Author: Dr Val Phua
Estimated reading time: 10–12 minutes
Dry Eye Usually Has More Than One Cause
Dry eye disease is often described as though the eyes simply do not produce enough tears. In reality, many patients produce tears but lose them too quickly because the tear film is unstable or lacks sufficient oil.
Other patients have eyelid inflammation, blocked oil glands, reduced blinking, medication-related dryness or an underlying medical condition. Several causes may occur at the same time.
Understanding the cause matters because treatment that works for one form of dry eye may be less effective for another.
For example:
- Artificial tears may supplement moisture.
- Warm compresses target blocked eyelid oil glands.
- Anti-inflammatory treatment addresses ocular-surface inflammation.
- Changes in screen habits reduce evaporation caused by incomplete blinking.
- Medical investigation may be required when an autoimmune condition is suspected.
Effective treatment therefore begins by identifying why the tear film has become unstable.
How Does the Tear Film Normally Work?
Every time you blink, a thin tear film spreads across the cornea—the clear front surface of the eye.
This tear film has several interacting components.
Oily Layer
The outer oily layer is produced mainly by the meibomian glands within the eyelids.
It slows evaporation and helps keep the tear film stable between blinks.
Watery Component
The lacrimal glands produce the watery component of tears.
This provides moisture, nutrients and protective proteins to the ocular surface.
Mucins
Mucins help the tears spread evenly and adhere to the surface of the eye.
If one or more components are inadequate, the tears may evaporate or break up too quickly. The exposed ocular surface then becomes irritated and inflamed, creating a cycle that further destabilises the tear film.
The Main Mechanisms of Dry Eye
Dry eye is commonly divided into two broad forms:
- Evaporative dry eye
- Aqueous-deficient dry eye
Many patients have a mixture of both.
Evaporative Dry Eye
Evaporative dry eye occurs when tears disappear from the ocular surface too quickly.
The eye may produce a reasonable volume of watery tears, but these tears cannot remain stable because the protective oily layer is inadequate.
Meibomian Gland Dysfunction
Meibomian gland dysfunction is one of the most important causes of evaporative dry eye.
The glands normally release clear oil whenever the eyelids blink. This oil spreads across the tear film and slows evaporation.
When the glands become blocked or dysfunctional:
- The oil may become thick or cloudy.
- Less oil reaches the tear film.
- Tears evaporate more rapidly.
- The eyelid margins may become inflamed.
- Glands may gradually shorten or disappear.
Meibomian gland dysfunction may be associated with:
- Ageing
- Blepharitis
- Rosacea
- Demodex infestation
- Prolonged screen use
- Contact lens wear
- Hormonal changes
- Previous eyelid inflammation
Patients often experience fluctuating vision, burning, tired eyes or symptoms that worsen later in the day.
Reduced or Incomplete Blinking
Blinking performs two important functions:
- It spreads fresh tears over the eye.
- It helps express oil from the meibomian glands.
During concentrated visual tasks, people tend to blink less frequently and may not close their eyelids completely.
This is common during:
- Computer work
- Smartphone use
- Gaming
- Reading
- Online meetings
- Watching television
Reduced blinking allows more evaporation and may also prevent the eyelid glands from functioning normally.
Environmental Exposure
Tears evaporate more quickly in environments with:
- Air conditioning
- Low humidity
- Strong fans
- Wind
- Smoke
- Air pollution
- Prolonged exposure to aircraft cabins
This is particularly relevant in Singapore, where people may spend long periods in air-conditioned offices, classrooms, clinics, shopping centres and vehicles.
Outdoor haze and smoke may also irritate the ocular surface, even when tear production is otherwise adequate.
Eyelid Closure Problems
The eyelids must close fully to protect the cornea and distribute tears.
Exposure-related dryness may occur with:
- Incomplete blinking
- Incomplete eyelid closure during sleep
- Facial-nerve weakness
- Eyelid malposition
- Thyroid eye disease
- Prominent or protruding eyes
- Scarring around the eyelids
- Previous eyelid surgery
Patients may experience worse symptoms on waking if the eyes remain partly open during sleep.
Aqueous-Deficient Dry Eye
Aqueous-deficient dry eye occurs when the lacrimal glands do not produce enough watery tears.
This may result from age-related change, inflammation, medication or an underlying medical condition.
Ageing
Tear production and ocular-surface function may decline with age.
Older adults are also more likely to:
- Take medications that reduce tear production
- Develop eyelid or meibomian gland dysfunction
- Have undergone eye surgery
- Use preserved eye drops
- Have systemic medical conditions associated with dry eye
Dry eye is therefore often multifactorial in older patients.
