Author: Dr Val Phua
Estimated reading time: 11–13 minutes
Sudden Dark Floaters or Hazy Vision May Be Blood Inside the Eye
A vitreous haemorrhage occurs when blood enters the vitreous cavity—the large space between the lens and the retina that is normally filled with clear gel.
Even a relatively small amount of blood can cast shadows onto the retina and cause:
- A sudden shower of dark floaters
- Cobwebs or streaks
- Red, brown or black clouds
- Hazy or smoky vision
- A marked reduction in vision
Vitreous haemorrhage is usually painless and commonly affects one eye.
The bleeding itself is not the final diagnosis. It may arise from a retinal tear, diabetic retinopathy, retinal vein occlusion, trauma or another retinal condition. Some causes require urgent laser treatment or surgery to prevent permanent visual loss.
Sudden new floaters, a dark cloud or a rapid reduction in vision should therefore be assessed promptly—even when the eye feels comfortable and does not look red.
What Is the Vitreous?
The vitreous is a transparent, gel-like substance filling most of the inside of the eye.
Light normally passes through the clear vitreous before reaching the retina.
The retina is the light-sensitive tissue lining the back of the eye. It converts light into electrical signals that travel through the optic nerve to the brain.
When blood enters the vitreous:
- Light can no longer pass through clearly.
- Blood cells cast moving shadows on the retina.
- The ophthalmologist may be unable to see the retina directly.
- An underlying retinal tear or detachment may be hidden behind the blood.
A vitreous haemorrhage does not usually mean that the vitreous gel itself is diseased. The blood generally originates from retinal vessels, abnormal new vessels or injured tissue.
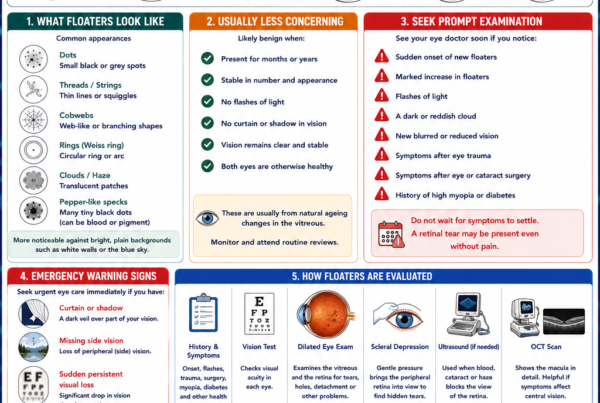
What Does Vitreous Haemorrhage Look Like?
Symptoms depend on how much blood is present and where it lies within the eye.
New Dark Floaters
Patients may suddenly see:
- Black dots
- Strings
- Cobwebs
- Curved lines
- Red or brown spots
- A pepper-like shower
A small haemorrhage may initially resemble ordinary floaters. The sudden onset, large number or dark colour makes the symptom more concerning.
A Dark Cloud or Haze
A larger bleed may appear as:
- Smoke
- Fog
- A dark cloud
- Dirty water
- A reddish or brown tint
- A moving veil across the vision
The appearance may change as blood shifts within the vitreous.
Markedly Reduced Vision
Dense haemorrhage may reduce vision to:
- Counting fingers
- Detecting hand movements
- Perceiving only light
The retina may still be functioning behind the blood. However, the final visual outcome depends on whether the underlying retina and macula remain healthy.
Floaters That Settle Temporarily
Blood cells may settle towards the bottom of the eye while a person rests, causing temporary improvement.
Movement may redistribute the blood and make the haze return.
This fluctuation does not mean that the underlying condition has resolved.
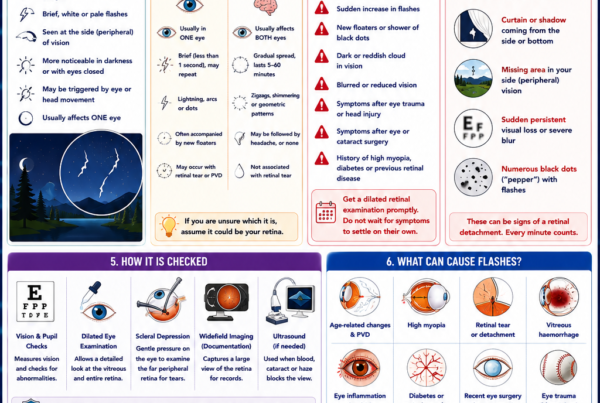
Flashes of Light
Flashes suggest that the vitreous may be pulling on the retina.
