Author: Dr Val Phua
Estimated reading time: 20 minutes
Cataract surgery removes the eye’s cloudy natural lens and replaces it with a clear artificial intraocular lens, or IOL.
The operation is usually performed as a day procedure under local anaesthesia. Most patients remain awake but should not feel sharp pain. They may see bright lights, colours, shadows or movement without seeing the surgical details clearly.
Modern cataract surgery usually involves five broad stages:
- Examining and measuring the eye
- Selecting the artificial lens and visual target
- Preparing and numbing the eye
- Removing the cloudy natural lens
- Implanting the artificial lens and allowing the eye to heal
Phacoemulsification is the most commonly used modern technique. A small ultrasound probe divides and removes the cloudy lens through a small corneal incision. The outer lens capsule is usually retained so that the new artificial lens can be positioned within it.
Cataract surgery is among the most commonly performed operations and is generally safe and effective.
What Is a Cataract?
A cataract is clouding or increasing optical irregularity within the eye’s natural crystalline lens.
The natural lens is located:
- Behind the cornea
- Behind the coloured iris
- In front of the vitreous gel and retina
It normally helps focus light onto the retina. When it becomes cloudy, light is blocked and scattered rather than being focused cleanly.
This may cause:
- Blurry or hazy vision
- Increasing glare
- Halos or starbursts
- Poor night vision
- Faded colours
- Reduced contrast
- Frequent changes in spectacle prescription
- Increasing short-sightedness
- Double or ghosted images from one eye
Cataract surgery treats the condition by removing the cloudy natural lens rather than attempting to clear it with medication.
When Is Cataract Surgery Needed?
The presence of a cataract does not automatically mean that surgery is required.
Surgery is usually considered when the cataract interferes meaningfully with activities such as:
- Driving
- Night driving
- Reading
- Computer work
- Employment
- Sports
- Cooking
- Walking safely
- Recognising faces
- Managing medication
- Maintaining independence
Surgery may also be recommended when the cataract:
- Prevents adequate examination of the retina
- Interferes with treatment of diabetic or retinal disease
- Contributes to angle closure
- Causes secondary glaucoma
- Causes lens-related inflammation
- Threatens normal visual development in a child
Modern cataract surgery does not require the cataract to become “ripe,” white or extremely dense. Timing is based mainly on visual function, ocular health, patient goals and the expected balance between benefit and risk.
Before Cataract Surgery
Step 1: Confirm That the Cataract Is Causing the Visual Problem
Blur, glare and reduced night vision are not always caused entirely by cataract.
Other possible contributors include:
- Dry eye
- Corneal irregularity
- Keratoconus
- Uncorrected spectacle power
- Macular degeneration
- Epiretinal membrane
- Diabetic macular oedema
- Glaucoma
- Optic-nerve disease
- Retinal detachment
The ophthalmologist therefore assesses whether removing the cataract is likely to improve the symptoms that matter to the patient.
A mild cataract may be present alongside a significant retinal problem. In that situation, cataract surgery may improve brightness but may not remove distortion or restore normal visual acuity.
Step 2: Measure Visual Acuity and Refraction
Vision is usually measured:
- Without spectacles
- With the current spectacles
- After a new refraction
- In each eye separately
Refraction determines whether updated spectacles can still provide satisfactory vision.
Early cataracts may cause:
- Increasing myopia
- Hyperopic change
- Astigmatism
- Unequal prescriptions between the eyes
- Frequent refractive changes
If glasses restore comfortable vision and the patient remains safe and independent, surgery may be deferred.
Glasses cannot correct the internal light scatter, glare and loss of contrast produced by a more significant cataract.
Step 3: Examine the Cataract
A slit-lamp microscope is used to assess:
- Cataract type
- Cataract density
- Lens colour
- Position of the opacity
- Pupil size
- Corneal health
- Anterior-chamber depth
- Lens stability
- Signs of trauma or inflammation
The main cataract patterns are:
- Nuclear sclerotic cataract
- Cortical cataract
- Posterior subcapsular cataract
- Mixed cataract
The appearance of the cataract is interpreted together with the patient’s symptoms.
A relatively small posterior subcapsular cataract may cause severe glare because it lies close to the visual axis. A denser peripheral cataract may produce fewer symptoms.
Step 4: Check the Eye Pressure
Eye pressure is measured to look for:
- Glaucoma
- Ocular hypertension
- Narrow or closed drainage angles
- Lens-related pressure problems
Cataract and glaucoma frequently occur together.
Cataract removal may improve lens-related blur and can also deepen the anterior chamber. Studies indicate that phacoemulsification may lower intraocular pressure in selected patients with glaucoma or ocular hypertension, although it does not restore optic-nerve tissue already lost from glaucoma.
Some patients may undergo cataract surgery together with:
- A minimally invasive glaucoma procedure
- Trabeculectomy
- Glaucoma drainage surgery
- Another pressure-lowering intervention
Step 5: Dilate the Pupil and Examine the Retina
Dilating drops enlarge the pupil so that the ophthalmologist can examine the:
- Retina
- Macula
- Optic nerve
- Retinal blood vessels
- Peripheral retina
This helps identify conditions that may limit vision after surgery, such as:
- Macular degeneration
- Diabetic retinopathy
- Epiretinal membrane
- Macular oedema
- Retinal tears
- Myopic retinal degeneration
- Advanced glaucoma
When the cataract is too dense to see through, ultrasound may be used to determine whether the retina appears attached and whether there is a major abnormality behind the lens.
