Author: Dr Val Phua
Estimated reading time: 14–16 minutes
What Are Dry Eyes?
Dry eye disease occurs when the tears do not adequately protect, lubricate or support the surface of the eye.
This may happen because:
- The eyes do not produce enough tears
- The tears evaporate too quickly
- The oil, water or mucous components of the tears are abnormal
- The eyelids do not spread tears properly
- Inflammation damages the tear-producing system or ocular surface
- The nerves controlling tear production and sensation do not function normally
The 2025 Tear Film and Ocular Surface Society Dry Eye Workshop defined dry eye as a multifactorial symptomatic disease involving loss of tear-film or ocular-surface stability. Tear instability, excessive tear concentration, inflammation, surface damage and abnormal nerve sensation may all contribute.
Dry eye is therefore more than simply “not having enough water in the eyes.”
A patient may have dry eye because the tears are:
- Too few
- Too unstable
- Missing sufficient protective oil
- Poorly distributed
- Excessively salty or concentrated
- Associated with ocular-surface inflammation
Most patients have more than one contributing factor.
What Is the Tear Film?
Every blink spreads a thin layer of tears across the cornea and conjunctiva.
This tear film is essential for:
- Clear and stable vision
- Lubricating the eyelids
- Protecting the cornea
- Delivering oxygen and nutrients
- Washing away debris
- Defending against infection
- Allowing the eyelids to move comfortably
The tear film is traditionally described as having oil, water and mucous components, although these layers blend together rather than existing as three completely separate sheets.
The Oil Component
The outer oil component is produced mainly by the meibomian glands within the eyelids.
It helps:
- Slow tear evaporation
- Stabilise the tear film
- Prevent tears from overflowing too easily
- Maintain a smooth optical surface
Blocked or unhealthy meibomian glands are a major cause of evaporative dry eye.
The Watery Component
The watery component is produced mainly by the lacrimal glands.
It contains:
- Water
- Electrolytes
- Proteins
- Antibodies
- Growth factors
- Antimicrobial substances
Reduced aqueous production may occur with ageing, autoimmune disease, medication use or damage to the lacrimal glands.
The Mucous Component
Mucins are produced by conjunctival goblet cells and ocular-surface tissues.
They help the tears spread evenly and adhere to the cornea.
Mucin abnormalities may occur with:
- Chronic inflammation
- Vitamin A deficiency
- Chemical injury
- Cicatrising conjunctival disease
- Certain medications
What Are the Main Types of Dry Eye?
Dry eye is commonly divided into:
- Evaporative dry eye
- Aqueous-deficient dry eye
- Mixed dry eye
Many patients have a combination.
Evaporative Dry Eye
In evaporative dry eye, tears are produced but disappear too quickly.
The most common cause is meibomian gland dysfunction.
Other contributors include:
- Incomplete blinking
- Prolonged screen use
- Eyelid disease
- Contact-lens wear
- Air conditioning
- Wind
- Low humidity
- Eyelid exposure
- Reduced blink strength
The tears may break apart only a few seconds after blinking, producing fluctuating blur and irritation.
Aqueous-Deficient Dry Eye
In aqueous-deficient dry eye, the lacrimal glands do not produce enough watery tears.
Possible causes include:
- Ageing
- Sjögren disease
- Rheumatoid arthritis
- Lupus
- Lacrimal-gland inflammation
- Previous radiation treatment
- Certain medications
- Nerve damage
- Severe ocular-surface disease
Patients may also have dry mouth, difficulty swallowing dry food, joint symptoms or systemic fatigue when an autoimmune disease is involved.
Mixed Dry Eye
Many patients have both:
- Reduced tear production
- Excessive evaporation
For example, an older patient may have reduced lacrimal secretion, blocked meibomian glands, incomplete blinking and chronic preserved eye-drop exposure simultaneously.
Successful treatment usually requires addressing each important contributor.
What Are the Symptoms of Dry Eye?
Dry eye symptoms may include:
- Burning
- Stinging
- Grittiness
- A sandy sensation
- Foreign-body sensation
- Tired or heavy eyes
- Redness
- Itching
- Light sensitivity
- Intermittent blurred vision
- Difficulty keeping the eyes open
- Discomfort when reading
- Contact-lens intolerance
- Excessive tearing
- Eye fatigue during screen use
Singapore HealthHub lists dryness, burning, foreign-body sensation, tired eyes, blurred vision, excessive tearing and light sensitivity among common symptoms.
Why Can Dry Eyes Cause Blurred Vision?
The tear film is the eye’s first optical surface.
A smooth, stable tear layer helps light focus sharply through the cornea.
When the tear film breaks apart:
- The corneal surface becomes optically irregular
- Vision fluctuates
- Letters may appear smeared
- Glare may increase
- Fine details become temporarily less clear
Dry-eye blur often:
- Changes from moment to moment
- Worsens during prolonged visual concentration
- Temporarily improves after blinking
- Improves after lubricant drops
- Is worse in air conditioning or wind
Persistent blur that does not improve with blinking may indicate another condition such as refractive error, cataract, corneal disease, macular disease or optic-nerve disease.
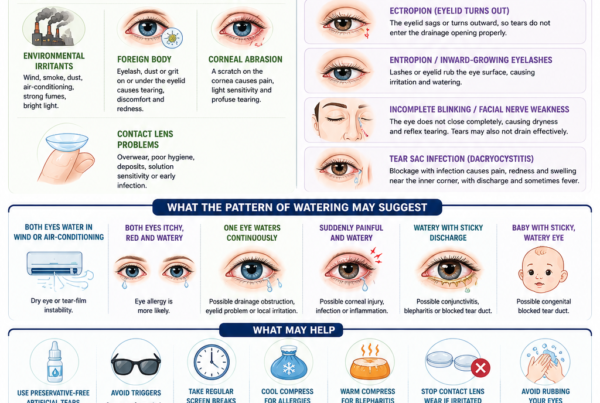
Why Do Dry Eyes Sometimes Water Excessively?
