Author: Dr Val Phua
Estimated reading time: 14–16 minutes
What Is Laser Treatment for Glaucoma?
Laser glaucoma treatment uses precisely focused light energy to alter a specific structure inside or around the eye.
Depending on the type of glaucoma, laser treatment may:
- Improve drainage through the trabecular meshwork
- Create an alternative route for fluid through the iris
- Pull the peripheral iris away from the drainage angle
- Reduce aqueous-fluid production by treating the ciliary body
- Lower eye pressure
- Reduce reliance on daily eye drops
- Delay or reduce the need for glaucoma surgery
Laser treatment cannot usually:
- Reverse optic-nerve damage
- Restore an established visual-field defect
- Cure glaucoma permanently
- Guarantee that eye drops will never be required
- Remove the need for lifelong monitoring
The National Eye Institute describes glaucoma laser treatment as an office-based procedure that can improve fluid drainage and lower pressure in selected types of glaucoma. Glaucoma remains a chronic condition even when the laser response is successful.
Is Glaucoma Laser the Same as LASIK?
No.
Glaucoma lasers and refractive lasers have very different purposes.
LASIK, PRK and SMILE
These procedures reshape the cornea to correct:
- Short-sightedness
- Long-sightedness
- Astigmatism
They aim to reduce spectacle dependence.
Glaucoma Laser Treatment
Glaucoma lasers target structures involved in eye-pressure regulation, such as:
- The trabecular meshwork
- The peripheral iris
- The ciliary body
They aim to preserve the optic nerve by lowering pressure or relieving angle obstruction.
Glaucoma laser treatment does not correct the spectacle prescription.
Why Is Eye Pressure Lowered?
Glaucoma progressively damages the optic nerve.
Eye pressure is the principal modifiable risk factor. Lowering pressure can reduce the likelihood of further structural and visual-field loss, even when the starting pressure falls within the usual statistical range.
The target pressure depends on:
- Untreated pressure
- Glaucoma severity
- Visual-field damage
- OCT progression
- Age and life expectancy
- Rate of deterioration
- Corneal thickness
- Glaucoma type
- Previous treatment
The aim is not simply to obtain a pressure below 21 mmHg. It is to reach a level that is sufficiently safe for that individual optic nerve.
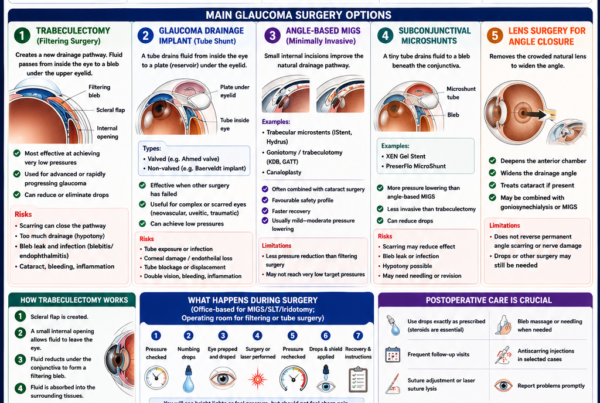
What Are the Main Types of Glaucoma Laser Treatment?
The principal laser procedures are:
- Selective laser trabeculoplasty
- Laser peripheral iridotomy
- Laser peripheral iridoplasty
- Transscleral cyclophotocoagulation
- Endoscopic cyclophotocoagulation
They are not interchangeable.
Each treats a different glaucoma mechanism.
Selective Laser Trabeculoplasty
Selective laser trabeculoplasty, usually abbreviated as SLT, treats the trabecular meshwork—the main drainage tissue in an eye with an open drainage angle.
SLT is commonly used for:
- Primary open-angle glaucoma
- Normal-tension glaucoma
- Ocular hypertension
- Pseudoexfoliative glaucoma
- Pigmentary glaucoma
- Selected secondary open-angle glaucomas
It may be used:
- As the first treatment
- Instead of starting daily drops
- In addition to existing drops
- When drops cause side effects
- When medication adherence is difficult
- When pressure remains above target
NICE recommends offering 360-degree SLT as first-line treatment in many people with newly diagnosed ocular hypertension at risk of visual impairment and in non-advanced chronic open-angle glaucoma. The guideline was reviewed in March 2025.
How Does SLT Work?
SLT applies short, low-energy laser pulses to pigmented cells within the trabecular meshwork.
The treatment does not drill open a physical drainage hole.
Instead, it triggers biological changes involving:
- Cellular signalling
- Macrophage recruitment
- Remodelling of the trabecular meshwork
- Improved aqueous outflow
The word selective refers to the laser’s preferential interaction with pigmented cells while limiting thermal damage to surrounding tissue.
This relatively non-destructive mechanism is one reason SLT can sometimes be repeated.
How Is SLT Performed?
SLT is usually performed in an outpatient clinic.
The usual steps are:
- Eye pressure is measured.
- A numbing eye drop is applied.
- A pressure-lowering drop may be given before treatment.
- The patient sits at a laser machine similar to a slit lamp.
- A mirrored contact lens is placed gently on the eye.
- The doctor views the drainage angle through the mirror.
- Laser applications are delivered around part or all of the trabecular meshwork.
- Pressure may be rechecked after treatment.
The procedure commonly takes several minutes per eye.
The patient sees flashes of light but should not feel each laser pulse.
Is SLT Painful?
Most patients experience little or no pain.
Possible sensations include:
- Pressure from the contact lens
- Mild stinging from the drops
- Awareness of bright flashes
- A mild ache later that day
- A gritty sensation
Severe pain is not typical and should be reported.
How Much Can SLT Lower Eye Pressure?
The response varies.
A commonly expected reduction is approximately 20% to 30% from the pretreatment pressure in a responsive eye.