Sjögren Syndrome
Sjögren syndrome is an autoimmune condition in which the immune system attacks moisture-producing glands.
It may cause:
- Dry eyes
- Dry mouth
- Dental problems
- Joint pain
- Fatigue
- Swelling of the salivary glands
Some patients are first investigated for Sjögren syndrome after an eye examination identifies severe aqueous tear deficiency.
Persistent dry eye accompanied by dry mouth or systemic symptoms should be discussed with a doctor.
Other Autoimmune Diseases
Dry eye may also be associated with:
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Systemic sclerosis
- Autoimmune thyroid disease
- Certain forms of vasculitis
- Graft-versus-host disease
The underlying condition may affect the lacrimal glands, ocular surface, eyelids or corneal nerves.
Lacrimal Gland Damage
Tear production may decrease after:
- Inflammation of the lacrimal glands
- Radiation treatment near the eye
- Trauma
- Surgery involving the lacrimal gland
- Scarring diseases affecting the ocular surface
Blepharitis and Eyelid Inflammation
Blepharitis is inflammation of the eyelid margins.
It may affect the front of the eyelid, the meibomian glands or both.
Features may include:
- Crusting around the eyelashes
- Red or thickened eyelid margins
- Itching
- Burning
- Recurrent styes
- Fluctuating vision
- Contact-lens intolerance
Blepharitis destabilises the tear film and commonly coexists with meibomian gland dysfunction.
Demodex Mites
Demodex are microscopic mites that can live around the eyelashes and within eyelid glands.
In some patients, excessive Demodex infestation contributes to:
- Eyelid inflammation
- Itching
- Cylindrical debris around the lashes
- Meibomian gland dysfunction
- Chronic ocular-surface irritation
Treatment should be directed specifically at the infestation rather than relying only on artificial tears.
Contact Lens Wear
Contact lenses sit within and interact with the tear film.
They may contribute to dryness by:
- Dividing the tear film into separate layers
- Increasing evaporation
- Creating friction during blinking
- Accumulating deposits
- Altering corneal sensation
- Worsening existing meibomian gland dysfunction
Risk increases with:
- Long wearing hours
- Overnight wear
- Poor lens fit
- Older or deposited lenses
- Inadequate replacement
- Air-conditioned environments
- Heavy screen use
Daily disposable lenses, shorter wear and treatment of the underlying ocular surface may improve comfort in selected patients.
Medications That Can Contribute to Dry Eye
Dry eye may be a side effect of systemic or topical medication.
Possible contributors include:
- Antihistamines
- Some antidepressants
- Diuretics
- Certain blood-pressure medications
- Isotretinoin
- Some bladder medications
- Hormonal treatments
- Sedatives
- Selected acne medications
The effect varies considerably between individuals.
Do not stop prescribed medication without speaking to the doctor who prescribed it. Sometimes the dose, timing or medication can be adjusted; in other cases, the dry eye is managed while the medication continues.
Preserved Eye Drops
Some eye drops contain preservatives that reduce bacterial contamination within the bottle.
When used frequently or over many years, certain preservatives may irritate the ocular surface in susceptible patients.
This is especially relevant for people using multiple glaucoma medications.
Options may include:
- Preservative-free formulations
- Reduced dosing frequency
- Combination preparations
- Laser or surgical treatment in selected glaucoma patients
Any change should be discussed with the treating ophthalmologist.
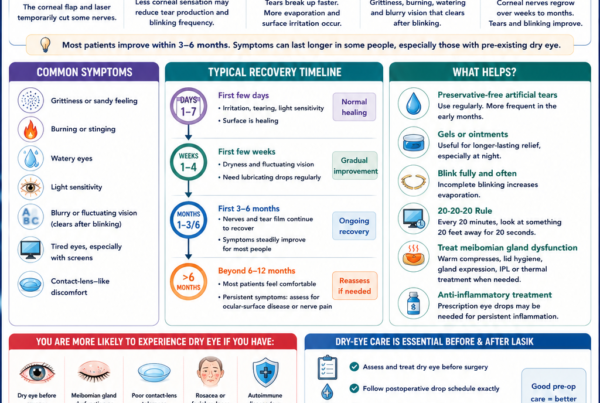
Dry Eye After Eye Surgery
Dry-eye symptoms may appear or worsen after eye surgery.
LASIK, SMILE and PRK
Laser vision correction can temporarily alter corneal sensation and the nerve feedback involved in tear production and blinking.
Pre-existing dry eye or meibomian gland dysfunction may become more noticeable after surgery.