Excessive watering can be a symptom of dry eye.
When the surface becomes irritated, sensory nerves trigger reflex tearing.
These reflex tears may be:
- Very watery
- Poorly balanced
- Short-lived
- Unable to remain on the eye
The tears may then overflow down the cheek without adequately lubricating the cornea.
Watering may also be caused by:
- Blocked tear drainage
- Eyelid malposition
- Allergy
- Infection
- A foreign body
- Corneal abrasion
An examination may be needed when watering is persistent or mainly affects one eye.
Can Dry Eye Cause Eye Pain?
Yes.
Dry eye discomfort may range from mild irritation to significant burning or aching.
Some patients experience symptoms that appear much more severe than the visible surface findings.
This may occur because ocular-surface nerves have become:
- Hypersensitive
- Inflamed
- Injured
- Abnormally active
Neuropathic ocular pain may cause:
- Burning
- Severe light sensitivity
- Wind sensitivity
- Pain triggered by air conditioning
- Persistent pain despite frequent lubrication
- Discomfort out of proportion to surface staining
These patients may require evaluation beyond simply increasing artificial tears.
Why Do Dry-Eye Symptoms and Test Results Sometimes Disagree?
Dry eye is not measured by one perfect test.
A patient may have:
- Significant symptoms but minimal visible staining
- Marked corneal staining but relatively few symptoms
- Reduced corneal sensation
- Neuropathic pain
- Fluctuating findings
- Different symptoms in different environments
Reduced sensation can occur in:
- Diabetes
- Long-term contact-lens wear
- Previous herpes infection
- Corneal surgery
- Neurotrophic keratopathy
A severely damaged but poorly sensitive cornea may produce surprisingly little discomfort.
What Causes Dry Eye?
Meibomian Gland Dysfunction
Meibomian glands are vertically arranged oil glands within the upper and lower eyelids.
They release oil through small openings along the eyelid margin.
In meibomian gland dysfunction, the oil may become:
- Too thick
- Cloudy
- Reduced in volume
- Unable to leave the gland
- Chemically abnormal
The gland openings may become blocked, and the glands may gradually shorten or disappear.
Without a healthy oil layer, tears evaporate too quickly.
Meibomian gland dysfunction is considered a leading cause of evaporative dry eye.
Blepharitis
Blepharitis is inflammation of the eyelid margins.
It may cause:
- Crusting around the eyelashes
- Eyelid redness
- Burning
- Itching
- Unstable tears
- Recurrent styes
- Blocked meibomian glands
Blepharitis and dry eye commonly occur together.
Treating only the tear deficiency without addressing the eyelid disease may provide incomplete relief.
Ageing
Tear production and meibomian gland function may decline with age.
Older adults are also more likely to:
- Use medications that reduce tear production
- Have eyelid laxity
- Undergo eye surgery
- Develop diabetes or autoimmune disease
- Use several preserved eye drops
Dry eye is therefore increasingly common after age 50.
Hormonal Factors
Dry eye is more common in women, particularly after menopause.
Sex hormones can influence:
- Lacrimal glands
- Meibomian glands
- Goblet cells
- Ocular-surface inflammation
- Corneal nerves
Hormone replacement does not reliably treat dry eye and may affect patients differently.
Screen Use
People blink less frequently and less completely while concentrating on:
- Computers
- Tablets
- Smartphones
- Video games
- Reading material
An incomplete blink may fail to spread meibomian oil across the tear film.
Prolonged screen use can therefore worsen:
- Tear evaporation
- Fluctuating blur
- Burning
- Eye fatigue
Screen use usually aggravates dry eye rather than permanently damaging an otherwise healthy retina. NEI and Singapore sources recognise prolonged screen use as a common contributor.
Air Conditioning and Fans
Direct airflow accelerates tear evaporation.
Symptoms may worsen:
- In strongly air-conditioned offices
- Under ceiling fans
- In vehicles
- On aeroplanes
- When a desk fan blows towards the face
- During cycling or motorcycling
Singapore’s warm climate does not prevent dry eye because many patients spend much of the day in cooled indoor environments.
Wind, Smoke and Pollution
The ocular surface may be irritated by:
- Wind
- Cigarette smoke
- Haze
- Dust
- Chemical fumes
- Aerosols
- Strong fragrances
Wraparound spectacles may help during windy outdoor activity.
Smoking and second-hand smoke may worsen symptoms and ocular-surface inflammation.
Contact-Lens Wear
Contact lenses interact continuously with the tear film.
They may cause or worsen dry eye through:
- Increased evaporation
- Tear-film disruption
- Surface deposits
- Reduced comfort during long wear
- Inflammation
- Corneal nerve changes
- Poor lens fit
- Inadequate cleaning
Contact-lens users should remove the lenses and seek urgent assessment when dryness is accompanied by:
- Significant pain
- Marked redness
- Light sensitivity
- Discharge
- Persistent blur
- A white corneal spot
These may indicate infection rather than ordinary dry eye.
Eye Surgery
Dry eye may worsen temporarily or persistently after:
- LASIK
- PRK
- SMILE
- Cataract surgery
- Glaucoma surgery
- Eyelid surgery
- Retinal surgery
Possible reasons include:
- Corneal nerve disruption
- Reduced blinking
- Ocular-surface medication
- Preservative exposure
- Eyelid speculum use
- Inflammation
- Pre-existing meibomian gland dysfunction
Singapore HealthHub includes LASIK and cataract surgery among factors that may worsen dryness.