The reduction is often greater when:
- Starting pressure is higher
- The angle is open and accessible
- The trabecular meshwork is suitably pigmented
- The eye has not already reached a very low pressure
- The procedure treats an adequate portion of the angle
A patient starting at 28 mmHg may experience a larger numerical reduction than someone starting at 15 mmHg.
SLT may have a smaller absolute effect in normal-tension glaucoma because the starting pressure is already relatively low.
Does SLT Work Immediately?
Not always.
Pressure may begin falling within days, but the full response may require several weeks.
An early pressure check may be arranged to exclude a post-laser spike.
A later review determines:
- Whether pressure reached the target
- Whether drops can be reduced
- Whether additional treatment is required
- Whether the fellow eye should be treated
Patients should normally continue their existing glaucoma medication until specifically advised to change it.
How Effective Is SLT Compared with Eye Drops?
The LiGHT randomised trial compared first-line SLT with first-line pressure-lowering drops in people with newly diagnosed open-angle glaucoma or ocular hypertension.
At six years, SLT provided safe and effective pressure control, better long-term disease control and a reduced need for incisional glaucoma and cataract surgery compared with the initial medication pathway. Many laser-treated eyes remained controlled without daily pressure-lowering medication.
A 2024 systematic review similarly found that SLT was associated with fewer glaucoma operations, fewer glaucoma medications and fewer ocular adverse effects than medication-based treatment in the reviewed studies.
These results do not mean that drops are ineffective.
Drops remain important when:
- SLT is unsuitable
- The laser response is incomplete
- A very low target is required
- The angle cannot be treated adequately
- Several mechanisms are contributing to pressure elevation
Does SLT Prevent Glaucoma Progression?
SLT lowers the principal modifiable risk factor rather than directly repairing the optic nerve.
If the pressure reduction is sufficient, it can reduce the likelihood of further damage.
A 2026 analysis of the LiGHT trial reported slower visual-field progression in the SLT-first pathway than in the medication-first pathway over six years.
However, progression can still occur when:
- The pressure reduction is insufficient
- Pressure later rises again
- Glaucoma is very aggressive
- The disease was already advanced
- Pressure peaks occur outside clinic hours
- The optic nerve is unusually vulnerable
OCT and visual-field monitoring must continue after successful laser.
Does SLT Work for Everyone?
No.
Some eyes respond strongly, some moderately and some minimally.
Possible reasons for a limited response include:
- Low starting pressure
- Inaccessible or closed drainage angle
- Extensive peripheral anterior synechiae
- Advanced outflow damage
- Previous treatment history
- Individual biological variation
- Certain secondary glaucoma mechanisms
SLT cannot be performed effectively if the trabecular meshwork cannot be seen adequately during gonioscopy.
How Long Does the SLT Effect Last?
The duration varies.
The pressure-lowering effect may last:
- Several months
- Several years
- Longer in selected patients
The effect can gradually diminish as the drainage system continues ageing or disease progresses.
Continued pressure checks remain necessary.
Can SLT Be Repeated?
Yes, in selected patients.
Because SLT causes less permanent thermal disruption than older argon laser trabeculoplasty, it can often be repeated when:
- The first treatment worked
- Pressure later rises
- The angle remains accessible
- The doctor believes further response is likely
Studies have shown that repeat SLT can restore pressure control in some eyes and may produce an effect comparable to the initial treatment.
A repeat response is not guaranteed.
Can SLT Be Done After Glaucoma Drops Have Started?
Yes.
SLT can be added when:
- Pressure remains above target
- Medication causes irritation
- The patient wants fewer bottles
- Adherence is difficult
- A fixed combination is being considered
A 2025 LiGHT-related analysis found that escalation to SLT after initial medication produced an average pressure reduction of approximately 4.6 mmHg, or 21.8%, in the studied eyes. Many reached target without incisional surgery.
Can Drops Be Stopped After SLT?
Sometimes.
The decision depends on:
- Pressure after treatment
- Target pressure
- Number of current medications
- Severity of glaucoma
- Condition of the other eye
- SLT response over time
Patients should not stop drops on the day of laser unless specifically instructed.
The doctor may:
- Continue all medication initially
- Reduce one medication later
- Stop medication if pressure remains safely controlled
- Continue drops because the combined effect is required
What Are the Risks of SLT?
SLT is generally considered safe, but no procedure is risk-free.
Possible effects include:
- Temporary eye-pressure elevation
- Mild anterior-chamber inflammation
- Redness
- Light sensitivity
- Mild ache
- Temporary blurred vision
- Corneal surface irritation
- Headache
- Incomplete pressure reduction
- Loss of effect over time
Less common complications include:
- A significant pressure spike requiring medication
- Corneal swelling
- Hyphema or bleeding
- Persistent inflammation
- Peripheral anterior synechiae
- Very rare sustained corneal changes
Modern reviews describe transient pressure spikes, redness, blur and anterior-segment inflammation as the principal complications.
Who Has a Greater Risk of a Pressure Spike After SLT?
Additional precautions may be taken in eyes with:
- Heavily pigmented trabecular meshwork
- Pigmentary glaucoma
- Pseudoexfoliation
- High pretreatment pressure
- Advanced optic-nerve damage
- Previous large pressure responses
A pressure-lowering drop may be given before or after treatment.
Some patients are monitored in the clinic for longer.
Will I Need Anti-Inflammatory Drops After SLT?
Practice varies.
The doctor may prescribe:
- A short course of steroid drops
- A non-steroidal anti-inflammatory drop
- No routine anti-inflammatory medication
The decision depends on:
- Laser energy
- Degree of inflammation
- Patient symptoms
- Glaucoma type
- The clinician’s protocol
Use only the prescribed drops.