Ultrasound cannot provide the same detailed assessment of the macula or optic nerve as direct examination and OCT. The final visual potential may therefore remain uncertain until the cataract has been removed.
Step 6: Perform OCT When Indicated
Optical coherence tomography, or OCT, provides cross-sectional imaging of the retina or optic nerve.
Macular OCT may identify:
- Epiretinal membrane
- Macular degeneration
- Macular oedema
- Vitreomacular traction
- Myopic macular disease
Optic-nerve OCT may help evaluate glaucoma.
These findings are important because cataract surgery may clear the optical pathway but cannot reverse permanent retinal or optic-nerve damage.
Step 7: Treat the Ocular Surface
The tear film and corneal surface affect both visual quality and the accuracy of surgical measurements.
Dry eye may cause:
- Fluctuating blur
- Glare
- Burning or grittiness
- Variable corneal measurements
- Inaccurate astigmatism readings
Significant dry eye, blepharitis or meibomian-gland dysfunction may be treated before final biometry.
Treatment may include:
- Lubricating drops
- Lid hygiene
- Warm compresses
- Anti-inflammatory treatment
- Management of eyelid-gland dysfunction
- Repeat measurements after the surface stabilises
Optimising the ocular surface is particularly important when planning:
- Toric IOLs
- Multifocal or trifocal IOLs
- Extended-depth-of-focus IOLs
- Monovision
- Cataract surgery after LASIK, PRK or SMILE
Step 8: Perform Biometry
Biometry measures the dimensions and optical properties of the eye so that the surgeon can calculate the required IOL power.
Measurements may include:
- Axial length
- Corneal curvature
- Anterior-chamber depth
- Lens thickness
- Corneal diameter
- Total corneal astigmatism
Modern IOL calculations use these measurements with mathematical formulas to estimate the lens power most likely to achieve the chosen postoperative target.
Accurate biometric data and appropriate formula selection are central to refractive predictability after cataract surgery.
Measurements may be repeated when:
- The results are inconsistent
- The two eyes differ unexpectedly
- The ocular surface is unstable
- The cataract is extremely dense
- The eye is unusually short or long
- Previous corneal laser surgery has been performed
- A premium IOL is being considered
Step 9: Perform Corneal Topography or Tomography When Needed
Corneal mapping may be recommended when:
- Significant astigmatism is present
- A toric IOL is being considered
- The patient previously underwent LASIK, PRK or SMILE
- Keratoconus is suspected
- The corneal shape appears irregular
- A presbyopia-correcting IOL is being considered
- The refraction and standard keratometry do not agree
Corneal mapping helps distinguish regular astigmatism, which may be corrected by a toric IOL, from irregular astigmatism, which may not be fully corrected by an intraocular lens.
Step 10: Choose the Postoperative Visual Target
Removing a cataract also removes most of the natural lens’s focusing power.
The artificial lens power can be selected to target:
- Distance vision
- Intermediate vision
- Near vision
- Monovision
- A blended-vision strategy
The decision should reflect:
- Work requirements
- Reading habits
- Computer use
- Night driving
- Sports
- Previous spectacle preferences
- Ocular dominance
- Tolerance of visual imbalance
- Willingness to use glasses
The aim is not simply to remove the cataract. It is to create an appropriate refractive plan for both eyes.
Step 11: Choose the Intraocular Lens
Monofocal IOL
A monofocal IOL has one principal focal range.
It may be targeted for:
- Distance
- Intermediate
- Near
Patients targeted for distance normally require reading glasses.
Potential advantages include:
- Good optical quality
- Good contrast
- Fewer lens-related halos than diffractive multifocal designs
- Broad suitability
Toric IOL
A toric IOL corrects regular corneal astigmatism.
It must be:
- Calculated using appropriate measurements
- Inserted at the intended axis
- Rotationally stable
Residual astigmatism may remain because of:
- Measurement variability
- Posterior corneal astigmatism
- IOL rotation
- Irregular corneal shape
- Surgically induced astigmatism
Multifocal or Trifocal IOL
These lenses distribute light between several focal ranges.
They may reduce dependence on glasses for:
- Distance
- Intermediate
- Near
Possible compromises include:
- Halos
- Glare
- Starbursts
- Reduced contrast
- Difficulty in dim lighting
- Greater sensitivity to residual prescription
- Need for neuroadaptation
Extended-Depth-of-Focus IOL
An extended-depth-of-focus, or EDOF, lens aims to create an elongated range of focus.
It may provide:
- Good distance vision
- Improved intermediate vision
- Some functional near vision
Reading glasses may still be required for small print.
Different EDOF lenses use different optical technologies and do not have identical performance or side-effect profiles.
Monovision
Monovision usually targets:
- One eye primarily for distance
- The other eye for intermediate or near vision
Potential advantages include reduced spectacle dependence.
Possible disadvantages include:
- Reduced depth perception
- Visual imbalance
- Difficulty with night driving
- Incomplete near vision
- Adaptation difficulties
A contact-lens simulation may be useful when the patient has not experienced monovision previously.