Preoperative dry-eye assessment is important because an unstable tear film can affect:
- Corneal measurements
- Intraocular lens calculations
- Refractive outcomes
- Postoperative visual quality
- Patient satisfaction
Eyelid Problems
The eyelids must close completely and distribute tears evenly.
Dryness may occur with:
- Incomplete closure
- Facial nerve palsy
- Thyroid eye disease
- Eyelid retraction
- Ectropion
- Entropion
- Loose eyelids
- Scarring
- Poor blinking
- Sleeping with the eyes partially open
Exposure-related dryness commonly affects the lower or central cornea.
It may be worse on waking.
Autoimmune Disease
Autoimmune conditions can reduce tear production or inflame the ocular surface.
Examples include:
- Sjögren disease
- Rheumatoid arthritis
- Lupus
- Thyroid-related autoimmune disease
- Graft-versus-host disease
- Cicatrising conjunctival disorders
Sjögren disease should be considered when dry eye is accompanied by:
- Dry mouth
- Dental decay
- Difficulty swallowing dry food
- Joint pain
- Unexplained fatigue
- Salivary-gland swelling
Inflammation of tear-secreting glands reduces aqueous production in Sjögren disease.
Diabetes
Diabetes may contribute through:
- Reduced corneal sensation
- Abnormal tear secretion
- Meibomian gland dysfunction
- Delayed epithelial healing
- Autonomic nerve dysfunction
- Medication and systemic factors
A diabetic patient may have significant ocular-surface damage without severe symptoms because corneal sensation is reduced.
Thyroid Disease
Thyroid disease may contribute through:
- Reduced blinking
- Eyelid retraction
- Incomplete closure
- Protrusion of the eyes
- Autoimmune inflammation
- Meibomian gland dysfunction
Exposure becomes particularly important in thyroid eye disease.
Vitamin A Deficiency
Vitamin A is important for epithelial and goblet-cell health.
Severe deficiency may cause:
- Dryness
- Loss of conjunctival goblet cells
- Night blindness
- Corneal damage
- Sight-threatening surface disease
Deficiency is uncommon in well-nourished populations but may occur with:
- Malabsorption
- Bariatric surgery
- Liver disease
- Severe dietary restriction
- Certain intestinal conditions
Patients should not take high-dose vitamin A without medical advice because excessive intake can be toxic.
Medications That May Worsen Dry Eye
Possible contributors include:
- Antihistamines
- Decongestants
- Antidepressants
- Antianxiety medication
- Anticholinergic medication
- Diuretics
- Some blood-pressure medications
- Isotretinoin
- Hormonal therapies
- Sedatives
- Parkinson disease medication
- Long-term preserved glaucoma drops
Antihistamines are specifically recognised by Singapore HealthHub and NUHS as medications that may reduce tear production.
Do not stop an important systemic medication independently.
The prescribing doctor may consider:
- An alternative medication
- A lower dose
- Different timing
- Additional dry-eye treatment
Can Glaucoma Eye Drops Cause Dry Eye?
Yes.
Long-term glaucoma treatment may cause ocular-surface symptoms because of:
- Preservatives
- The active medication
- Multiple daily doses
- Chronic allergy
- Reduced tear stability
- Eyelid inflammation
Options may include:
- Preservative-free glaucoma drops
- Fixed-combination medication
- Selective laser trabeculoplasty
- Dry-eye treatment
- Glaucoma surgery in selected cases
Glaucoma drops should not be stopped without an alternative pressure-control plan.
Is Dry Eye the Same as Eye Allergy?
No, although both may coexist.
Dry Eye More Commonly Causes
- Burning
- Grittiness
- Fluctuating blur
- Tired eyes
- Symptoms during screen use
- Discomfort in air conditioning
Allergy More Commonly Causes
- Prominent itching
- Eyelid swelling
- Stringy mucus
- Seasonal symptoms
- Exposure-related attacks
- Sneezing or nasal allergy
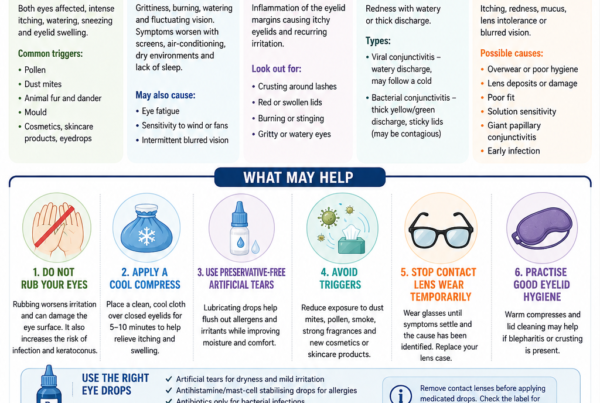
Rubbing may worsen both conditions.
Some oral antihistamines used for allergy can reduce tear production, while appropriate anti-allergy eye drops may improve the ocular-surface inflammation.
Is Dry Eye the Same as Conjunctivitis?
No.
Dry eye can cause mild redness, but infectious conjunctivitis is more likely to cause:
- Discharge
- Crusting
- Close-contact spread
- Marked conjunctival inflammation
- Recent respiratory illness
Pain, light sensitivity or reduced vision is unusual for simple conjunctivitis and should prompt assessment for a corneal or intraocular condition.
Is Dry Eye the Same as Eye Strain?
Eye strain may involve:
- Headache
- Focusing fatigue
- Difficulty reading
- Neck or shoulder discomfort
- Tired eyes
Dry eye frequently contributes, particularly during screen use.
However, eye strain may also result from:
- An incorrect spectacle prescription
- Presbyopia
- Binocular-vision problems
- Poor ergonomics
- Inadequate sleep
Can Severe Dry Eye Damage Vision?
Yes.
Most dry eye causes discomfort and fluctuating blur without permanent damage.