Steroids can raise eye pressure in susceptible patients and should not be continued beyond instructions.
What Is Argon Laser Trabeculoplasty?
Argon laser trabeculoplasty, or ALT, is an older treatment for open-angle glaucoma.
ALT applies thermal laser burns to the trabecular meshwork.
It can lower pressure but causes more permanent tissue alteration than SLT and has less repeatability.
SLT has largely replaced ALT in many centres because it provides comparable pressure lowering with less thermal damage.
What Is Micropulse Laser Trabeculoplasty?
Micropulse laser trabeculoplasty delivers laser energy in very short bursts separated by rest periods.
The aim is to reduce heat accumulation within the trabecular meshwork.
Evidence is developing, but the treatment is less established than conventional SLT.
A 2024 systematic review found that micropulse trabeculoplasty and SLT could both lower pressure, with differences depending on the included studies and treatment protocols.
What Is Direct Selective Laser Trabeculoplasty?
Direct selective laser trabeculoplasty, or DSLT, delivers treatment through the limbus without using the traditional mirrored contact lens to visualise the angle.
Potential advantages include:
- Shorter treatment
- Less contact with the eye
- Easier delivery in high-volume settings
- Reduced dependence on operator gonioscopic technique
A 2025 randomised trial found that DSLT was well tolerated and produced sustained pressure reduction through 12 months. It did not meet the study’s prespecified six-month non-inferiority endpoint compared with conventional SLT, so the two procedures should not yet be assumed to be equivalent in every setting.
Conventional SLT remains the more established procedure.
Laser Peripheral Iridotomy
Laser peripheral iridotomy, abbreviated as LPI or sometimes PI, creates a small full-thickness opening in the peripheral iris.
It is used mainly for glaucoma related to narrow or closed drainage angles.
The opening allows aqueous fluid to move directly from behind the iris into the anterior chamber.
This equalises pressure across the iris and reduces forward bowing caused by pupillary block.
HealthHub describes peripheral iridotomy as an important laser treatment in angle-closure glaucoma.
Who May Need Laser Iridotomy?
LPI may be recommended for:
- Acute primary angle closure
- The fellow eye after an acute angle-closure attack
- Primary angle closure
- Primary angle-closure glaucoma
- Selected primary angle-closure suspects
- Intermittent angle-closure symptoms
- Pupillary-block mechanisms
- Selected plateau-iris cases as an initial step
- Certain secondary pupillary-block conditions
Not everyone with a shallow anterior chamber automatically requires laser.
The decision depends on:
- Gonioscopy
- Extent of iridotrabecular contact
- Pressure
- Peripheral anterior synechiae
- Symptoms
- Lens size
- Need for repeated pupil dilation
- Access to emergency care
- Risk in the fellow eye
How Is Laser Iridotomy Performed?
The usual steps are:
- Eye pressure is checked.
- A drop may be used to make the pupil smaller.
- A numbing drop is applied.
- The patient sits at the laser machine.
- A special contact lens is placed on the cornea.
- The doctor selects a thin peripheral area of iris.
- Argon laser may be used first to thin or coagulate the iris.
- A YAG laser creates a full-thickness opening.
- Pressure is rechecked after treatment.
- Anti-inflammatory drops are prescribed.
The opening is usually placed beneath the upper eyelid when anatomy permits.
Is Laser Iridotomy Painful?
Most patients experience little pain.
Possible sensations include:
- Pressure from the contact lens
- A brief sharp or pinching feeling
- Bright flashes
- Mild headache
- Brow ache
- Grittiness later that day
Significant persistent pain requires reassessment.
Does Iridotomy Lower Eye Pressure?
It may.
Its primary purpose is to relieve pupillary block and reduce the risk of angle closure.
Pressure may fall when pupillary block was the principal cause.
However, pressure can remain elevated because of:
- Permanent angle scarring
- Peripheral anterior synechiae
- Trabecular-meshwork damage
- Plateau iris
- A large or anteriorly positioned lens
- Coexisting open-angle glaucoma
- Previous acute pressure damage
LPI does not guarantee that glaucoma drops or further treatment will be unnecessary.
Does Iridotomy Open the Angle Completely?
Not always.
The angle may remain narrow after a patent iridotomy because of:
- Plateau-iris configuration
- Lens vault
- Thick peripheral iris
- Anteriorly positioned ciliary processes
- Peripheral anterior synechiae
Long-term data and Asian studies have shown that residual angle narrowing may persist in a meaningful proportion of treated eyes.
The angle should therefore be reassessed after LPI using gonioscopy.
Does Every Person with Narrow Angles Need Preventive Iridotomy?
No.
Large preventive trials have shown that many low-risk primary angle-closure suspects have a relatively low absolute risk of progressing over several years, even though LPI reduces that risk.
Observation may be reasonable in selected low-risk patients when:
- Pressure is normal
- No peripheral anterior synechiae are present
- No glaucomatous damage is present
- The patient has no angle-closure symptoms
- Reliable follow-up is available
Preventive LPI may be favoured when:
- The fellow eye has suffered an acute attack
- The angle is extremely narrow
- Pressure is elevated
- Synechiae are present
- Intermittent symptoms occur
- Repeated pupil dilation is required
- The patient takes medications that may precipitate closure
- Emergency ophthalmic care may be difficult to access
The decision should be individualised.
What Are the Risks of Laser Iridotomy?
Possible complications include:
- Temporary eye-pressure elevation
- Mild inflammation
- Small amounts of bleeding from the iris
- Temporary blurred vision
- Light sensitivity
- Corneal irritation
- Headache or brow ache
- Closure of the opening
- Need for repeat laser
- Glare, halos, lines or other dysphotopsias
An American Academy of Ophthalmology review reported transient pressure spikes, anterior-chamber bleeding and dysphotopsias among recognised complications. Most bleeding is minor and stops during the procedure.