When flashes occur together with vitreous haemorrhage, a retinal tear must be excluded promptly.
A Curtain or Shadow
A curtain, shadow or missing part of the visual field may indicate that a retinal detachment has developed.
This requires emergency ophthalmic assessment.
Does Vitreous Haemorrhage Cause Pain?
Usually not.
The retina and vitreous do not produce the type of pain associated with the cornea or inflamed front of the eye.
Significant eye pain, redness, headache, nausea or marked light sensitivity may indicate an additional problem, such as:
- Neovascular glaucoma
- Uveitis
- Corneal disease
- Infection
- Trauma
- Raised eye pressure
A painful red eye with reduced vision should be assessed urgently.
When Should I Seek Urgent Eye Care?
Arrange a prompt, preferably same-day, dilated retinal examination if you develop:
- A sudden shower of new floaters
- A dark cloud or smoky haze
- Sudden painless visual loss
- Flashes of light
- A curtain or shadow
- Symptoms after eye trauma
- New floaters in an eye with diabetes
- New symptoms following eye surgery or an eye injection
Do not wait to see whether the blood clears.
A retinal tear may be hidden behind the haemorrhage. If fluid then passes through the tear, a retinal detachment can develop and threaten permanent sight loss.
What Causes Vitreous Haemorrhage?
The most common causes include:
- Proliferative diabetic retinopathy
- Posterior vitreous detachment with a retinal tear
- Retinal vein occlusion
- Eye trauma
Other causes include retinal macroaneurysms, age-related macular disease, retinal vasculitis, abnormal blood vessels and complications of eye surgery.
Posterior Vitreous Detachment and Retinal Tears
As we age, the vitreous gradually liquefies and separates from the retina. This is called a posterior vitreous detachment, or PVD.
Most PVDs occur without serious complications.
However, if the vitreous is strongly attached at one point, it may:
- Pull on a retinal blood vessel.
- Tear the vessel and cause bleeding.
- Tear the retina at the same time.
- Allow fluid to pass beneath the retina.
- Cause a retinal detachment.
The presence of vitreous haemorrhage during an acute PVD substantially increases concern for an associated retinal tear.
A careful peripheral retinal examination with scleral depression is therefore important. When blood prevents a clear view, ultrasound and repeat examinations may be required.
Proliferative Diabetic Retinopathy
Diabetic retinopathy is a major cause of vitreous haemorrhage.
When diabetes severely reduces the retina’s blood supply, the retina releases signals that stimulate the growth of abnormal new vessels.
These vessels are:
- Fragile
- Poorly supported
- Prone to leakage
- Easily torn by vitreous movement
They may bleed suddenly into the vitreous, producing dark floaters or profound visual loss.
The blood may clear temporarily, but the abnormal vessels remain and can bleed again. Scar tissue may also develop, contract and pull the retina away from the back of the eye.
Treatment is therefore directed not only at clearing the blood but also at controlling the proliferative diabetic retinopathy.
Retinal Vein Occlusion
A retinal vein occlusion blocks the normal drainage of blood from the retina.
The resulting congestion and poor oxygen supply may stimulate abnormal new blood vessels. These vessels can later bleed into the vitreous.
Vitreous haemorrhage may develop weeks or months after the initial vein occlusion, sometimes after the patient’s original blur has improved.
Patients with retinal vein occlusion therefore require continued monitoring for:
- Retinal neovascularisation
- Iris neovascularisation
- Vitreous haemorrhage
- Neovascular glaucoma
Eye Trauma
Both blunt and penetrating eye injuries can cause vitreous haemorrhage.