Severe untreated disease may cause:
- Persistent epithelial defects
- Corneal ulceration
- Infection
- Corneal thinning
- Scarring
- Blood-vessel growth
- Rare perforation
NEI notes that severe untreated dry eye can damage the cornea.
Warning Signs That May Not Be Simple Dry Eye
Seek prompt eye assessment for:
- Significant eye pain
- Marked light sensitivity
- Sudden or persistent reduced vision
- A white or grey corneal spot
- Thick discharge or pus
- Severe redness
- Eye injury
- Chemical exposure
- Contact-lens-related pain or redness
- Inability to keep the eye open
- Symptoms mainly in one eye
- A persistent foreign-body sensation
- Symptoms after eye surgery
- Facial rash or blisters around the eye
HealthHub recommends medical assessment when symptoms worsen or are associated with pain, swelling, discharge, vision changes, persistent redness, dry mouth or one-eye involvement.
How Is Dry Eye Diagnosed?
There is no single test that proves or excludes every form of dry eye.
The 2025 TFOS DEWS III diagnostic approach combines symptoms with evidence of tear-film or ocular-surface instability and then assesses the underlying contributors.
Symptom History
The clinician may ask about:
- Burning
- Grittiness
- Watering
- Fluctuating blur
- Screen exposure
- Contact-lens wear
- Environment
- Medication
- Previous surgery
- Dry mouth
- Autoimmune symptoms
- Morning or nighttime worsening
Questionnaires such as the Ocular Surface Disease Index may help quantify symptom burden, although a score does not identify the cause by itself.
Visual Acuity and Refraction
Vision is assessed before and sometimes after blinking or lubrication.
Fluctuating acuity may suggest tear-film instability.
Persistent reduction requires evaluation for other ocular disease.
Slit-Lamp Examination
The slit lamp allows assessment of:
- Tear meniscus
- Eyelid margins
- Meibomian gland openings
- Blink closure
- Conjunctiva
- Cornea
- Inflammation
- Mucus and debris
Tear Break-Up Time
A small amount of fluorescein dye may be placed in the tears.
The clinician measures how long the tear film remains intact after a blink.
Rapid breakup suggests tear instability.
The TFOS DEWS III diagnostic report includes shortened fluorescein tear breakup time as evidence of an unstable tear film.
Corneal and Conjunctival Staining
Fluorescein, lissamine green or rose bengal dye may reveal damaged or poorly protected surface cells.
The clinician assesses:
- Location
- Density
- Pattern
- Severity
Different patterns may suggest:
- Exposure
- Aqueous deficiency
- Contact-lens trauma
- Medication toxicity
- Eyelid-related friction
- Neurotrophic disease
Schirmer Test
A small paper strip is placed at the lower eyelid to measure tear production.
It may be performed:
- With anaesthetic
- Without anaesthetic
- For a specified number of minutes
Low wetting supports reduced aqueous production but should be interpreted with symptoms and other tests.
Tear Osmolarity
Tear osmolarity estimates the concentration of dissolved particles in the tears.
Abnormally concentrated or highly variable tears may support dry-eye disease.
Results may fluctuate and should not be interpreted alone.
Meibomian Gland Assessment
The clinician may inspect:
- Gland openings
- Eyelid-margin irregularity
- Oil quality
- Ease of expression
- Gland obstruction
- Telangiectatic vessels
Gentle pressure may be used to assess whether the secretions are:
- Clear
- Cloudy
- Thick
- Toothpaste-like
- Absent
Meibography
Meibography uses infrared imaging to show the structure of the meibomian glands.
It may reveal:
- Gland shortening
- Distortion
- Dropout
- Atrophy
Gland dropout cannot simply be reversed by applying more heat.
Earlier treatment aims to improve the function of the glands that remain.
Corneal Sensation
Corneal sensation may be assessed when symptoms or surface findings are unusual.
Reduced sensation may suggest:
- Diabetes
- Previous herpes infection
- Neurotrophic keratitis
- Previous corneal surgery
- Chronic contact-lens effects
- Neurological disease
Blood Tests
Blood investigations are not required for every patient.
They may be considered when symptoms suggest:
- Sjögren disease
- Rheumatoid arthritis
- Lupus
- Thyroid disease
- Vitamin deficiency
- Other systemic inflammation
A negative screening blood test does not exclude every autoimmune cause.
How Are Dry Eyes Treated?
Treatment should be matched to the underlying mechanism.
A patient with blocked oil glands may need a different approach from someone with severe Sjögren-related aqueous deficiency or exposure from facial nerve palsy.
TFOS DEWS III emphasises personalised management directed at the source of tear-film and ocular-surface instability.
Artificial Tears
Artificial tears supplement or stabilise the tear film.
Common ingredients include:
- Carboxymethylcellulose
- Hypromellose
- Hyaluronic acid
- Hydroxypropyl guar
- Carbomer
- Dextran
- Glycerin
- Lipid components
HealthHub notes that lubricant drops may substitute tears, lubricate the surface or retain moisture.
Different formulations suit different problems.
Watery Drops
Useful for:
- Mild symptoms
- Daytime use
- Frequent visual tasks
They usually blur vision only briefly.
Lipid-Containing Drops
May be more suitable when meibomian oil deficiency and rapid evaporation are important.
Gels
Remain on the eye longer but may cause temporary blur.
Ointments
Provide prolonged lubrication and are commonly used:
- At bedtime
- For exposure during sleep
- In severe aqueous deficiency
They are usually too blurry for ordinary daytime use.
Preserved Versus Preservative-Free Tears
Preservatives help prevent contamination in multidose bottles.
Frequent exposure may irritate the ocular surface in some patients.