Rare complications include:
- Corneal endothelial injury
- Cataract progression
- Cystoid macular oedema
- Retinal haemorrhage
- Persistent inflammation
- Aqueous misdirection in anatomically predisposed eyes
Why Might I See a Line or Glare After Iridotomy?
Light may occasionally pass through the iridotomy opening and create:
- A horizontal line
- A crescent
- Glare
- Ghosting
- A bright spot
These symptoms are called dysphotopsias.
They may improve as the brain adapts.
Persistent symptoms should be discussed because:
- The opening may be exposed by the eyelid margin.
- Dry eye or cataract may also contribute.
- Additional evaluation may be needed.
Can the Iridotomy Hole Close?
Yes.
Closure is more likely when:
- The opening was very small
- The iris is thick or heavily pigmented
- Inflammation occurs
- Pigment or tissue blocks the opening
A repeat laser may be required.
A patent opening can usually be confirmed by slit-lamp examination.
Does Iridotomy Cure Angle-Closure Glaucoma?
No.
It treats the pupillary-block component.
The patient may still require:
- Pressure-lowering eye drops
- Laser iridoplasty
- Cataract or lens surgery
- Goniosynechialysis
- Trabeculectomy
- A glaucoma drainage implant
- Continued OCT and visual-field monitoring
Existing optic-nerve damage remains irreversible.
Can Cataract or Lens Surgery Be Better Than Iridotomy?
In selected patients with established primary angle closure and significant pressure elevation or glaucoma, lens extraction may provide better anatomical opening and long-term pressure control than iridotomy alone.
The EAGLE randomised trial found that early clear-lens extraction produced better pressure control and patient-reported outcomes than standard care beginning with LPI in patients with primary angle closure with pressure above 30 mmHg or primary angle-closure glaucoma.
This does not mean every narrow-angle patient should undergo lens surgery.
The decision depends on:
- Age
- Cataract
- Visual symptoms
- Pressure
- Extent of angle closure
- Glaucoma damage
- Surgical risk
- Refractive consequences
Laser Peripheral Iridoplasty
Laser peripheral iridoplasty, also called argon laser peripheral iridoplasty or ALPI, applies low-energy contraction burns to the far peripheral iris.
The burns shrink the peripheral iris tissue and pull it away from the drainage angle.
Unlike iridotomy, iridoplasty does not create a hole through the iris.
When Is Iridoplasty Used?
Possible indications include:
- Persistent appositional angle closure after a patent iridotomy
- Plateau-iris syndrome
- Acute angle closure when iridotomy cannot initially be performed
- An angle that remains dangerously narrow despite relieving pupillary block
- Selected small or anatomically crowded eyes
- Iris or ciliary-body cyst-related narrowing
Current references generally position iridoplasty as a second-line procedure for residual appositional closure after iridotomy.
How Does Iridoplasty Differ from Iridotomy?
Iridotomy
- Creates a full-thickness iris opening
- Relieves pupillary block
- Equalises pressure across the iris
Iridoplasty
- Applies contraction burns to the peripheral iris
- Pulls the iris away from the angle
- Addresses residual appositional crowding
The two procedures may be complementary.
Does Iridoplasty Provide Permanent Control?
Not always.
It can widen the angle, particularly in plateau iris or acute appositional closure.
Long-term pressure benefit is less certain, and the angle can narrow again.
A Cochrane review found insufficient evidence that iridoplasty provides superior long-term control over alternative treatments for chronic angle closure.
Continued gonioscopy and pressure monitoring remain necessary.
What Are the Risks of Iridoplasty?
Possible effects include:
- Temporary inflammation
- Pressure elevation
- Eye ache
- Pupil distortion
- Iris atrophy
- Corneal burns if the view is poor
- Temporary visual blur
- An inadequate angle-opening response
Severe complications are uncommon when the procedure is properly performed, but long-term evidence is less extensive than for SLT or LPI.
Cyclophotocoagulation
Cyclophotocoagulation, or CPC, lowers eye pressure by treating the ciliary body.
The ciliary body produces aqueous fluid.
By reducing the activity of part of the ciliary processes, CPC decreases fluid production and lowers pressure.
The principal forms include:
- Continuous-wave transscleral cyclophotocoagulation
- Slow-coagulation transscleral cyclophotocoagulation
- Micropulse transscleral laser treatment
- Endoscopic cyclophotocoagulation
What Is Transscleral Cyclophotocoagulation?
In transscleral CPC, laser energy is delivered through the white wall of the eye—the sclera—to the ciliary body beneath it.
The surgeon positions the probe around the eye and treats selected regions while avoiding important structures.
The procedure is generally performed with:
- Local anaesthesia
- Sedation
- Occasionally general anaesthesia
Unlike SLT or LPI, transscleral CPC is usually performed in an operating-room or procedure-room setting rather than at a standard slit-lamp laser.
What Is Continuous-Wave CPC?
Continuous-wave CPC delivers sustained diode-laser energy to individual treatment locations.
It can produce substantial pressure reduction.
Historically, it was often reserved for:
- Refractory glaucoma
- Painful eyes with poor visual potential
- Eyes in which other surgery had failed
- Neovascular glaucoma
- Eyes unsuitable for incisional surgery
Modern techniques and adjusted energy settings have expanded its use to selected eyes with useful vision, but the procedure remains more destructive than SLT or iridotomy.
What Is Slow-Coagulation CPC?
Slow-coagulation CPC uses lower power for a longer duration at each treatment location.