Cataract Surgery
Dry-eye symptoms after cataract surgery may be influenced by:
- Pre-existing ocular-surface disease
- Microscopic corneal incisions
- Postoperative eye drops
- Preservative exposure
- Reduced blinking
- Temporary corneal nerve changes
The ocular surface should ideally be assessed and treated before cataract measurements because an unstable tear film may also affect the accuracy of biometry and refractive planning.
Eyelid and Cosmetic Procedures
Surgery around the eyelids may alter eyelid position, blinking or closure.
Dryness may occur when too much ocular surface remains exposed.
Hormonal Influences
The tear film and meibomian glands are influenced by hormonal pathways.
Dry eye is more common in women and may become more noticeable:
- Around menopause
- During hormonal change
- With certain hormonal medications
- In association with androgen deficiency
Hormones are rarely the only cause, but they may influence gland function and tear stability.
Diabetes
Diabetes may contribute to dry eye through several mechanisms:
- Reduced corneal nerve function
- Altered tear production
- Slower ocular-surface healing
- Meibomian gland dysfunction
- Changes in blinking
- Chronic inflammation
Good glucose control remains important for both general and ocular health.
Thyroid Disease
Thyroid dysfunction may be associated with dry eye even when there is no obvious thyroid eye disease.
When thyroid eye disease is present, the eyes may become prominent and the eyelids may retract, increasing exposure and evaporation.
Incomplete eyelid closure during sleep may cause significant morning discomfort.
Rosacea
Rosacea can affect both the skin and the eyelids.
Ocular rosacea may cause:
- Meibomian gland dysfunction
- Eyelid redness
- Recurrent styes
- Burning
- Light sensitivity
- Corneal inflammation in more severe cases
Some patients have significant eyelid disease without prominent facial symptoms.
Neurological Conditions and Corneal Nerve Dysfunction
The corneal nerves help regulate:
- Tear production
- Blinking
- Ocular-surface sensation
- Healing
Dry eye or dry-eye-like symptoms may occur with neurological conditions, previous viral infections, eye surgery or nerve injury.
The relationship between signs and symptoms is not always straightforward.
Reduced Corneal Sensation
Some patients have substantial ocular-surface damage but relatively few symptoms because corneal sensation has decreased.
Neuropathic Ocular Pain
Other patients experience severe burning, light sensitivity or pain despite relatively mild visible surface changes.
This may reflect abnormal pain processing within the corneal nerves or nervous system rather than tear deficiency alone.
Neuropathic ocular pain requires specialised evaluation and should not simply be treated with increasing amounts of artificial tears.
Vitamin A Deficiency and Nutritional Causes
Vitamin A is required for normal ocular-surface and epithelial health.
Severe deficiency can cause:
- Dryness of the conjunctiva
- Night blindness
- Abnormal corneal changes
- Permanent visual damage in advanced disease
Vitamin A deficiency is uncommon in well-nourished populations but may occur with:
- Severe dietary restriction
- Malabsorption
- Bariatric surgery
- Liver or pancreatic disease
- Certain gastrointestinal conditions
Routine vitamin supplementation is not necessary for most patients with ordinary dry eye.
Pregnancy and Breastfeeding
Hormonal changes during pregnancy or breastfeeding may alter tear production and contact-lens tolerance.
Symptoms are often temporary but should still be assessed if there is significant redness, pain or visual change.
Allergies
Allergic eye disease and dry eye frequently coexist.
Itching is more suggestive of allergy, while burning and fluctuating vision may point towards tear-film instability.
Frequent rubbing and the use of some antihistamines may worsen dryness.
Treating only the allergy—or only the dryness—may leave the other component uncontrolled.
Smoking, Vaping and Air Pollution
Smoke contains irritants that destabilise the tear film and inflame the ocular surface.
Both active and passive smoke exposure may worsen symptoms.
The long-term ocular effects of vaping continue to be studied, but aerosols and chemical exposure may still irritate the eyes and should not be assumed to be harmless.
Can Stress Cause Dry Eye?
Stress does not usually act as a single direct cause, but it may contribute indirectly through:
- Longer screen exposure
- Reduced sleep
- Altered blinking
- Increased pain sensitivity
- Poor adherence to treatment
- Changes in general health
Dry eye symptoms and emotional wellbeing can also influence one another, particularly in chronic or painful disease.
Why Do Symptoms Often Have Several Causes?
A person may simultaneously have:
- Meibomian gland dysfunction
- Heavy screen use
- An air-conditioned work environment
- Contact-lens wear
- Mild aqueous tear deficiency
- Ocular-surface inflammation
Treating only one factor may therefore produce incomplete relief.