Step 12: Review Medical Conditions and Medication
The surgical team may ask about:
- Diabetes
- High blood pressure
- Heart disease
- Lung disease
- Kidney disease
- Previous stroke
- Bleeding disorders
- Allergies
- Sleep apnoea
- Neurological conditions
- Difficulty lying flat
- Tremor or movement disorders
Medication history is important.
Particular attention may be given to:
- Blood-thinning medication
- Alpha-blockers used for urinary symptoms
- Steroids
- Glaucoma medication
- Diabetes medication
- Immunosuppressive treatment
- Drug allergies
Alpha-blockers such as tamsulosin may affect pupil behaviour during surgery. Patients should inform the surgeon even when the medication was discontinued years earlier.
Medication should not be stopped unless the surgeon or treating physician specifically advises it.
Step 13: Discuss the Risks and Provide Consent
Although cataract surgery is generally safe, no operation is risk-free.
Possible risks include:
- Infection
- Inflammation
- Corneal swelling
- Eye-pressure changes
- Posterior capsule rupture
- Vitreous loss
- Retained lens material
- Cystoid macular oedema
- Retinal tear or detachment
- IOL displacement
- Residual spectacle power
- Glare or halos
- Posterior capsule opacification
- Rare permanent visual loss
The individual risk varies according to:
- Cataract density
- Pupil size
- Corneal health
- Lens stability
- Previous trauma
- Previous vitrectomy
- Pseudoexfoliation
- Glaucoma
- Diabetes
- Retinal disease
- Previous eye surgery
The consent discussion should also cover:
- The expected visual benefit
- The possibility of needing glasses
- Alternative IOLs
- Alternatives to immediate surgery
- What may happen if surgery is deferred
- The possibility that another condition limits the result
Step 14: Plan Transport and Postoperative Support
Patients usually cannot drive themselves home after cataract surgery.
Arrangements may be needed for:
- Transport home
- An accompanying adult
- Help administering eyedrops
- Assistance with young children
- Time away from work
- Temporary interruption of swimming or strenuous exercise
- Postoperative appointments
Patients receiving sedation may remain drowsy and should follow the facility’s instructions concerning driving, alcohol, legal decisions and operating machinery.
On the Day of Cataract Surgery
Step 15: Registration and Final Checks
On arrival, the team confirms:
- Patient identity
- Eye to be operated on
- Planned IOL
- Refractive target
- Allergies
- Medical history
- Consent
- Fasting status when applicable
The operative eye is marked according to local safety protocols.
Vision, blood pressure or blood glucose may be checked depending on the patient and facility.
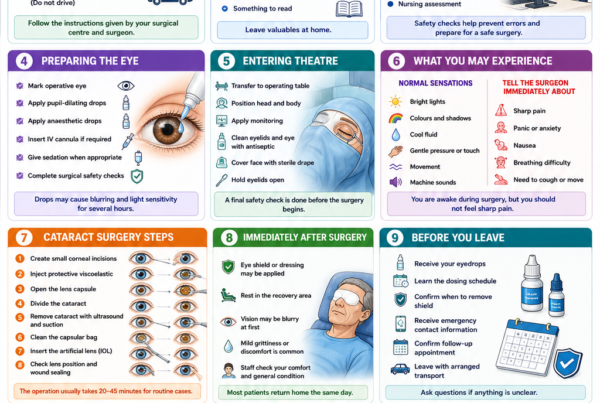
Step 16: Dilate the Pupil
Dilating medication is placed into the eye.
The pupil must usually become sufficiently large so that the surgeon can:
- See the cataract
- Create the capsular opening
- Divide and remove the lens
- Insert the artificial lens safely
Additional measures may be required when the pupil remains small.
These may include:
- Intracameral pupil-expanding medication
- Iris hooks
- A pupil-expansion ring
- Careful mechanical stretching
Step 17: Numb the Eye
Most adult cataract operations are performed under local rather than general anaesthesia.
Anaesthetic options include:
- Topical anaesthetic drops
- Intracameral anaesthetic
- Sub-Tenon’s local anaesthetic
- Peribulbar local anaesthetic
- Sedation combined with local anaesthesia
The choice depends on:
- Patient anxiety
- Ability to cooperate
- Expected complexity
- Eye movement
- General health
- Surgeon and anaesthetist preference
General anaesthesia may be considered for:
- Young children
- Patients unable to remain still
- Severe anxiety that cannot be managed otherwise
- Significant cognitive or movement disorders
- Selected complex operations
The patient may feel touching, cool fluid or gentle pressure, but sharp pain should not ordinarily occur.
What Will I See During Surgery?
Patients may see:
- Bright microscope light
- Colours
- Moving shadows
- Geometrical patterns
- Changes in brightness
- A brief dimming of vision
Most patients cannot see the instruments or procedure in recognisable detail.
Patients should remain still and follow simple instructions. They should tell the surgeon immediately if they experience:
- Sharp pain
- Sudden nausea
- Severe coughing
- Need to move
- Difficulty breathing
The Cataract Operation: Step by Step
Step 18: Clean and Cover the Eye
The eyelids and surrounding skin are cleaned with antiseptic solution.