The aim is to create a more controlled thermal effect and reduce explosive tissue disruption.
It may be considered in refractory glaucoma and in eyes where conventional continuous-wave treatment carries greater concern.
Technique and settings vary between surgeons.
What Is Micropulse Cyclophotocoagulation?
Micropulse transscleral laser treatment divides laser energy into repeated short bursts separated by rest periods.
During the “off” periods, tissue can partially cool.
The aim is to reduce aqueous production and alter outflow while limiting collateral thermal damage.
Potential advantages include:
- Less postoperative inflammation
- Less pain
- Lower risk of severe hypotony
- Suitability for selected eyes with useful vision
- Repeatability
A 2025 systematic review found broadly similar pressure-lowering efficacy between micropulse and continuous-wave treatments in refractory glaucoma, with a more favourable safety profile for micropulse treatment.
A 2026 meta-analysis similarly reported comparable efficacy with fewer complications in the micropulse group, although treatment protocols and glaucoma types varied.
Is Micropulse Always Better Than Continuous-Wave CPC?
No.
Micropulse may have a gentler safety profile, but:
- Pressure reduction may be less predictable.
- Retreatment may be required.
- Some refractory glaucomas may respond more strongly to continuous-wave treatment.
- Energy settings vary significantly.
- Study populations are heterogeneous.
A 2024 comparative study suggested that continuous-wave treatment may provide stronger control in selected glaucoma subtypes, although subgroup sizes were limited.
The choice depends on:
- Glaucoma type
- Target pressure
- Visual potential
- Previous surgery
- Risk of hypotony
- Surgeon experience
What Is Endoscopic Cyclophotocoagulation?
Endoscopic cyclophotocoagulation, or ECP, treats the ciliary processes from inside the eye.
A small camera and laser probe are introduced through an incision, allowing the surgeon to view the ciliary processes directly.
ECP is commonly performed:
- With cataract surgery
- In pseudophakic eyes
- In selected refractory glaucoma
- In certain childhood glaucomas
- When a controlled internal treatment is preferred
Because it requires an incision, ECP is a surgical laser procedure rather than a non-incisional office laser.
Who May Need Cyclophotocoagulation?
CPC may be considered when:
- Pressure remains uncontrolled despite several drops
- SLT is unsuitable or insufficient
- Previous trabeculectomy or tube surgery failed
- Incisional surgery carries high risk
- Neovascular glaucoma is present
- The eye is painful from very high pressure
- Visual potential is poor
- A less invasive pressure-lowering procedure is preferred
- Previous procedures have produced extensive conjunctival scarring
Micropulse or carefully controlled CPC may also be considered earlier in selected eyes with useful vision.
What Are the Risks of Cyclophotocoagulation?
Potential complications include:
- Pain
- Inflammation
- Temporary or sustained pressure elevation
- Excessively low pressure
- Choroidal detachment
- Macular oedema
- Bleeding
- Reduced vision
- Corneal swelling
- Cataract progression
- Irregular pupil
- Need for repeat treatment
More serious risks include:
- Persistent hypotony
- Shrinkage of the eye
- Severe inflammation
- Permanent loss of vision
- Rare sympathetic ophthalmia
The risk depends on:
- Laser technique
- Energy delivered
- Number of treated areas
- Glaucoma type
- Previous surgery
- Baseline visual potential
Continuous-wave CPC generally carries more risk of destructive complications than micropulse treatment.
Can CPC Be Repeated?
Yes.
Retreatment may be required when:
- The initial response is insufficient
- Pressure later rises
- Only part of the ciliary body was initially treated
- The surgeon deliberately used conservative energy
Repeated treatment increases cumulative exposure and must be balanced against the risk of hypotony and inflammation.
Does CPC Restore Vision in a Painful Blind Eye?
No.
The purpose may be to:
- Lower pressure
- Reduce pain
- Reduce medication burden
- Improve comfort
It does not restore vision that has already been lost from advanced optic-nerve or retinal disease.
Which Laser Is Used for Which Type of Glaucoma?
Open-Angle Glaucoma or Ocular Hypertension
Common laser:
- Selective laser trabeculoplasty
Possible alternatives:
- Argon laser trabeculoplasty
- Micropulse trabeculoplasty
- Direct SLT where available
Narrow or Closed Angles
Common laser:
- Laser peripheral iridotomy
Additional option:
- Laser peripheral iridoplasty
Lens extraction may be more appropriate in selected established angle-closure disease.
Refractory or Complex Glaucoma
Possible laser:
- Continuous-wave CPC
- Slow-coagulation CPC
- Micropulse transscleral treatment
- Endoscopic CPC
How Does Laser Compare with Glaucoma Eye Drops?
Advantages of Laser
- No daily instillation for some patients
- Less dependence on memory
- Avoids chronic preservative exposure
- Fewer systemic medication effects
- Can provide several years of control
- May reduce the number of bottles
- SLT is repeatable in selected eyes
Limitations of Laser
- Not every eye responds
- Effect may wear off
- Temporary pressure spikes can occur
- Drops may still be required
- Different procedures have different risks
- Continued monitoring remains essential
- Laser cannot restore lost vision
Advantages of Eye Drops
- No procedure
- Treatment can begin immediately
- Several medication mechanisms are available
- Dose and class can be adjusted
- Useful across many glaucoma types
Limitations of Eye Drops
- Daily lifelong routine
- Adherence difficulties
- Ocular-surface irritation
- Systemic side effects
- Ongoing cost
- Multiple bottles may be required
For suitable open-angle glaucoma or ocular hypertension, SLT and drops are both valid initial options. The choice should reflect clinical suitability and patient preference.
How Does Laser Compare with Glaucoma Surgery?