Preservative-free tears are generally preferred when:
- Drops are needed more than four times daily
- The ocular surface is significantly inflamed
- Several preserved glaucoma drops are used
- Contact lenses are worn
- There has been corneal surgery
- Preservative sensitivity is suspected
Singapore HealthHub recommends preservative-free lubricants for people requiring drops more than four times a day.
Can Artificial Tears Be Used Too Often?
Preservative-free tears can generally be used frequently when required.
Excessive use of preserved products may worsen irritation.
A patient needing drops every few minutes should be assessed for:
- Severe aqueous deficiency
- Exposure
- Ocular-surface inflammation
- Neurotrophic disease
- Neuropathic pain
- Incorrect diagnosis
How Should Lubricant Drops Be Applied?
- Wash and dry the hands.
- Tilt the head backwards.
- Pull the lower eyelid gently down.
- Place one drop into the lower-eyelid pocket.
- Avoid touching the eye or eyelashes with the bottle.
- Close the eye gently.
- Wipe away excess fluid.
Temporary blur for a few minutes is common, particularly with thicker preparations.
Warm Compresses
Warm compresses aim to soften thickened meibomian oil.
A practical technique is:
- Use a clean warm compress or reusable eye mask.
- Ensure it is comfortably warm rather than hot.
- Apply over the closed eyelids.
- Maintain warmth for several minutes.
- Follow with gentle eyelid massage when advised.
A towel cools quickly and may need reheating.
Excessive heat can burn the eyelid skin or cornea.
Warm compresses are most useful when blocked meibomian glands are part of the problem. They are less likely to correct severe gland atrophy or pure aqueous deficiency.
Eyelid Hygiene
Eyelid hygiene may include:
- Cleaning crusts from the lash line
- Using a dedicated eyelid cleanser
- Treating dandruff or facial skin disease
- Managing Demodex mites when present
- Avoiding contaminated eye makeup
- Replacing old cosmetic products
Harsh soap or concentrated baby shampoo may irritate some ocular surfaces.
A purpose-formulated eyelid product may be better tolerated.
Blink Training
Complete blinking helps:
- Spread oil
- Reform the tear film
- Reduce evaporation
- Clear surface debris
During screen work:
- Blink deliberately
- Close the eyelids fully
- Avoid rapid partial blinking
- Take regular visual breaks
A simple routine is to perform several slow complete blinks whenever changing tasks.
Screen and Workplace Adjustments
Helpful measures may include:
- Positioning the monitor slightly below eye level
- Increasing text size
- Reducing glare
- Taking frequent short breaks
- Avoiding direct fan or air-conditioning flow
- Using a humidifier when appropriate
- Keeping adequate viewing distance
- Treating an uncorrected spectacle prescription
Lowering the monitor reduces how widely the eyelids must open and may reduce exposed ocular surface.
The 20-20-20 Rule
A commonly used approach is to look approximately 20 feet away for 20 seconds every 20 minutes.
The exact numbers are less important than:
- Breaking prolonged concentration
- Relaxing accommodation
- Blinking fully
- Looking away from the screen
A break will not treat severe dry-eye disease by itself but may reduce screen-related worsening.
Hydration and Sleep
Adequate hydration and sleep support general health and tear function.
However, simply drinking more water will not correct:
- Blocked meibomian glands
- Sjögren-related lacrimal damage
- Eyelid exposure
- Significant ocular-surface inflammation
Lifestyle measures should complement rather than replace targeted treatment.
Wraparound Glasses and Moisture Chambers
Wraparound spectacles reduce airflow across the eyes.
Moisture-chamber glasses retain humidity around the ocular surface.
They may help with:
- Wind sensitivity
- Cycling
- Air-conditioned environments
- Severe aqueous deficiency
- Exposure-related dryness
- Neuropathic wind sensitivity
NUHS includes moisture-chamber spectacles among potential measures for dry eye.
Treating Meibomian Gland Dysfunction
Management may include:
- Warm compresses
- Eyelid hygiene
- Gland expression
- Lipid-containing lubricants
- Treatment of rosacea
- Oral or topical antibiotics in selected cases
- Thermal pulsation
- Intense pulsed light
- Radiofrequency or other heat-based treatments
Not every device-based treatment is suitable for every patient, and results vary.
Meibomian Gland Expression
After warming the eyelids, controlled pressure may be applied to release obstructed oil.
It may be performed:
- Manually
- With forceps
- Using an office device
Forceful home squeezing may injure the eyelids and is not recommended.
Thermal Pulsation
Thermal pulsation devices apply controlled heat and pressure to the eyelids.
They aim to:
- Warm thickened oil
- Express blocked glands
- Improve meibomian secretion
Treatment may improve symptoms in selected patients, but it does not regenerate glands that have already atrophied.
Intense Pulsed Light
Intense pulsed light treatment applies filtered light to the skin around the eyelids.
Potential mechanisms include:
- Reducing abnormal surface vessels
- Decreasing inflammatory mediators
- Improving meibomian secretion
- Treating associated rosacea
Eye protection and correct patient selection are essential.
The treatment is not suitable for every skin type, medication profile or ocular condition.
Antibiotics for Eyelid Disease
Low-dose oral doxycycline or selected topical antibiotics may be prescribed for:
- Rosacea
- Chronic meibomian gland inflammation
- Recurrent styes
- Significant blepharitis
Their benefit may relate partly to anti-inflammatory effects rather than simply killing bacteria.
Possible oral doxycycline side effects include:
- Stomach irritation
- Sun sensitivity
- Oesophageal irritation
- Drug interactions
It is unsuitable in selected patients, including during pregnancy.
Prescription Anti-Inflammatory Drops
Chronic dry eye frequently involves inflammation.
Prescription options may include:
- Cyclosporine
- Lifitegrast
- Short courses of topical corticosteroids
- Other locally available immunomodulatory treatments
NEI identifies cyclosporine and lifitegrast as prescription treatments for more significant dry eye.