Antiseptic is also applied to the ocular surface according to the surgical protocol.
A sterile drape covers the surrounding face while leaving the operative eye exposed.
These measures reduce contamination and help lower infection risk.
Step 19: Hold the Eyelids Open
A small instrument called an eyelid speculum gently holds the lids apart.
The patient does not need to worry about blinking.
The other eye is usually covered by the drape.
Step 20: Create the Surgical Incisions
The surgeon creates one or more small incisions near the edge of the clear cornea.
A main incision permits entry of the phacoemulsification probe and IOL injector.
One or more smaller side-port incisions may be used for:
- Manipulating the lens
- Injecting fluid or medication
- Stabilising the eye
- Removing residual lens material
Modern clear-corneal incisions are commonly only a few millimetres wide and often seal without stitches.
Step 21: Fill the Front of the Eye With Viscoelastic
A transparent gel-like substance called an ophthalmic viscosurgical device, or OVD, is injected into the anterior chamber.
It helps:
- Maintain space
- Protect the corneal endothelial cells
- Stabilise the anterior chamber
- Allow controlled manipulation
- Facilitate IOL implantation
Different viscoelastic formulations may be selected according to the eye and surgical step.
Step 22: Open the Front of the Lens Capsule
The natural lens sits within a thin transparent capsular bag.
The surgeon creates a controlled circular opening in the front capsule.
This is called a:
- Capsulotomy
- Continuous curvilinear capsulorhexis
The opening allows access to the cataract while preserving the surrounding capsular bag.
A well-centred, appropriately sized capsular opening helps:
- Keep the IOL stable
- Maintain lens centration
- Support predictable overlap of the IOL edge
- Reduce the chance of an uncontrolled capsular tear
Step 23: Separate the Cataract From the Capsule
Fluid is gently injected around the lens.
This process is called hydrodissection.
It helps separate the cataractous lens material from the surrounding capsule so that the nucleus can rotate and be removed more safely.
In selected eyes, a modified or limited technique may be used to reduce capsular stress.
Step 24: Divide the Cataract
The surgeon uses the phacoemulsification probe and another fine instrument to divide the cataract nucleus into manageable pieces.
Techniques may include:
- Divide and conquer
- Stop and chop
- Phaco chop
- Vertical chop
- Horizontal chop
- Other nucleus-disassembly strategies
The technique is selected according to:
- Cataract hardness
- Pupil size
- Capsular stability
- Corneal endothelial health
- Surgeon preference
A dense cataract generally requires more energy and manipulation than a soft cataract.
Step 25: Remove the Cataract With Phacoemulsification
The phacoemulsification probe uses ultrasound energy to fragment the lens.
At the same time, controlled fluidics:
- Maintain the anterior chamber
- Draw the lens fragments towards the probe
- Aspirate the fragments from the eye
The cataract is removed progressively while the capsular bag is preserved.
The amount of ultrasound energy and fluid used is adjusted according to:
- Lens density
- Fragment size
- Corneal health
- Anterior-chamber depth
- Surgical technique
Phacoemulsification through a small incision is the most common modern method of cataract removal.
Step 26: Remove the Remaining Soft Cortex
After the harder nucleus has been removed, softer cortical lens material may remain attached to the capsular bag.
An irrigation-and-aspiration instrument removes this residual material.
The aim is to leave:
- A clean capsular bag
- An intact posterior capsule
- Adequate support for the IOL
The surgeon avoids excessive stress on the zonular fibres that hold the capsular bag in place.
Step 27: Inspect the Capsular Bag
The surgeon checks:
- Posterior-capsule integrity
- Zonular stability
- Remaining lens material
- Capsular-bag shape
- Suitability for the intended IOL
If the support is not adequate, the lens plan may need to change.
Possible alternatives include:
- Placing the IOL in the ciliary sulcus
- Optic capture
- Using a different IOL design
- Iris fixation
- Scleral fixation
- Leaving the eye temporarily without an IOL
- Implanting a secondary lens later
These changes are uncommon in routine uncomplicated surgery but may be necessary for safety.
Step 28: Refill the Capsular Bag With Viscoelastic
Viscoelastic is injected to:
- Expand the capsular bag
- Create space for the IOL
- Protect the surrounding structures
- Facilitate controlled lens insertion
Step 29: Insert the Artificial Lens
The foldable IOL is loaded into an injector cartridge.
It is inserted through the small corneal incision in a folded form.
Once inside the eye, the lens unfolds.
The IOL usually has:
- A central optical portion
- Flexible supporting arms called haptics
The haptics position the lens within the capsular bag.
Step 30: Position the IOL
The surgeon confirms that:
- The lens has unfolded fully
- Both haptics are correctly positioned
- The optic is centred
- The capsular bag is stable
A toric IOL must be rotated to the intended axis.
Because toric correction depends on alignment, the surgeon checks its orientation carefully before completing the procedure.
Step 31: Remove the Viscoelastic
The viscoelastic is removed from:
- In front of the IOL
- Behind the IOL when appropriate
- The anterior chamber
Removing retained viscoelastic reduces the risk of an early postoperative eye-pressure rise.
The surgeon then restores the eye to an appropriate pressure and depth using balanced fluid.