Examples include:
- A ball striking the eye
- Contact sports
- Falls
- Road-traffic accidents
- Workplace injuries
- Assault
- Penetrating foreign bodies
Trauma may simultaneously cause:
- Retinal tears
- Retinal dialysis
- Retinal detachment
- Choroidal rupture
- Lens damage
- Bleeding in the front of the eye
- An intraocular foreign body
A traumatic vitreous haemorrhage therefore requires a thorough examination even when some vision remains.
Retinal Macroaneurysm
A retinal arterial macroaneurysm is an abnormal dilation of a retinal artery, often associated with age and high blood pressure.
It may rupture and cause bleeding:
- Within the retina
- Beneath the retina
- In front of the retina
- Into the vitreous
Blood-pressure assessment is important when this diagnosis is suspected.
Wet Age-Related Macular Degeneration
Abnormal vessels beneath the macula may bleed through the retinal layers and occasionally extend into the vitreous.
This is less common than retinal bleeding confined around the macula but may cause sudden severe visual loss.
Retinal Vasculitis and Other Vascular Disorders
Inflammatory retinal disease may damage retinal vessels and reduce retinal circulation.
Abnormal new vessels may subsequently form and bleed.
Possible associated conditions include:
- Uveitis
- Inflammatory diseases
- Sickle-cell retinopathy
- Blood disorders
- Retinal tumours
- Certain inherited retinal diseases
Investigation is directed by the patient’s age, medical history and retinal findings.
Can Blood-Thinning Medication Cause Vitreous Haemorrhage?
Anticoagulants and antiplatelet medication may increase the amount or duration of bleeding, but they are often not the sole cause.
An underlying retinal lesion is still usually present, such as:
- A retinal tear
- Diabetic neovascularisation
- A vein occlusion
- A macroaneurysm
- Trauma
Do not stop aspirin, warfarin, apixaban, rivaroxaban, clopidogrel or another prescribed blood thinner without consulting the doctor who manages it.
Stopping medication may increase the risk of stroke, heart attack or another serious systemic event.
How Is Vitreous Haemorrhage Diagnosed?
Medical and Symptom History
The ophthalmologist will ask about:
- When the visual change began
- Floaters and flashes
- A curtain or shadow
- Diabetes
- High blood pressure
- Previous retinal disease
- Eye surgery
- Eye trauma
- Blood-thinning medication
- Previous injections or laser treatment
The pattern of symptoms helps identify the likely source.
Visual Acuity
Vision is measured in each eye.
The degree of visual loss reflects the density and location of the haemorrhage but does not by itself reveal the condition of the retina behind it.
Pupil Examination
A relative afferent pupillary defect may suggest substantial retinal or optic-nerve dysfunction rather than blood alone.
Slit-Lamp Examination
The front of the eye is examined for:
- Trauma
- Inflammation
- Abnormal iris vessels
- Cataract
- Bleeding in the anterior chamber
- Previous surgical changes
Small pigment cells or blood within the front of the vitreous may raise concern for a retinal tear.
Dilated Retinal Examination
Dilating drops enlarge the pupil so that the retina can be examined.
If the view is adequate, the ophthalmologist looks for:
- A retinal tear
- Retinal detachment
- Abnormal new vessels
- Diabetic retinopathy
- Retinal vein occlusion
- Macroaneurysm
- Retinal or choroidal bleeding
- Scar tissue
Scleral depression may be required to examine the far peripheral retina, where many retinal tears occur.
Ocular Ultrasound
When blood blocks the view of the retina, B-scan ocular ultrasound is a crucial investigation.
Ultrasound may detect:
- Retinal detachment
- Large retinal tears
- Vitreous separation
- Intraocular masses
- Choroidal detachment
- Foreign material in selected injuries
The test uses high-frequency sound waves and is usually performed with a probe placed gently over the closed eyelid or anaesthetised eye.
Ultrasound is highly useful but may not show every small retinal tear. Repeat retinal examinations or repeat ultrasound may be needed while the blood clears.
Optical Coherence Tomography
OCT may initially be impossible if the haemorrhage is dense.
Once the central retina becomes visible, OCT can assess:
- Macular swelling
- Epiretinal membranes
- Vitreomacular traction
- Tractional retinal detachment
- Macular damage from diabetes or vascular disease
Fluorescein Angiography
Fluorescein angiography may be performed after the view improves.