Availability and regulatory approval differ between countries.
Cyclosporine
Cyclosporine reduces ocular-surface inflammation and may improve natural tear production over time.
Patients should understand that:
- Improvement may take weeks or months
- Initial burning or stinging is common
- Lubricants may still be required
- Consistent use matters
- It is not an immediate numbing drop
Lifitegrast
Lifitegrast targets an inflammatory pathway involved in dry eye.
Possible effects include:
- Temporary irritation
- Blurred vision
- An unusual taste
Availability varies by country.
Topical Steroids
A short supervised course may rapidly reduce significant inflammation.
Potential risks include:
- Increased eye pressure
- Glaucoma
- Cataract
- Delayed healing
- Worsening of certain infections
Steroid drops should not be started or continued without medical supervision.
NUHS notes that steroid and cyclosporine treatment should be undertaken with close supervision because of potential side effects.
Punctal Plugs
Tears drain through small openings called puncta at the inner eyelids.
A punctal plug partially or completely blocks this drainage, allowing tears to remain longer on the eye.
Plugs may be:
- Temporary and dissolvable
- Longer-lasting silicone devices
They may help aqueous-deficient dry eye.
Possible limitations include:
- Watering
- Irritation
- Plug loss
- Plug migration
- Infection
- Retention of inflammatory tears
Inflammation and eyelid disease are often treated before or alongside punctal occlusion.
NEI and NUHS recognise punctal occlusion as a method of conserving tears.
Cautery of the Puncta
In severe aqueous deficiency, tear drainage openings may be closed more permanently using cautery.
This is generally considered when temporary occlusion has been helpful but insufficient or plugs repeatedly fall out.
Autologous Serum Eye Drops
Autologous serum drops are made using the patient’s own blood.
The serum contains:
- Growth factors
- Vitamins
- Proteins
- Components that resemble natural tears
They may be considered for:
- Severe dry eye
- Persistent epithelial defects
- Sjögren disease
- Neurotrophic keratopathy
- Severe postoperative surface disease
They require:
- Blood collection
- Special preparation
- Cold storage
- Careful handling
NUHS describes autologous serum as an option for severe dry eye while noting the inconvenience and infection considerations.
Platelet-Rich Plasma and Related Blood Products
Other biological preparations may include:
- Platelet-rich plasma
- Plasma rich in growth factors
- Allogeneic serum
Their availability, preparation and evidence vary between centres.
Scleral Contact Lenses
A scleral lens is a large rigid lens that vaults over the cornea and rests on the white of the eye.
The space beneath the lens is filled with sterile saline, creating a fluid reservoir over the cornea.
Scleral lenses may help:
- Severe aqueous deficiency
- Sjögren disease
- Irregular corneas
- Neurotrophic disease
- Exposure
- Graft-versus-host disease
They require specialist fitting and careful hygiene.
They are not the same as ordinary soft contact lenses.
Bandage Contact Lenses
A bandage lens may temporarily protect the cornea when there is:
- An epithelial defect
- Recurrent erosion
- Severe surface pain
- Postoperative injury
Because a lens can increase infection risk, antibiotic cover and close follow-up may be required.
Amniotic Membrane
An amniotic membrane may be placed on the eye to support healing in severe surface disease.
It may be used for:
- Persistent epithelial defects
- Neurotrophic keratitis
- Severe inflammation
- Chemical injury
- Selected postoperative complications
Eyelid Surgery
Surgery may be required when dryness is caused by:
- Ectropion
- Entropion
- Eyelid laxity
- Incomplete closure
- Facial nerve palsy
- Excessive exposure
Possible procedures include:
- Eyelid tightening
- Correcting malposition
- Tarsorrhaphy
- Upper-eyelid loading for facial palsy
NEI notes that eyelid surgery is occasionally used when abnormal eyelid position prevents tears from remaining on the eye.
What Is Tarsorrhaphy?
Tarsorrhaphy partially joins the upper and lower eyelids to reduce exposure.
It may be:
- Temporary
- Permanent
- Partial
- Adjustable
It is used for severe exposure or neurotrophic disease when the cornea needs stronger protection.
Can Omega-3 Supplements Treat Dry Eye?
Evidence is mixed.
Some smaller studies have suggested benefit, but the large multicentre DREAM trial did not find omega-3 supplements superior to an olive-oil placebo for improving dry-eye symptoms and signs over one year.
Eating fish and maintaining a balanced diet may have general health benefits, but patients should not assume that high-dose fish-oil supplements will reliably cure dry eye.
Supplements may also interact with medication or increase bleeding risk in selected patients.
Can Dry Eye Be Cured?
Some temporary forms resolve after the trigger is removed.
Examples include:
- Short-term medication-related dryness
- Postoperative dryness
- Environmental exposure
- Contact-lens overwear
Chronic dry eye caused by ageing, meibomian gland loss or autoimmune disease is usually controlled rather than permanently cured.
Treatment aims to:
- Improve comfort
- Stabilise vision
- Protect the cornea
- Reduce inflammation
- Preserve remaining gland function
- Prevent recurrence
How Long Does Treatment Take to Work?
The response depends on the treatment.
Artificial Tears
May provide relief within minutes but often have a temporary effect.
Warm Compresses
May improve symptoms over days or weeks when used consistently.
Prescription Anti-Inflammatory Drops
May require several weeks or months.
Device-Based Gland Treatment
May produce gradual improvement, and repeat treatment may be needed.
Severe Surface Disease
May require long-term combined therapy.
Failure of one lubricant brand does not mean that dry eye is untreatable.
Can Dry Eye Return After Treatment?
Yes.