Step 32: Seal and Check the Incisions
The surgeon checks whether the incisions are watertight.
Fluid may be applied to the corneal wound edges to help them seal.
Most small incisions close naturally without stitches.
A stitch may be placed when:
- The wound does not seal adequately
- A larger incision was required
- The cornea is unusually weak
- A complication occurred
- Additional wound security is desired
Step 33: Administer Medication
Depending on the surgical protocol, medication may be placed:
- Inside the eye
- Around the eye
- On the ocular surface
This may include:
- Antibiotic medication
- Anti-inflammatory medication
- Anaesthetic medication
- Medication to constrict or dilate the pupil
- Eye-pressure medication
Evidence supports intracameral antibiotic prophylaxis as one strategy for reducing postoperative endophthalmitis, although the precise medication and postoperative drop regimen vary by country, facility, allergies and surgeon preference.
Step 34: Remove the Speculum and Drape
The instruments are removed.
The eyelid speculum and sterile drape are taken away.
The eye is checked again.
A clear shield, eye pad or both may be placed over the eye depending on the anaesthesia and surgical protocol.
Immediately After Surgery
Step 35: Rest in the Recovery Area
After surgery, the patient rests in a recovery area.
The team may check:
- Comfort
- Vision
- Eye appearance
- Blood pressure
- General condition
- Instructions for medication and follow-up
Patients generally return home on the same day after the team confirms that they are stable.
What Will Vision Be Like Immediately?
Vision may initially appear:
- Blurry
- Bright
- Hazy
- Distorted
- Tinted
- Temporarily dim
Possible causes include:
- Dilating drops
- Corneal swelling
- Tear-film disturbance
- Viscoelastic
- Inflammation
- Temporary eye-pressure variation
- The eye shield
- Anaesthetic medication
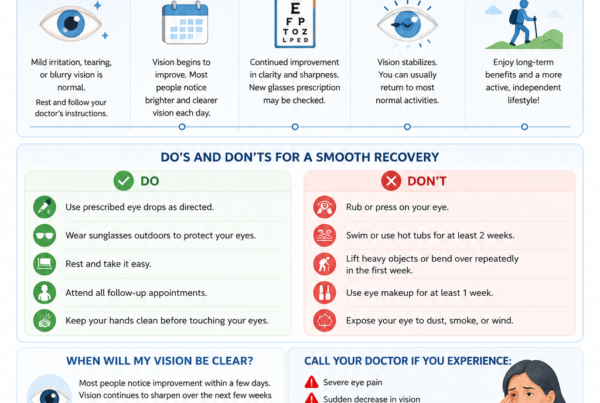
Many patients notice improvement within the first few days, but complete stabilisation takes longer.
Common Early Sensations
During the first few days, patients may notice:
- Mild grittiness
- Watering
- Light sensitivity
- Mild redness
- Slight eyelid swelling
- Awareness of the eye
- A scratchy sensation
Mild discomfort may be normal.
Severe or increasing pain is not expected and requires prompt review.
Postoperative Medication
The exact prescription differs among surgeons and patients.
Drops may include:
- Antibiotic medication
- Steroid medication
- Non-steroidal anti-inflammatory medication
- Lubricating drops
- Eye-pressure medication
The purposes include:
- Reducing inflammation
- Preventing or treating infection
- Controlling pain
- Supporting surface healing
- Reducing macular-oedema risk in selected patients
- Controlling postoperative pressure
Patients should:
- Wash their hands
- Avoid touching the bottle tip to the eye
- Use the medication at the prescribed frequency
- Leave a short interval between different drops
- Continue the medication until instructed otherwise
- Not share eyedrops
If assistance is needed, a family member or caregiver should receive clear instructions.
Follow-Up After Cataract Surgery
The review schedule varies according to:
- Surgical complexity
- Patient health
- Anaesthesia
- Diabetes
- Glaucoma
- Corneal disease
- Retinal disease
- Surgeon and facility protocol
Follow-up may assess:
- Visual acuity
- Eye pressure
- Corneal clarity
- Wound integrity
- Inflammation
- IOL position
- Retina and macula
- Drop adherence
A patient should not skip follow-up simply because the eye feels comfortable.
The First Postoperative Review
The first review may occur:
- On the same day
- The next day
- Within the first few days
The ophthalmologist checks for early issues such as:
- Pressure elevation
- Corneal swelling
- Excessive inflammation
- Wound leakage
- IOL displacement
- Infection
Later Reviews
Subsequent reviews may assess:
- Resolution of inflammation
- Visual recovery
- Refractive stability
- Macular oedema
- Ocular-surface recovery
- Need for new spectacles
- Timing of second-eye surgery
Recovery Timeline
First 24 Hours
Vision may remain blurry.
Patients should:
- Use prescribed drops
- Wear the shield when instructed
- Avoid rubbing the eye
- Avoid driving
- Rest as needed
- Follow bathing and face-washing instructions
First Week
Vision often improves substantially.
Mild:
- Grittiness
- Light sensitivity
- Redness
- Fluctuation
may persist.
Patients should avoid direct trauma, contaminated water and activities specifically restricted by the surgeon.
First Few Weeks
Inflammation and corneal swelling continue settling.