Laser is generally less invasive than:
- Trabeculectomy
- Glaucoma drainage implantation
- Minimally invasive glaucoma surgery
Recovery is often faster and serious complications are less common.
However, incisional surgery may achieve substantially lower pressure and may be necessary when:
- Glaucoma is advanced
- The target pressure is very low
- Laser and drops are insufficient
- Pressure is dangerously high
- Progression continues rapidly
The National Eye Institute notes that incisional surgery may be recommended when medicines and laser do not provide adequate control.
Can Laser Replace Surgery in Advanced Glaucoma?
Sometimes, but not always.
SLT may help an advanced-glaucoma eye when:
- The angle is open
- Pressure is moderately above target
- A modest additional reduction may be enough
- Surgery carries significant risk
It may be inadequate when:
- Very low pressure is required
- The field is rapidly deteriorating
- The angle is closed
- The outflow system is severely damaged
- The nerve cannot tolerate further delay
CPC may lower pressure in refractory advanced disease but carries a different risk profile.
What Happens Before Glaucoma Laser Treatment?
The pre-laser assessment may include:
- Visual acuity
- Eye-pressure measurement
- Slit-lamp examination
- Gonioscopy
- Optic-nerve assessment
- Review of OCT and visual fields
- Medication and allergy review
- Examination of the cornea and anterior chamber
- Discussion of risks, benefits and alternatives
Patients should disclose:
- Pregnancy
- Blood-thinning medication
- Asthma or cardiac disease
- Previous steroid response
- Eye inflammation
- Herpes eye disease
- Previous eye surgery
- Current glaucoma drops
Blood-thinning medication does not always need to be stopped for office laser, but the prescribing doctor’s advice should be followed.
Should I Use My Glaucoma Drops Before Laser?
Usually, yes.
Continue the usual treatment unless instructed otherwise.
Stopping medication beforehand may allow pressure to rise unnecessarily.
Bring the medication list or bottles to the appointment.
Can Both Eyes Be Treated on the Same Day?
Sometimes.
This depends on:
- Type of laser
- Disease severity
- Patient preference
- Clinic protocol
- Risk of inflammation or pressure spikes
- Ability to attend follow-up
Bilateral SLT or iridotomy can be performed in selected patients.
Others prefer separate sessions.
Can I Drive Home?
Vision may be temporarily blurred because of:
- The contact lens
- Gel used during treatment
- Pupil-altering drops
- Bright laser light
- Mild inflammation
It is safer to arrange transport, particularly when:
- Both eyes are treated
- Vision is already limited
- Pilocarpine is used
- The patient is light-sensitive
- The clinic advises against driving
What Is Recovery Like After SLT or Iridotomy?
Most patients can resume light activity quickly.
Temporary symptoms may include:
- Mild blur
- Grittiness
- Redness
- Light sensitivity
- Brow ache
- Headache
Follow the prescribed instructions regarding:
- Anti-inflammatory drops
- Glaucoma drops
- Driving
- Exercise
- Swimming
- Contact lenses
- Follow-up timing
Avoid rubbing the eye while numbing drops remain active.
Can I Exercise After Laser?
Light ordinary activity is usually possible.
The doctor may advise avoiding:
- Heavy straining
- Vigorous exercise
- Swimming
- Dusty environments
for a short period, especially after more inflammatory treatments.
Restrictions after CPC may be more extensive than after SLT or LPI.
When Is the Pressure Rechecked?
Depending on the procedure and risk, pressure may be checked:
- Shortly after laser
- The next day
- Within one week
- Several weeks later
Earlier review is particularly important for:
- Advanced glaucoma
- High pretreatment pressure
- Heavily pigmented angles
- Previous pressure spikes
- Acute angle closure
- Significant post-laser symptoms
Warning Symptoms After Glaucoma Laser
Seek prompt eye care for:
- Severe or increasing eye pain
- Sudden loss of vision
- Marked redness
- Persistent nausea or vomiting
- New halos with pain
- A cloudy cornea
- Significant light sensitivity
- Thick discharge
- Trauma to the treated eye
- Symptoms that worsen rather than improve
Mild irritation is common, but severe pain or visual loss is not expected after routine SLT or iridotomy.
Can Laser Treatment Make Glaucoma Worse?
A temporary pressure spike can place additional stress on the optic nerve.
This is why:
- Preventive pressure-lowering drops may be given.
- Pressure may be checked after treatment.
- High-risk patients receive closer observation.
Long-term failure of the laser does not usually mean the glaucoma was caused to worsen; it may mean the effect was insufficient or wore off while the disease continued.
CPC can cause excessive pressure lowering or inflammation and therefore has a different risk profile.
Can Laser Damage the Retina?
SLT and LPI target the front of the eye rather than the retina.
Retinal complications are rare.
Recognised but uncommon complications of iridotomy include retinal or macular effects.
Cyclophotocoagulation may cause macular oedema or other posterior-segment complications through inflammation or hypotony.
Can Laser Cause Cataract?
Routine SLT is not considered a major cause of cataract.
LPI may rarely be associated with local lens injury or cataract progression, especially if laser energy is delivered too close to the lens.
CPC can contribute to cataract development through inflammation in susceptible phakic eyes.
Age-related cataract and glaucoma frequently coexist, making causation difficult to determine in an individual patient.
Can Laser Be Performed After Cataract Surgery?
Yes.
SLT can be performed in pseudophakic eyes when the angle is open.
Iridotomy may be performed for selected pupillary-block mechanisms, although routine primary angle closure is often improved by lens removal.
CPC and ECP may also be performed in pseudophakic eyes.
Can Laser Be Performed After LASIK?
Yes.
Previous corneal refractive surgery does not usually prevent glaucoma laser treatment.