Symptoms may recur because of:
- Environmental changes
- Reduced treatment adherence
- Screen exposure
- Illness
- Medication
- Hormonal changes
- Progression of meibomian gland dysfunction
- Contact-lens use
- Eye surgery
A maintenance plan is often necessary after symptoms improve.
Dry Eye and Contact Lenses
Patients with mild dry eye may continue wearing contact lenses after:
- Optimising the tear film
- Treating meibomian glands
- Adjusting lens material or replacement frequency
- Reducing wearing hours
- Improving hygiene
Stop lens wear and seek assessment for:
- Pain
- Redness
- Light sensitivity
- Discharge
- Persistent blur
- A visible corneal spot
Never use tap water to rinse or store contact lenses.
Dry Eye Before Cataract or Refractive Surgery
Dry eye should be identified and treated before measurements are finalised.
An unstable surface can affect:
- Corneal curvature
- Astigmatism readings
- Intraocular lens power
- Toric-lens planning
- Multifocal-lens suitability
- Postoperative satisfaction
The patient may need a period of surface treatment before measurements are repeated.
Frequently Asked Questions
Why are my eyes dry even though they keep watering?
The watering may be reflex tearing caused by surface irritation.
The tears may lack sufficient oil to remain on the eye.
Why does blinking improve the blur?
Blinking temporarily reforms the tear film and smooths the corneal surface.
Why are my eyes worse in air conditioning?
Moving dry air increases tear evaporation.
Why are my eyes worse at the end of the day?
Tear stability, blink quality and ocular-surface tolerance may decline after prolonged visual activity.
Why are my eyes worse in the morning?
Possible causes include:
- Sleeping with the eyes partly open
- Overnight tear-film changes
- Eyelid inflammation
- Recurrent corneal erosion
- Ointment residue
Why do my eyes burn when I apply artificial tears?
Possible reasons include:
- Preservative sensitivity
- Severe surface damage
- An ingredient that does not suit the eye
- Temporary pH or concentration differences
- Allergy
Persistent significant burning should be discussed with the clinician.
Are redness-relief drops good for dry eye?
Drops that constrict blood vessels may make the eye look temporarily whiter without treating the underlying disease.
Repeated use can cause rebound redness and may mask a more important condition.
Can I use saline instead of artificial tears?
Ordinary saline lacks many lubricating and tear-stabilising components.
It may rinse the eye but provides less sustained relief.
Can I wash my eyes with tap water?
Routine flushing with tap water is not recommended for chronic dryness.
Immediate prolonged water irrigation is appropriate after chemical exposure, followed by emergency assessment.
Are gel drops better than ordinary tears?
They last longer but may blur vision more.
The best formulation depends on symptom severity and timing.
Is preservative-free always better?
It is often preferable for frequent use or significant surface disease, but bottle design, cost and convenience also matter.
Can I use artificial tears with glaucoma drops?
Yes.
Separate different drops by at least five minutes.
Use the medicated glaucoma drop first unless instructed otherwise.
Can warm compresses worsen inflammation?
A comfortably warm compress may help blocked meibomian glands.
Excessive heat can irritate rosacea, inflamed skin or the ocular surface.
Should I massage the eyelids firmly?
No.
Massage should be gentle and directed appropriately.
Forceful squeezing may injure the eyelids or cornea.
Do screens permanently dry out the eyes?
Screens commonly worsen symptoms by reducing blinking, but they do not usually permanently destroy tear glands by themselves.
Do blue-light glasses treat dry eye?
They do not restore tear production or meibomian gland function.
A wraparound design may reduce airflow, but the blue-light filter itself is not a recognised treatment for dry eye.
Can dry eye cause headaches?
Dry eye and visual strain may contribute to discomfort around the eyes.
Persistent or severe headache may have another cause.
Can dry eye cause floaters?
No.
True floaters originate in the vitreous inside the eye.
Dry eye can cause surface debris or fluctuating blur that patients may describe imprecisely.
Can dry eye cause flashes?
No.
Lightning-like flashes are more commonly related to vitreoretinal traction, migraine or neurological phenomena.
Can dry eye cause permanent blindness?
Ordinary mild dry eye does not.
Severe untreated ocular-surface disease can occasionally produce infection, scarring or corneal thinning with permanent visual loss.
Can Sjögren disease begin with dry eye?
Yes.
Dry eyes and dry mouth may be early features.
Persistent significant aqueous deficiency may warrant systemic evaluation.
Does drinking more water cure dry eye?
Adequate hydration is sensible, but it does not correct every dry-eye mechanism.
Do omega-3 supplements cure dry eye?
No consistent benefit has been demonstrated across high-quality trials.
Can dry eye worsen after LASIK?
Yes.
Corneal nerve alteration and pre-existing tear-film problems may cause temporary or persistent symptoms.
Can dry eye affect cataract-surgery results?
Yes.
It can reduce measurement accuracy and postoperative visual quality.
Why do symptoms persist even when the eye looks normal?
Possible explanations include:
- Tear-film instability not visible during a brief examination
- Fluctuating disease
- Neuropathic ocular pain
- Environmental triggers
- Another diagnosis
When should I see an eye doctor?
Arrange an assessment when:
- Symptoms persist despite lubricant use
- Vision is affected
- One eye is significantly worse
- Contact lenses become painful
- Dry mouth or autoimmune symptoms are present
- Frequent drops are required
- Symptoms interfere with work, sleep or driving
A Practical Home-Care Plan
Step 1: Reduce Evaporation
- Redirect fans and air conditioning.
- Use wraparound glasses outdoors.
- Consider a humidifier.
- Avoid smoke and fumes.
Step 2: Improve Blinking
- Position screens slightly below eye level.
- Take frequent short breaks.
- Perform slow, complete blinks.
- Avoid staring without blinking.
Step 3: Supplement the Tears
- Use an appropriate lubricant.