The patient may notice:
- Changing clarity
- Different colour perception between the eyes
- Visual imbalance
- Dry-eye symptoms
- Greater awareness of floaters
The eye’s prescription gradually stabilises.
Four to Eight Weeks
Many uncomplicated eyes have largely healed during this period, although the precise recovery time varies.
Final spectacles may be prescribed when:
- The refraction is sufficiently stable
- Both eyes have been treated when appropriate
- The ocular surface is stable
- Macular and corneal recovery is satisfactory
The National Eye Institute notes that complete healing may take approximately eight weeks in many patients.
What Should Be Avoided After Surgery?
Instructions vary, but patients are commonly advised temporarily to avoid:
- Rubbing or pressing the eye
- Swimming
- Hot tubs
- Contaminated water
- Eye makeup
- Dusty or dirty environments
- Contact sports
- Heavy straining
- Direct trauma
- Driving until cleared
Normal walking and light daily activity may usually resume relatively early, but the surgeon’s instructions should take priority.
Can I Bend Over?
Brief gentle bending is not automatically harmful after uncomplicated modern surgery.
However, patients may be advised to avoid prolonged deep bending, heavy straining or lifting during the early healing period.
Specific advice depends on:
- Surgical complexity
- Wound security
- Eye pressure
- Other eye procedures performed
- General health
Can I Shower or Wash My Hair?
Usually, yes, with appropriate care.
Patients may be instructed to:
- Keep soap and dirty water out of the eye
- Avoid forceful splashing
- Avoid rubbing the eyelids
- Pat the surrounding skin gently
When Can I Drive?
Driving should resume only when:
- Vision meets legal requirements
- The surgeon confirms that recovery is satisfactory
- The patient can judge distance safely
- Glare is manageable
- Binocular balance is adequate
- The patient is no longer affected by sedation
A patient may see clearly in one eye but still be unsafe because of imbalance between the operated and unoperated eyes.
When Can I Return to Work?
The timing depends on:
- Type of work
- Visual demands
- Exposure to dust or contamination
- Physical exertion
- Surgical complexity
- Whether the other eye sees well
Office work may resume earlier than:
- Heavy manual work
- Construction
- Swimming instruction
- Contact-sport work
- Occupations involving dust or chemicals
Normal Changes After Surgery
Colours May Look Brighter
A cataract often develops a yellow or brown tint.
After removal, patients may notice that:
- Whites appear brighter
- Blues appear more vivid
- Colours seem cooler
- The operated and unoperated eyes perceive colour differently
The brain generally adapts over time.
Vision May Fluctuate
Fluctuation may result from:
- Dry eye
- Corneal healing
- Inflammation
- Pupil changes
- Refractive stabilisation
Vision that clears after blinking often suggests a tear-film component.
Floaters May Become More Noticeable
A clearer lens allows patients to see pre-existing vitreous floaters more distinctly.
Cataract surgery does not necessarily create every floater that becomes visible afterwards.
A sudden shower of new floaters, especially with flashes or a shadow, requires urgent retinal examination.
The Two Eyes May Feel Unequal
Before second-eye surgery, the patient may experience:
- Different spectacle powers
- Different image sizes
- Different colour perception
- Reduced depth perception
- Difficulty tolerating old spectacles
Temporary spectacle adjustment, removal of one lens or earlier second-eye surgery may be considered depending on the situation.
Warning Symptoms After Cataract Surgery
Seek urgent assessment for:
- Sudden or rapidly worsening vision
- Severe or increasing eye pain
- Marked redness
- Significant discharge
- Increasing light sensitivity
- Nausea or vomiting with eye pain
- A new curtain or shadow
- New flashes
- A sudden shower of floaters
- Eye trauma
- Worsening swelling
- A white spot on the cornea
These symptoms may indicate:
- Endophthalmitis
- Acute eye-pressure elevation
- Retinal tear or detachment
- Corneal infection
- Severe inflammation
- Wound complication
Postoperative endophthalmitis is uncommon but potentially sight-threatening and requires urgent treatment.
Possible Complications
Corneal Swelling
Temporary corneal oedema may cause:
- Hazy vision
- Halos
- Light sensitivity
Risk may be higher with:
- Dense cataracts
- Greater ultrasound energy
- Pre-existing endothelial disease
- Complex surgery
Most mild swelling improves with time and medication.
Severe endothelial failure may require additional treatment or corneal transplantation.
Eye-Pressure Rise
Pressure may increase because of:
- Retained viscoelastic
- Inflammation
- Steroid response
- Pre-existing glaucoma
- Retained lens material
Treatment may include:
- Pressure-lowering drops
- Oral medication
- Removal of retained viscoelastic or lens material
- Glaucoma treatment
Posterior Capsule Rupture
The back of the capsular bag may tear during surgery.
This can alter:
- Lens removal
- Vitreous management
- IOL positioning
- Postoperative treatment
Many patients still achieve good vision after appropriate management, but additional treatment or surgery may be required.
Retained Lens Material
A lens fragment may remain:
- In the anterior chamber
- Behind the iris
- Within the vitreous
Small soft fragments may resolve with treatment.
Larger nuclear fragments may require vitrectomy by a retinal surgeon.
Cystoid Macular Oedema
Inflammatory swelling may develop at the macula.