It can identify:
- Retinal ischaemia
- Leaking abnormal vessels
- Proliferative diabetic retinopathy
- Neovascularisation from vein occlusion
- Macroaneurysm-related leakage
The test helps guide retinal laser or other treatment.
Does Vitreous Haemorrhage Clear Naturally?
Sometimes.
The body can gradually remove blood from the vitreous cavity. Small haemorrhages may improve over days or weeks, while dense bleeding can take considerably longer.
The rate of recovery depends on:
- The quantity of blood
- Whether fresh bleeding continues
- The underlying cause
- Whether the eye has previously undergone vitrectomy
- The condition of the vitreous
- The presence of retinal traction or detachment
Visual improvement does not prove that the source has been treated. Fragile abnormal vessels may remain and bleed again.
When Can Vitreous Haemorrhage Be Observed?
Observation may be reasonable when:
- The retina is confirmed to be attached.
- No urgent retinal tear is present.
- The cause is known and stable.
- Bleeding is expected to clear.
- The patient can attend close follow-up.
- There is no macula-threatening traction.
- Useful vision in the other eye allows safe daily functioning.
Follow-up may include repeat:
- Dilated retinal examination
- Ultrasound
- OCT
- Retinal photography
- Angiography
New flashes, floaters, shadows or further visual loss require earlier reassessment.
How Is Vitreous Haemorrhage Treated?
Treatment depends entirely on the cause.
Possible approaches include:
- Observation
- Retinal laser
- Cryotherapy
- Anti-VEGF injections
- Panretinal photocoagulation
- Vitrectomy surgery
- Repair of retinal detachment
- Treatment of trauma or inflammation
Laser for a Retinal Tear
If a retinal tear is visible, laser photocoagulation may be applied around it.
The laser produces controlled scars that adhere the retina to the underlying tissue, reducing the risk of fluid passing through the tear and causing detachment.
Cryotherapy may be used when laser delivery is difficult.
A tear treated before detachment develops generally has an excellent prognosis.
Treatment for Diabetic Vitreous Haemorrhage
Treatment may include:
- Anti-VEGF injections
- Panretinal laser
- Vitrectomy with endolaser
- A combination of these approaches
Anti-VEGF Injections
Anti-VEGF medication suppresses abnormal retinal blood vessels and may reduce further bleeding while existing blood clears.
Injections do not mechanically remove blood already present.
Repeated treatment and close follow-up may be required because abnormal vessels can reactivate if treatment stops.
Panretinal Photocoagulation
Panretinal laser treats areas of poorly perfused peripheral retina.
This reduces the stimulus for abnormal new blood-vessel growth and lowers the risk of recurrent haemorrhage, retinal detachment and neovascular glaucoma.
Laser can only be applied when the retinal view is sufficiently clear, unless it is delivered internally during vitrectomy.
Anti-VEGF Versus Early Vitrectomy
A major randomised clinical trial compared aflibercept injections with prompt vitrectomy and panretinal laser for vitreous haemorrhage caused by proliferative diabetic retinopathy.
Both approaches produced similar longer-term visual outcomes for many patients.
Vitrectomy provided faster initial visual recovery, while injections allowed some patients to avoid surgery. Approximately one-third of participants eventually required both approaches during follow-up. Treatment should therefore be individualised according to the density of the bleed, retinal traction, the need for rapid visual recovery and the patient’s ability to attend repeated appointments.
Vitrectomy Surgery
Pars plana vitrectomy removes the blood-filled vitreous from the eye.
Small instruments are inserted through the white part of the eye to:
- Remove blood and vitreous gel
- Identify retinal tears
- Relieve vitreoretinal traction
- Remove scar tissue
- Apply retinal laser
- Repair retinal detachment
- Insert gas or silicone oil when necessary
Vitrectomy is commonly considered when:
- The haemorrhage is dense and not clearing.
- A retinal tear or detachment is present or strongly suspected.
- Ultrasound suggests retinal traction.
- Proliferative diabetic retinopathy remains active.
- Recurrent haemorrhages affect useful vision.