- Choose preservative-free drops for frequent use.
- Consider gel or ointment at night when advised.
Step 4: Treat the Eyelids
- Use a warm compress when meibomian blockage is present.
- Perform gentle lid hygiene.
- Treat blepharitis or rosacea.
Step 5: Review Contributing Factors
- Contact lenses
- Medications
- Glaucoma drops
- Previous eye surgery
- Autoimmune symptoms
- Eyelid closure
Step 6: Seek Assessment When Symptoms Persist
Further treatment may include:
- Prescription anti-inflammatory drops
- Punctal plugs
- Meibomian gland procedures
- Serum tears
- Scleral lenses
- Eyelid correction
A Practical Clinical Treatment Ladder
Mild Dry Eye
- Education
- Environmental changes
- Blink modification
- Artificial tears
- Eyelid hygiene when required
Evaporative Dry Eye or Meibomian Gland Dysfunction
- Warm compresses
- Lipid-based lubricants
- Gland expression
- Rosacea treatment
- Thermal pulsation or IPL in selected patients
Inflammatory Dry Eye
- Preservative reduction
- Prescription anti-inflammatory treatment
- Short supervised steroid course
- Cyclosporine or another immunomodulator
Aqueous-Deficient Dry Eye
- Frequent preservative-free tears
- Gel or ointment
- Punctal occlusion after controlling inflammation
- Autoimmune investigation when indicated
Severe Ocular-Surface Disease
- Autologous serum
- Scleral lenses
- Amniotic membrane
- Moisture chambers
- Exposure correction
- Tarsorrhaphy
- Systemic disease treatment
Common Myths About Dry Eye
“Dry eye means the eyes do not produce any tears.”
False.
Many patients produce tears that evaporate too quickly or are of poor quality.
“Watering proves the eyes are not dry.”
False.
Reflex tearing is common in dry eye.
“Any artificial tear should work equally well.”
False.
Formulations differ in viscosity, lipid content, preservatives and intended use.
“More heat is better for blocked glands.”
False.
Excessive heat can burn or irritate the ocular surface.
“Screens are the only cause of modern dry eye.”
False.
Meibomian gland dysfunction, ageing, medication, contact lenses, surgery and systemic disease are also important.
“Dry eye is merely uncomfortable.”
False.
Severe disease can damage the cornea and impair vision.
“Omega-3 supplements are a proven cure.”
False.
Research results are mixed, and a major randomised trial found no superiority over placebo.
“Steroid drops are safe because they make the eye feel better.”
False.
They may raise eye pressure, cause cataract or worsen infection.
“If the tests look mild, the symptoms cannot be severe.”
False.
Corneal nerve abnormalities and neuropathic pain can produce substantial symptoms with limited staining.
“Dry eye treatment is one bottle for everyone.”
False.
Treatment should address the patient’s specific tear, eyelid, inflammatory, exposure and nerve-related factors.
The Bottom Line
Dry eye disease occurs when the tears and ocular surface lose their normal stability.
The main mechanisms are:
- Excessive tear evaporation
- Inadequate watery tear production
- Abnormal tear composition
- Eyelid and blinking problems
- Inflammation
- Altered corneal nerve function
Common symptoms include:
- Burning
- Grittiness
- Redness
- Watering
- Tired eyes
- Light sensitivity
- Fluctuating blurred vision
Common contributors include:
- Meibomian gland dysfunction
- Prolonged screen use
- Air conditioning
- Contact lenses
- Ageing
- Menopause
- Autoimmune disease
- Diabetes
- Medication
- Previous eye surgery
- Eyelid exposure
Treatment may include:
- Preservative-free artificial tears
- Lipid-containing drops
- Warm compresses
- Eyelid hygiene
- Environmental and blink modification
- Anti-inflammatory medication
- Punctal plugs
- Meibomian gland procedures
- Autologous serum
- Scleral lenses
- Eyelid surgery in severe exposure
Seek prompt assessment for:
- Significant pain
- Persistent reduced vision
- Marked redness
- Light sensitivity
- Discharge
- A corneal white spot
- Contact-lens-related symptoms
- Symptoms mainly in one eye
- Dry eye associated with dry mouth or autoimmune features
The best dry-eye treatment is not simply the thickest lubricant. It is a personalised plan that identifies why the tears are unstable and treats the tear film, eyelids, inflammation, exposure and underlying health factors together.
References
- Wolffsohn JS, et al. TFOS DEWS III: Diagnostic Methodology. American Journal of Ophthalmology. 2025.
- Jones L, et al. TFOS DEWS III: Management and Therapy. American Journal of Ophthalmology. 2025.
- Perez VL, et al. TFOS DEWS III: Executive Summary. American Journal of Ophthalmology. 2025.
- American Academy of Ophthalmology. Dry Eye Syndrome Preferred Practice Pattern. Ophthalmology. 2024.
- National Eye Institute. Dry Eye. Updated August 6, 2025.
- Singapore HealthHub. Dry Eye. Reviewed January 8, 2026.
- Singapore HealthHub. Lubricant Eyedrops. Reviewed March 2, 2026.
- National University Health System. Dry Eyes: Signs, Symptoms and Treatment. Updated January 24, 2025.
- Sheppard JD, et al. Dry Eye Disease Associated with Meibomian Gland Dysfunction. 2023.
- Akpek EK, et al. Sjögren Syndrome: More Than Just Dry Eye. 2019.
- Asbell PA, et al. n−3 Fatty Acid Supplementation for the Treatment of Dry Eye Disease. New England Journal of Medicine. 2018.
- Landsend ECS, et al. Lifitegrast in the Treatment of Dry Eye Disease: A Practical Review. 2025.
- Sjögren’s Foundation. Dry Eye and Sjögren Disease.