Symptoms include:
- Blurred central vision
- Distortion
- Delayed visual recovery
Treatment may include:
- Anti-inflammatory drops
- Steroid treatment
- Injection therapy in selected cases
- Management of underlying retinal disease
Retinal Tear or Detachment
Warning symptoms include:
- Flashes
- A sudden increase in floaters
- A curtain or shadow
- Peripheral field loss
Risk may be higher in:
- High myopia
- Younger patients
- Previous retinal tears
- Previous retinal detachment
- Complicated surgery
Urgent retinal examination is required.
Endophthalmitis
Endophthalmitis is a serious infection within the eye.
Possible symptoms include:
- Increasing pain
- Rapidly worsening vision
- Marked redness
- Increasing light sensitivity
- Eyelid swelling
- Discharge
Urgent intravitreal treatment and sometimes surgery may be needed.
Residual Refractive Error
The result may differ from the intended target.
Possible reasons include:
- Biometric measurement variation
- Formula limitations
- Corneal healing
- Astigmatism
- IOL position
- Previous LASIK or PRK
- Unusual eye length
Management may include:
- Spectacles
- Contact lenses
- Corneal laser enhancement
- Piggyback IOL
- IOL exchange in selected cases
IOL Rotation or Displacement
A toric lens may lose some astigmatic effect if it rotates.
An IOL may rarely become:
- Decentred
- Tilted
- Dislocated
This is more likely with weak zonules or capsular instability.
Treatment may involve:
- Repositioning
- Fixation
- Exchange
- Observation when displacement is minor
Posterior Capsule Opacification
Months or years after surgery, the back of the capsular bag may become cloudy.
This is called:
- Posterior capsule opacification
- PCO
- After-cataract
- Secondary cataract
The original cataract has not grown back.
PCO is usually treated with YAG laser capsulotomy, which creates an opening in the cloudy capsule.
Does Cataract Surgery Use a Laser?
Standard phacoemulsification uses ultrasound rather than a laser to remove the cataract.
A femtosecond laser may assist selected stages, such as:
- Corneal incisions
- Capsulotomy
- Initial lens fragmentation
- Astigmatic corneal incisions
The surgeon must still:
- Enter the eye
- Remove the lens fragments
- Aspirate residual cortex
- Implant the IOL
Studies generally find that both femtosecond laser-assisted cataract surgery and conventional phacoemulsification are safe and effective. Laser assistance can reduce ultrasound energy and create precise capsulotomies, but it has not consistently produced superior visual acuity for every routine patient.
Femtosecond laser assistance does not eliminate:
- Surgical risk
- Need for accurate biometry
- IOL side effects
- Need for postoperative medication
- Possibility of residual prescription
- Need for surgeon judgement
What Is Manual Small-Incision Cataract Surgery?
Manual small-incision cataract surgery, or MSICS, removes the cataract nucleus through a self-sealing scleral or corneoscleral tunnel without using phacoemulsification to divide it completely inside the eye.
It may be useful for:
- Very dense cataracts
- High-volume surgical settings
- Limited access to phacoemulsification technology
- Selected complex eyes
Phacoemulsification and MSICS are both widely practised. Evidence suggests that both can provide good postoperative visual acuity, although their incision sizes, recovery patterns, equipment requirements and complication profiles differ.
What Is Extracapsular Cataract Extraction?
Extracapsular cataract extraction uses a larger incision to remove the lens nucleus largely in one piece while retaining the posterior capsule.
It is used much less frequently for routine cataracts but may be considered when:
- The cataract is exceptionally dense
- Phacoemulsification is unsuitable
- Equipment limitations exist
- A complication requires conversion to a larger-incision technique
A larger incision may require stitches and may produce:
- Slower recovery
- Greater astigmatism
- More wound-related considerations
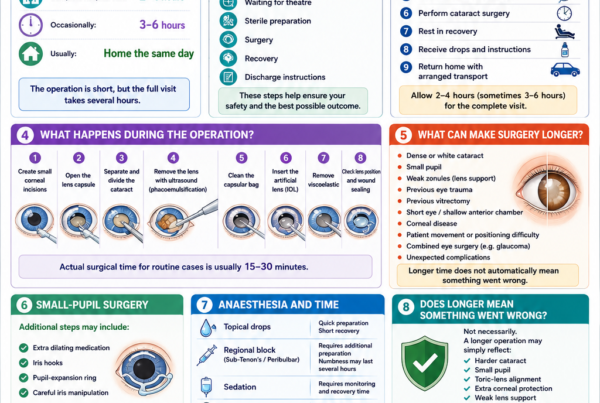
What Changes in a Complex Cataract?
The exact steps may be modified for particular problems.
Small Pupil
The surgeon may use:
- Intracameral medication
- Iris hooks
- Pupil-expansion ring
- Mechanical stretching
Weak Zonules
Weak lens-support fibres may occur with:
- Pseudoexfoliation
- Previous trauma
- High myopia
- Previous vitrectomy
- Connective-tissue disorders
The surgeon may use:
- Capsular hooks
- Capsular-tension ring
- Modified capsular-tension device
- Alternative IOL fixation
Dense White Cataract
Additional measures may include:
- Capsule-staining dye
- Controlled decompression
- Modified capsulorhexis technique
- Greater corneal protection
- Alternative nucleus-disassembly method
Previous Vitrectomy
The eye may have:
- A deeper, less stable anterior chamber
- Reduced vitreous support
- Faster cataract progression
- Zonular weakness
- Retinal disease limiting the result
Previous LASIK, PRK or SMILE
Corneal refractive surgery alters the relationship between measured corneal curvature and true corneal power.