- Both eyes are significantly impaired.
- Rapid visual rehabilitation is particularly important.
- The underlying cause cannot be safely treated through the blood.
Vitrectomy clears the visual pathway, but the final vision depends on the health of the retina beneath the blood.
What Happens During Vitrectomy?
The procedure is commonly performed as day surgery under local anaesthesia with sedation, although general anaesthesia may be used in selected patients.
The surgeon:
- Creates very small openings in the white of the eye.
- Removes the blood and vitreous gel.
- Examines the retina directly.
- Treats tears, abnormal vessels or scar tissue.
- Applies internal retinal laser when needed.
- Leaves the eye filled with fluid, gas or silicone oil.
A gas bubble or silicone oil is not required for every vitreous haemorrhage. It is used when additional internal retinal support is needed.
What Are the Risks of Vitrectomy?
Possible complications include:
- Cataract progression
- Retinal tear
- Retinal detachment
- Recurrent bleeding
- Raised or reduced eye pressure
- Infection
- Macular swelling
- Scar-tissue formation
- Loss of vision
The risks are weighed against the danger of untreated retinal disease and prolonged visual loss.
What If a Gas Bubble Is Used?
When gas is placed in the eye:
- Vision remains blurred while the bubble is present.
- Specific head positioning may be required.
- Air travel and substantial altitude changes are prohibited.
- Scuba diving is prohibited.
- Nitrous oxide anaesthesia must not be used.
Gas expands when atmospheric pressure falls and may cause a dangerous increase in eye pressure.
The restrictions remain until the surgeon confirms that the bubble has completely disappeared.
Will My Vision Return to Normal?
Visual recovery depends more on the underlying retinal condition than on the quantity of blood alone.
A patient whose retina and macula remain healthy may recover excellent vision after the blood clears or is removed.
Vision may remain limited when there is:
- Macular ischaemia
- Diabetic macular oedema
- Retinal detachment
- Macular scarring
- Optic-nerve damage
- Severe retinal vein occlusion
- Tractional damage
- Age-related macular disease
Removing blood restores the pathway for light but cannot regenerate retinal tissue already permanently damaged.
Can Vitreous Haemorrhage Recur?
Yes.
Recurrent bleeding may occur when:
- Diabetic neovascularisation remains active.
- Panretinal laser is incomplete.
- A vein occlusion produces new vessels.
- Scar tissue continues pulling on vessels.
- A retinal tear has not been treated.
- Blood pressure remains severely uncontrolled.
- New trauma occurs.
Treating the source is therefore essential.
Vitrectomy alone clears the blood; additional laser, injections or membrane removal may be needed to reduce recurrence.
What Can I Do While Waiting for the Blood to Clear?
Follow the ophthalmologist’s individual instructions.
General considerations include:
- Attend every scheduled review.
- Avoid driving when vision is unsafe.
- Continue prescribed diabetes and blood-pressure medication.
- Do not stop blood thinners without medical advice.
- Protect the eye from further injury.
- Report new flashes, shadows or worsening vision immediately.
- Follow any temporary activity restrictions given by the retina specialist.
Do not rely on supplements, eye exercises or over-the-counter eye drops to dissolve blood inside the vitreous.
Should I Avoid Exercise?
The advice depends on the cause.
The ophthalmologist may temporarily restrict strenuous exercise, heavy lifting or contact sports when:
- A retinal tear is suspected.
- Fresh bleeding is present.
- Trauma caused the haemorrhage.
- Retinal surgery has recently been performed.
- Significant abnormal vessels remain untreated.
Ordinary walking and light activity may be acceptable in stable cases, but individual instructions should take priority.
Can I Fly with Vitreous Haemorrhage?
Vitreous haemorrhage alone does not usually expand at altitude.
However:
- Vision may be too poor for safe independent travel.
- Urgent follow-up or surgery may be required.
- Air travel is prohibited if a gas bubble was placed during surgery.
Confirm travel plans with the treating ophthalmologist.
Can I Drive?
Do not drive if:
- Vision is significantly reduced.
- A dense cloud obstructs the visual field.
- Depth perception is impaired.
- Both eyes are affected.