This is why the dry-eye assessment should look beyond whether the eye appears “wet” or “dry” at a single moment.
How Is the Cause Identified?
An eye examination may include:
Detailed History
The clinician may ask about:
- Screen use
- Contact lenses
- Environmental exposure
- Medications
- Previous eye surgery
- Medical conditions
- Dry mouth or joint symptoms
- Timing of symptoms
- Sleep and eyelid closure
Tear-Film Assessment
The stability, quantity and appearance of the tears may be evaluated.
Ocular-Surface Staining
Special dyes identify areas of corneal or conjunctival damage.
Eyelid and Meibomian Gland Examination
The glands may be assessed for:
- Blockage
- Thickened secretions
- Inflammation
- Gland loss
- Demodex-related changes
Additional Tests
Depending on the clinical situation, testing may include:
- Tear breakup time
- Tear osmolarity
- Schirmer testing
- Meibography
- Tear-film interferometry
- Corneal topography
- Corneal-sensation testing
- Blood investigations for suspected autoimmune disease
Not every patient requires every test.
When Might Further Medical Investigation Be Needed?
Further assessment may be considered when dry eye is:
- Severe
- Unusually sudden
- Associated with marked dry mouth
- Accompanied by joint pain or fatigue
- Associated with other autoimmune symptoms
- Much worse in one eye
- Resistant to standard treatment
- Accompanied by corneal damage
Depending on the findings, referral to a rheumatologist or another physician may be appropriate.
Warning Signs That Suggest Something Other Than Ordinary Dry Eye
Seek prompt assessment for:
- Severe eye pain
- Sudden reduction in vision
- Marked sensitivity to light
- A white spot on the cornea
- Thick discharge
- Significant one-sided redness
- Recent eye injury
- Chemical exposure
- A painful red eye while wearing contact lenses
These symptoms may indicate infection, inflammation or another urgent eye condition.
Frequently Asked Questions
What is the most common cause of dry eye?
Evaporative dry eye associated with meibomian gland dysfunction is a major contributor, but many patients have several overlapping causes.
Can air conditioning cause dry eye?
Air conditioning lowers humidity and may increase tear evaporation. It commonly worsens an existing tendency towards dry eye, particularly during prolonged screen use.
Can medication cause permanent dry eye?
Some medication-related dryness improves when the medication is changed or discontinued, while other patients have additional underlying causes. Medication should not be stopped without medical advice.
Why is one eye drier than the other?
Unequal symptoms may result from eyelid position, incomplete closure, previous surgery, contact-lens fit, nerve differences or local ocular-surface disease. Persistent one-sided symptoms should be assessed.
Can dry eye occur in young people?
Yes. Heavy screen use, contact lenses, allergies, isotretinoin, autoimmune disease and meibomian gland dysfunction can cause dry eye in younger patients.
Is all dry eye caused by meibomian gland dysfunction?
No. Meibomian gland dysfunction is common, but inadequate tear production, inflammation, medication, eyelid problems and nerve dysfunction may also contribute.
The Bottom Line
Dry eye disease rarely has one universal cause.
The tear film may become unstable because:
- Tears evaporate too quickly.
- The eyes do not produce enough watery tears.
- The eyelid oil glands are blocked.
- Blinking is reduced or incomplete.
- The ocular surface is inflamed.
- Medication, surgery or medical disease affects tear production.
- Corneal nerves process sensation abnormally.
Identifying the dominant causes allows treatment to be directed more precisely.
If symptoms persist despite artificial tears—or if you experience fluctuating vision, contact-lens intolerance, persistent redness or significant discomfort—a comprehensive eye examination can help determine why your eyes are dry and which treatment is most appropriate.
References
- Perez VL, et al. TFOS DEWS III Executive Summary. American Journal of Ophthalmology. 2025.
- Wolffsohn JS, et al. TFOS DEWS III: Diagnostic Methodology. American Journal of Ophthalmology. 2025.
- Stapleton F, et al. TFOS DEWS III Digest. American Journal of Ophthalmology. 2025.
- Bron AJ, et al. TFOS DEWS II Pathophysiology Report. The Ocular Surface. 2017.
- Stapleton F, et al. TFOS DEWS II Epidemiology Report. The Ocular Surface. 2017.
- Gomes JAP, et al. TFOS DEWS II Iatrogenic Report. The Ocular Surface. 2017.
- American Academy of Ophthalmology. Dry Eye Syndrome Preferred Practice Pattern. 2023.
- National Eye Institute. Dry Eye: Causes and Risk Factors.