannot hold several full drops at once.
Follow-Up Appointment
Your follow-up appointment may be scheduled:
- Later the same day
- The following day
- Within several days
- According to an individualised schedule
Patients with glaucoma, corneal disease, diabetes, retinal disease, previous eye surgery or a complicated operation may require closer follow-up.
Do not miss the appointment simply because the eye feels comfortable.
Written Discharge Instructions
You should receive written or electronic instructions covering:
- Medication
- Eye protection
- Washing and bathing
- Exercise
- Driving
- Work
- Emergency contact details
- Warning symptoms
- Follow-up arrangements
Keep the emergency contact information somewhere easily accessible.
Going Home After Cataract Surgery
Do Not Drive
Do not drive yourself home.
Even when the operated eye seems clearer, your pupil may still be enlarged and your depth perception may be altered.
Sedation can also impair judgement and reaction time without making you feel obviously drowsy.
Wear Sunglasses if Needed
The dilated pupil and newly operated eye may be sensitive to bright light.
Sunglasses can make the journey home more comfortable, but they are not mandatory unless advised.
Walk Carefully
Your vision may be imbalanced if only one eye has been operated on, particularly when the two eyes now have very different spectacle prescriptions.
Take care with:
- Steps
- Kerbs
- Escalators
- Uneven flooring
- Bathrooms
- Poorly lit areas
Use a handrail or accept assistance when necessary.
Your First Evening at Home
Rest, but Complete Bed Rest Is Usually Unnecessary
Most patients can:
- Walk around the home
- Eat normally
- Watch television
- Use a phone briefly
- Read if comfortable
- Perform light daily activities
You do not usually need to remain in bed.
However, it is sensible to rest and avoid strenuous activity on the day of surgery.
Use the Eye Drops as Directed
Begin your postoperative medication at the time specified.
Do not delay the drops because the eye feels comfortable. Their purpose is to control inflammation and reduce the risk of complications.
Create a written schedule or phone reminder if several drops are required.
Do Not Rub or Press the Eye
The eye may feel itchy, watery or gritty as the anaesthetic wears off.
Do not:
- Rub the eye
- Press on the eyelid
- Squeeze the eyelids tightly
- Allow a child to touch the eye
- Sleep with the operated eye pressed firmly into the pillow
Use the shield at night if instructed.
Eating and Drinking
Most patients can resume a normal diet after returning home.
Start with a light meal if you have received sedation or feel nauseated.
Drink enough water unless you have been advised to restrict fluids for another medical condition.
Taking Pain Relief
Mild discomfort can often be managed with simple pain relief such as paracetamol, provided it is safe for you.
Avoid taking unfamiliar medication without checking whether it interacts with your regular medicines or medical conditions.
Increasing or severe pain requires medical assessment rather than repeated self-medication.
Sleeping Position
Many patients worry about sleeping after surgery.
Your surgeon may recommend avoiding direct pressure on the operated eye, particularly during the first few nights.
You do not usually need to sleep upright unless specifically advised. Use the protective shield if it has been prescribed.
Washing, Bathing and Personal Care
Keeping Water Out of the Eye
You can usually wash your face, but take care not to allow soap, shampoo or potentially contaminated water to enter the operated eye.
Rather than splashing water directly onto your face:
- Use a clean cloth around the eye
- Keep the eyelids gently closed
- Wipe away from the eye
- Avoid pressing on the eyelid
Showering and Washing Your Hair
Your surgeon will advise when you may shower normally.
When washing your hair during the early recovery period, tilt your head backwards so that water flows away from the face.
Avoid forceful shower spray directly onto the operated eye.
Makeup and Skin Products
Do not apply eye makeup until your surgeon says it is safe.
Mascara, eyeliner, makeup brushes and applicators can carry microorganisms and may irritate the healing eye.
Avoid applying creams or oils directly beside the eyelid incision area.
Activity After Surgery
Bending and Lifting
Advice about bending and lifting varies.
Normal gentle movements are usually acceptable, but avoid heavy lifting and strenuous exertion during the early recovery period unless your surgeon has advised otherwise.
When picking up a light object, bend your knees rather than holding your breath and straining.
Exercise
Light walking is generally reasonable when you feel steady.
More strenuous activities should be resumed gradually according to your surgeon’s advice. These may include:
- Running
- Gym workouts
- Heavy weight training
- Tennis
- Padel
- Contact sports
- Yoga positions with the head down
The appropriate timing depends on the operation and your individual recovery.