However:
- Eye-pressure measurements may be underestimated after LASIK or PRK.
- High myopia may complicate optic-nerve assessment.
- The original glaucoma risk remains.
Can Children Receive Glaucoma Laser?
Yes, in selected circumstances.
Possible procedures include:
- SLT for juvenile open-angle glaucoma
- Iridotomy for pupillary block
- Iridoplasty for selected angle mechanisms
- ECP or transscleral CPC for refractory childhood glaucoma
Children often require:
- Greater cooperation support
- Sedation or general anaesthesia
- Specialist paediatric glaucoma care
- Closer long-term monitoring
Evidence for SLT in juvenile glaucoma is less extensive than in adult disease.
Frequently Asked Questions
Is glaucoma laser surgery?
Some laser procedures are performed in the clinic without an incision.
CPC and ECP may be performed in an operating or procedure room and can be considered surgical laser treatments.
Does the laser burn the optic nerve?
No.
SLT treats the trabecular meshwork.
Iridotomy and iridoplasty treat the iris.
CPC treats the ciliary body.
Does laser restore lost peripheral vision?
No.
Existing glaucomatous visual-field loss is generally irreversible.
Is SLT a cure?
No.
Its effect may last for years, but pressure can rise again.
Can I choose SLT instead of drops?
Often, yes, when open-angle glaucoma or ocular hypertension is suitable for laser.
Does SLT work for closed-angle glaucoma?
Not usually, because the iris blocks access to the trabecular meshwork.
Why do I still need drops after SLT?
The laser may not have lowered pressure enough to reach the target.
The combined effect of laser and medication may be necessary.
Why did my pressure not change immediately?
SLT often requires several weeks to reach its full effect.
Can SLT be repeated three or four times?
It can be repeated in selected eyes, but the likelihood and size of response may decline.
Can iridotomy prevent an acute glaucoma attack?
It can substantially reduce pupillary-block-related risk in appropriately selected eyes.
Does an iridotomy hole affect the appearance of the eye?
It is usually very small and placed peripherally, often beneath the upper eyelid.
It is generally not noticeable without magnification.
Can the iridotomy hole close?
Yes.
A repeat laser may be needed.
Why is my angle still narrow after iridotomy?
The lens, plateau iris, peripheral iris thickness or synechiae may continue crowding the angle.
Is iridoplasty the same as iridotomy?
No.
Iridoplasty contracts peripheral iris tissue; iridotomy creates an opening through the iris.
Is micropulse CPC completely risk-free?
No.
It may carry fewer severe complications than conventional continuous-wave treatment, but inflammation, pain, pressure problems and visual loss remain possible.
Does CPC destroy the whole ciliary body?
No.
Only selected regions receive treatment, and energy is adjusted to reduce aqueous production without eliminating all ciliary-body function.
Can laser cause pressure to become too low?
This is unusual after SLT or iridotomy.
It is a more important potential complication after cyclophotocoagulation.
Will I feel the laser working?
No.
Pressure lowering cannot normally be felt.
Can I stop follow-up when the laser works?
No.
The effect can diminish and glaucoma can progress despite an apparently acceptable pressure.
How often should I be reviewed after laser?
The schedule depends on:
- Procedure
- Pressure response
- Disease severity
- Glaucoma type
- Symptoms
- Medication changes
Can laser be performed while I am on blood thinners?
Often, yes, particularly for office-based SLT or LPI.
The ophthalmologist should know what medication is being taken. Do not stop anticoagulants or antiplatelet drugs without instruction from the prescribing doctor.
Is laser suitable during pregnancy?
Selected laser treatments may reduce the need for medications with systemic absorption.
The decision depends on glaucoma type, disease severity and stage of pregnancy.
Does laser treatment hurt more in a heavily pigmented iris?
A thicker or more pigmented iris may require more energy during iridotomy, but topical anaesthesia and staged argon-YAG treatment can improve control.
Why was argon laser used before YAG during iridotomy?
Argon laser can thin and coagulate the iris, potentially reducing bleeding before the YAG laser creates the opening.
Can I wear contact lenses after laser?
Follow the clinic’s instructions.
It may be advisable to avoid contact lenses until:
- Surface irritation settles
- Prescribed drops are completed
- The eye is white and comfortable
Is laser covered by insurance or MediSave?
Coverage depends on:
- Procedure code
- Clinical indication
- Facility
- Insurance policy
- Panel arrangements
- Current MediSave and MediShield rules
Singapore’s Ministry of Health lists selective laser trabeculoplasty as a recognised ophthalmic procedure with published bill information.
Patients should obtain a clinic estimate and confirm coverage with the insurer before treatment.
A Practical Comparison of Glaucoma Lasers
| Procedure | Main target | Common use | Main limitation |
|---|---|---|---|
| SLT | Trabecular meshwork | Open-angle glaucoma and ocular hypertension | Some eyes do not respond; effect may wear off |
| ALT | Trabecular meshwork | Older open-angle treatment | More thermal damage and limited repeatability |
| LPI | Peripheral iris | Pupillary block and angle closure | Angle may remain narrow; pressure may remain elevated |
| Iridoplasty | Peripheral iris surface | Plateau iris or persistent appositional closure | Long-term pressure benefit is less certain |
| Micropulse CPC | Ciliary body through sclera | Refractory or selected uncontrolled glaucoma | May require repeat treatment |
| Continuous-wave CPC | Ciliary body through sclera | Refractory or painful high-pressure glaucoma | Greater inflammation and hypotony risk |
| ECP | Ciliary processes from inside the eye | Often combined with cataract surgery | Requires an intraocular surgical procedure |
A Practical Laser Treatment Pathway
Step 1: Identify the Glaucoma Mechanism
- Open angle
- Narrow or closed angle
- Pupillary block
- Plateau iris
- Refractory aqueous production
- Secondary glaucoma
Step 2: Determine the Target Pressure
Consider:
- Baseline pressure
- Optic-nerve damage
- OCT
- Visual field
- Age and progression
Step 3: Choose the Appropriate Laser
- Open angle: consider SLT
- Pupillary block: consider LPI
- Persistent appositional closure: consider iridoplasty
- Refractory glaucoma: consider CPC or ECP
Step 4: Discuss Alternatives
Alternatives may include:
- Eye drops
- Cataract or lens surgery
- MIGS
- Trabeculectomy
- Glaucoma drainage implant
- Observation in selected low-risk cases
Step 5: Perform and Monitor
- Use preventive pressure-lowering treatment when indicated.