- Dilating drops are still active.
- You do not meet the legal vision requirements for driving.
Vision may fluctuate as blood moves, so temporary improvement does not necessarily make driving safe.
What Medical Conditions Should Be Reviewed?
Depending on the suspected cause, medical assessment may include:
- Blood pressure
- Blood glucose and HbA1c
- Cholesterol
- Blood count
- Kidney function
- Blood-clotting history
- Medication review
- Investigation for inflammatory or blood disorders
The testing should be tailored to the clinical situation rather than applying an extensive standard panel to every patient.
Warning Signs During Follow-Up
Seek urgent assessment if you develop:
- A new curtain or shadow
- Increasing flashes
- A sudden increase in dark floaters
- Further loss of vision
- Significant eye pain
- Redness with headache or nausea
- Marked light sensitivity
- New symptoms following an injection or surgery
These may indicate retinal detachment, recurrent bleeding, raised eye pressure, inflammation or infection.
Frequently Asked Questions
Is vitreous haemorrhage an emergency?
It requires prompt assessment because a retinal tear or detachment may be hidden behind the blood.
A curtain, shadow or rapidly worsening vision requires emergency care.
Can a small bleed clear by itself?
Yes.
Small haemorrhages may clear without surgery, but the cause must still be identified and treated when necessary.
Can eye drops clear vitreous blood?
No.
Eye drops do not penetrate the vitreous in a way that dissolves the blood.
How long does the blood take to clear?
It may take days, weeks or months depending on the density, cause and whether further bleeding occurs.
Dense or recurrent haemorrhage may not clear sufficiently without vitrectomy.
Will drinking more water clear the haemorrhage faster?
No evidence shows that increased water intake meaningfully accelerates clearance of blood from the vitreous.
Should I stop aspirin or blood thinners?
Not without medical advice.
The underlying retinal cause still needs evaluation, and abruptly stopping medication may create serious systemic risks.
Why does my vision improve in the morning and worsen later?
Blood may settle while you are lying still and redistribute when you move around.
This does not mean the bleeding has resolved.
Can vitreous haemorrhage cause permanent blindness?
The blood itself may clear without permanent damage, but the underlying cause—such as retinal detachment, severe diabetes or retinal ischaemia—can permanently impair vision.
Is vitrectomy always required?
No.
Observation may be appropriate when the retina is attached, the source is controlled and the blood is clearing. Surgery is considered when the haemorrhage is persistent, recurrent or associated with dangerous retinal disease.
Can the other eye be affected?
Yes, particularly when the cause is diabetes, retinal vein occlusion, high myopia or another systemic retinal disease.
Both eyes should be examined and monitored as advised.
The Bottom Line
Vitreous haemorrhage is bleeding into the normally clear gel filling the back of the eye.
It may cause:
- Sudden dark floaters
- Cobwebs
- Smoky or hazy vision
- A dark cloud
- Severe painless visual loss
Common causes include:
- Proliferative diabetic retinopathy
- Posterior vitreous detachment with a retinal tear
- Retinal vein occlusion
- Eye trauma
The blood may clear naturally, but treatment must address the underlying cause.
Management may include:
- Observation
- Retinal laser or cryotherapy
- Anti-VEGF injections
- Panretinal laser
- Vitrectomy
- Retinal-detachment repair
Do not wait for the blood to clear before seeking an examination. A retinal tear or detachment may be hidden behind it, and early treatment provides the best chance of protecting vision.
References
- Shaikh N, et al. Vitreous Hemorrhage: Causes, Diagnosis and Management. Indian Journal of Ophthalmology. 2023.
- Kim SJ, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern. Ophthalmology. 2025.
- Lim JI, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025.
- National Eye Institute. Diabetic Retinopathy. Updated September 2025.
- American Society of Retina Specialists. Retinal Tears.
- American Society of Retina Specialists. Vitrectomy.
- Antoszyk AN, et al. Aflibercept Versus Vitrectomy With Panretinal Photocoagulation for Vitreous Haemorrhage From Proliferative Diabetic Retinopathy. JAMA. 2020.
- American Society of Retina Specialists. Advanced Retinal Imaging.