Swimming
Avoid swimming until your ophthalmologist confirms that it is safe.
Swimming pools, hot tubs, lakes and seawater can expose the healing eye to microorganisms and irritation.
Work and Screen Use
You may use a phone, tablet or computer if comfortable. Screen use does not normally damage the artificial lens or undo the surgery.
However, vision may fluctuate and the eye may tire easily.
The appropriate time to return to work depends on:
- Your occupation
- Your visual requirements
- Exposure to dust or contaminants
- Whether you operate machinery
- Whether you drive professionally
- Whether your other eye provides good vision
Driving
Do not resume driving until:
- Your vision is sufficiently clear
- You are no longer affected by sedation
- You meet the legal visual requirements
- You feel comfortable judging distance and traffic
- Your ophthalmologist has not advised against it
A patient may see well on an eye chart yet still feel uncomfortable with glare, depth perception or imbalance between the eyes.
When Should You Seek Urgent Medical Attention?
Severe or Increasing Pain
Mild irritation is common, but severe or worsening pain is not.
Contact your ophthalmologist urgently if pain:
- Becomes progressively stronger
- Prevents you from sleeping
- Is associated with nausea or vomiting
- Does not improve with the recommended medication
- Is accompanied by reduced vision
Sudden or Significant Vision Loss
Seek urgent assessment if your vision suddenly becomes much worse after initially improving, or if there is a marked reduction compared with earlier in the day.
Do not assume that sudden visual deterioration is simply part of the normal healing process.
Increasing Redness
A small amount of redness can occur after surgery.
However, rapidly increasing redness, especially when associated with pain, discharge or worsening vision, requires prompt assessment.
New Flashes, Floaters or a Curtain in the Vision
Report:
- New flashes of light
- A sudden increase in floaters
- A dark curtain or shadow
- Missing peripheral vision
These symptoms may indicate a retinal tear or retinal detachment and require urgent examination.
Discharge or Marked Swelling
Thick discharge, increasing eyelid swelling or difficulty opening the eye should be assessed.
Mild watering is common, but pus-like discharge is not.
Injury to the Operated Eye
Contact your surgical team if the eye is:
- Hit
- Scratched
- Pressed firmly
- Exposed to a chemical
- Contaminated with dirty water
- Rubbed forcefully
Do not wait for symptoms to develop after a significant injury.
Frequently Asked Questions About Cataract Surgery Day
How Long Does the Operation Take?
The cataract-removal portion of an uncomplicated operation is often brief.
However, the precise duration varies according to:
- Cataract density
- Pupil size
- Eye anatomy
- Previous surgery
- Patient cooperation
- Whether a toric or specialised lens is used
- Whether unexpected technical challenges arise
The time spent in theatre is longer than the time required to remove the cataract because preparation, sterile cleaning, anaesthesia and final checks must also be completed.
Why Am I at the Centre for Several Hours?
Most of your visit is not spent undergoing surgery.
Time is required for:
- Registration
- Repeated safety checks
- Pupil dilation
- Medical assessment
- Preparation of equipment
- Theatre scheduling
- Recovery
- Discharge counselling
This process is designed to support safety rather than speed alone.
Will I Be Awake?
Most adult patients remain awake because cataract surgery is commonly performed using local anaesthesia.
You may receive sedation to help you relax, but you will usually still be able to hear the surgeon and respond to simple instructions.
Will I See What the Surgeon Is Doing?
You will usually see bright light, colours, patterns and shadows rather than a detailed view of the surgery.
This is normal and does not mean that the anaesthetic is failing.
Can I Blink During the Operation?
The eyelid speculum keeps the eyelids open.
You do not need to prevent yourself from blinking, and you cannot accidentally close the eyelids over the instruments.
What Happens If My Eye Moves?
Small eye movements are common.
The surgeon may ask you to look in a particular direction. Try to follow the light and remain relaxed.
Tell the surgeon before making a deliberate large movement.
Is Cataract Surgery Painful?
Cataract surgery should not usually cause severe pain.
You may notice pressure, water, movement or mild discomfort. Tell the surgeon if you experience significant pain so that additional anaesthesia can be considered.
Will I Need Stitches?
Most small cataract incisions seal without stitches.
A stitch may be used if the incision requires additional support. This does not necessarily mean that a serious complication occurred.
Will My Vision Be Clear Immediately?