- Check pressure after laser.
- Treat inflammation.
- Continue medication unless instructed otherwise.
Step 6: Assess the Response
- Was the target pressure reached?
- Can drops be reduced?
- Did the angle open?
- Is retreatment required?
- Is surgery now more appropriate?
Step 7: Continue Glaucoma Surveillance
- Eye pressure
- Gonioscopy
- Optic-nerve examination
- OCT
- Visual-field testing
Common Myths About Laser Glaucoma Treatment
“Laser cures glaucoma.”
False.
It lowers pressure or treats an anatomical mechanism but does not remove the underlying lifelong risk.
“Laser restores the damaged optic nerve.”
False.
Existing nerve loss is generally permanent.
“SLT means I will never need drops.”
False.
Some patients remain drop-free, while others need medication immediately or later.
“All glaucoma lasers are the same.”
False.
SLT, iridotomy, iridoplasty and CPC treat different structures and diseases.
“Laser is only used after every eye drop fails.”
False.
SLT is now an established first-line option for many patients with open-angle glaucoma or ocular hypertension.
“A normal pressure after laser means follow-up is unnecessary.”
False.
Pressure can rise again and progression may occur despite a normal clinic reading.
“Every narrow angle needs iridotomy.”
False.
Low-risk angle-closure suspects may be observed, while higher-risk eyes benefit more clearly from treatment.
“Iridotomy fully cures angle closure.”
False.
Lens crowding, plateau iris and permanent angle adhesions may remain.
“Micropulse CPC has no risks.”
False.
Its safety profile may be better than conventional CPC, but significant complications remain possible.
The Bottom Line
Laser glaucoma treatment is not one single procedure.
The principal options are:
- Selective laser trabeculoplasty: improves drainage in open-angle glaucoma and ocular hypertension.
- Laser peripheral iridotomy: creates an opening in the iris to relieve pupillary block.
- Laser peripheral iridoplasty: contracts the peripheral iris to widen a persistently crowded angle.
- Cyclophotocoagulation: reduces aqueous-fluid production in refractory or selected uncontrolled glaucoma.
SLT may be offered as a first treatment rather than eye drops in many suitable open-angle eyes.
Laser iridotomy is used for selected narrow-angle and angle-closure conditions, but it does not guarantee that the angle will open completely or that pressure medication will be unnecessary.
Cyclophotocoagulation is a more powerful treatment with a different risk profile. Micropulse techniques may reduce inflammation and hypotony risk, but retreatment may be needed.
All glaucoma lasers share several limitations:
- They do not restore lost vision.
- They do not guarantee lifelong pressure control.
- They do not eliminate the need for OCT, visual fields and pressure checks.
- Further drops, repeat laser or surgery may still be required.
The right question is not simply, “Should I have glaucoma laser?” It is, “Which structure is causing my pressure problem, which laser treats that mechanism, and will the expected pressure reduction be enough to protect my optic nerve?”
References
- National Eye Institute. Laser Treatment for Glaucoma. Updated August 2025.
- National Eye Institute. Glaucoma Surgery. Updated December 2024.
- National Institute for Health and Care Excellence. Glaucoma: Diagnosis and Management. Reviewed March 2025.
- Gazzard G, et al. Laser in Glaucoma and Ocular Hypertension Trial: Six-Year Results of Primary SLT Versus Eye Drops. Ophthalmology. 2023.
- Montesano G, et al. Six-Year Rate of Visual-Field Progression in the LiGHT Trial. Ophthalmology. 2026.
- Chavez MP, et al. Selective Laser Trabeculoplasty Versus Medical Therapy for Open-Angle Glaucoma. 2024.
- Polat J, et al. Repeatability of Selective Laser Trabeculoplasty. British Journal of Ophthalmology. 2016.
- Radhakrishnan S, et al. Laser Peripheral Iridotomy in Primary Angle Closure: An American Academy of Ophthalmology Report. Ophthalmology. 2018.
- He M, et al. Laser Peripheral Iridotomy for the Prevention of Angle Closure: The ZAP Trial. The Lancet. 2019.
- Yuan Y, et al. Fourteen-Year Outcome of Angle-Closure Prevention With Laser Iridotomy. Ophthalmology. 2023.
- Azuara-Blanco A, et al. Effectiveness of Early Lens Extraction for Primary Angle Closure and Glaucoma: The EAGLE Trial. The Lancet. 2016.
- Bayliss JM, et al. Laser Peripheral Iridoplasty for Chronic Angle Closure. Cochrane Database of Systematic Reviews. 2021.
- Aquino MCD, et al. Micropulse Versus Continuous-Wave Transscleral Cyclophotocoagulation in Refractory Glaucoma. Clinical and Experimental Ophthalmology. 2015.
- Chavez MP, et al. Micropulse Transscleral Laser Treatment Versus Continuous-Wave Cyclophotocoagulation. 2025.
- Singapore HealthHub. Glaucoma.