Some patients notice an improvement within hours. Others experience blurred vision for several days.
Recovery may be slower when there is:
- Corneal swelling
- Dry-eye disease
- A dense cataract
- Significant inflammation
- Glaucoma
- Macular disease
- Optic-nerve disease
- Previous corneal or retinal surgery
- A complicated cataract operation
Why Do Colours Look Different?
A cataract often causes gradual yellowing or dulling of colour perception.
After the cloudy lens is removed, colours may initially appear unusually bright, cool or blue. The brain generally adapts over time.
When Will I Get New Glasses?
The eye needs time to heal and the prescription needs time to stabilise.
Your ophthalmologist will advise when refraction and new glasses should be arranged. The timing may differ when the second eye is also scheduled for surgery.
What Happens If the Other Eye Is Still Blurry?
There may temporarily be a difference between the operated and unoperated eyes.
This can cause:
- Unequal image size
- Depth-perception difficulty
- Headache
- Dizziness
- Difficulty wearing old spectacles
Your ophthalmologist or optometrist can advise whether temporary spectacle modification or another visual strategy is appropriate.
Can I Be Alone on the First Night?
Some medically fit patients may manage independently, but having someone available is preferable, particularly if you:
- Received sedation
- Live alone
- Have mobility difficulties
- Have poor vision in the other eye
- Use several medications
- Have difficulty instilling eye drops
- Are at increased risk of falling
Discuss your home arrangements before surgery rather than waiting until discharge.
A Calm and Carefully Controlled Process
Cataract surgery day involves much more than the operation itself.
Each stage—from identification checks and pupil dilation to antiseptic preparation, cataract removal, lens implantation and postoperative observation—is designed to make the procedure as safe and predictable as possible.
It is normal to feel apprehensive, especially when undergoing eye surgery for the first time. Most patients find that the experience is less frightening than they imagined once the procedure begins.
Remember the most important practical points:
- Follow the fasting and medication instructions provided
- Arrange for someone to accompany you home
- Tell the team about new health problems or eye symptoms
- Inform the surgeon if you feel pain, panic or the need to cough
- Use your postoperative eye drops correctly
- Do not rub or press the operated eye
- Attend your scheduled follow-up
- Seek urgent advice for worsening pain, redness or vision
Good preparation, clear communication and appropriate postoperative care all contribute to a smoother surgical experience and recovery.
References
- Guay J, Sales K. Sub-Tenon’s anaesthesia versus topical anaesthesia for cataract surgery. Cochrane Database of Systematic Reviews. 2015;2015(8). PMID: 26308931.
- Zhao LQ, Zhu H, Zhao PQ, Wu QR, Hu YQ. Topical anesthesia versus regional anesthesia for cataract surgery: a meta-analysis of randomized controlled trials. Ophthalmology. 2012. PMID: 22365066.
- Rengaraj V, Radhakrishnan M, Au Eong KG, et al. Visual experience during phacoemulsification cataract surgery under topical anaesthesia. British Journal of Ophthalmology. 2000. PMID: 10611091.
- Au Eong KG. Visual experiences during cataract surgery: what anaesthesia providers should know. European Journal of Anaesthesiology. 2005. PMID: 15991502.
- Ciulla TA, Starr MB, Masket S. Bacterial endophthalmitis prophylaxis for cataract surgery: an evidence-based update. Ophthalmology. 2002. PMID: 11772573.
- Kessel L, Flesner P, Andresen J, Erngaard D, Tendal B, Hjortdal J. Antibiotic prevention of postcataract endophthalmitis: a systematic review and meta-analysis. Acta Ophthalmologica. 2015. PMID: 25779209.
- Dhoot AS, Popovic MM, Mihalache A, et al. Eye protection following cataract surgery: a systematic review. Canadian Journal of Ophthalmology. PMID: 34863675.
- Shoss BL, Tsai LM. Postoperative care in cataract surgery. Current Opinion in Ophthalmology. 2013. PMID: 23197268.
- Shen D, Huang W, Wei S, Zhu Y, Shi B. The impact of the Teach-back method on preoperative anxiety and surgical cooperation in elderly patients undergoing outpatient ophthalmology surgery: a randomized clinical trial. Medicine. 2023;102(8). PMID: 36827029.
- Effect of intravenous sedation on patients’ visual experience and vital signs during cataract surgery under topical anesthesia: a randomized controlled trial. PMID: 37846396.