Planning may require:
- Historical treatment data
- Corneal topography
- Modern post-refractive formulas
- Additional counselling about refractive predictability
- Intraoperative aberrometry in selected cases
A 2025 American Academy of Ophthalmology review found that intraoperative aberrometry may provide additional value in selected eyes, but it does not uniformly outperform modern preoperative formulas in every situation.
Are Both Eyes Operated on at the Same Time?
Cataract surgery is commonly performed one eye at a time.
Advantages include:
- Assessing the first eye’s recovery
- Confirming the refractive result
- Adjusting the second-eye target when needed
- Avoiding simultaneous bilateral complications
- Allowing adaptation to the selected IOL
Immediate sequential bilateral cataract surgery may be offered in selected patients and facilities using strict separation protocols.
It is not appropriate for every patient, particularly when:
- The first eye’s result may influence the second-eye plan
- Surgical complexity is high
- Infection risk is increased
- Significant corneal or retinal disease is present
- Different anaesthetic arrangements are needed
When Is the Second Eye Operated On?
The interval depends on:
- Recovery of the first eye
- Cataract severity in the second eye
- Visual imbalance
- Refractive target
- Patient preference
- Medical circumstances
- Surgeon and facility protocol
Second-eye surgery may be considered when the remaining cataract causes:
- Poor binocular balance
- Large prescription difference
- Reduced depth perception
- Continued glare
- Poor night vision
- Difficulty tolerating spectacles
- Reduced mobility
Frequently Asked Questions
Is Cataract Surgery Painful?
Most patients do not experience sharp pain.
They may notice:
- Pressure
- Touching
- Cool fluid
- Bright light
- Mild discomfort
The patient should tell the surgeon immediately if sharp pain occurs.
Will I Be Awake?
Most adults remain awake under local anaesthesia.
Sedation may be used to reduce anxiety.
General anaesthesia is reserved for selected situations.
Can I Blink During the Operation?
The eyelids are held open with a speculum, so blinking is not a problem.
What Happens if I Move?
Small natural movements can usually be managed.
Patients should warn the surgeon before:
- Coughing
- Sneezing
- Moving the head
- Adjusting position
Sudden movement should be avoided.
Will I See the Surgery?
Most patients see light, colour and movement rather than the surgical instruments in recognisable detail.
How Long Does the Operation Take?
An uncomplicated cataract operation is often relatively short, but the total visit is longer because of:
- Registration
- Pupil dilation
- Preparation
- Anaesthesia
- Surgery
- Recovery
- Discharge checks
More complex surgery may take longer. Cataract surgery is usually performed on an outpatient basis and commonly takes less than an hour, although duration varies.
Is the Whole Natural Lens Removed?
The cloudy lens contents are removed.
Most of the transparent capsular bag is retained to support the IOL.
Can the Cataract Grow Back?
No.
The removed natural lens cannot regrow.
Posterior capsule opacification can later cause cloudy vision but is not recurrence of the original cataract.
Will the Artificial Lens Wear Out?
Modern IOLs are designed to remain permanently within the eye.
Routine replacement is not required.
Can I Feel the IOL?
Normally, no.
The lens is positioned inside the eye and cannot usually be felt.
Will I Still Need Glasses?
Possibly.
The need depends on:
- IOL type
- Refractive target
- Corneal astigmatism
- Biometric accuracy
- Healing
- Retinal and optic-nerve health
- Visual task
Even patients with multifocal or EDOF lenses may require glasses for selected tasks.
Does a Toric Lens Guarantee No Astigmatism?
No.
It reduces regular corneal astigmatism but does not guarantee complete correction.
Does a Multifocal Lens Guarantee Freedom From Glasses?
No.
It may reduce spectacle dependence but can produce halos, glare and reduced contrast.
Can Cataract Surgery Correct Presbyopia?
It removes the natural lens and therefore eliminates natural accommodation.
Presbyopia-management strategies include:
- Monovision
- Multifocal or trifocal IOL
- EDOF IOL
- Reading glasses
No artificial lens perfectly reproduces the focusing ability of a young natural lens.
Can Cataract Surgery Correct Myopia?
The IOL power can be chosen to reduce myopia substantially.
High-myopia patients still retain the retinal risks associated with an elongated eye.
Can Cataract Surgery Correct Astigmatism?
Regular astigmatism may be reduced using:
- Toric IOL
- Corneal relaxing incisions
- Incision placement
- Later laser correction
Irregular astigmatism is more difficult to correct.
Can Cataract Surgery Improve Glaucoma?
Removing the cataract may improve the view and may lower pressure in selected eyes.
It cannot restore optic-nerve damage.
Can Cataract Surgery Improve Macular Degeneration?
It may improve brightness, contrast and cataract-related blur.
It does not cure macular degeneration.
Can Cataract Surgery Be Repeated?
The original cataract cannot recur.
Additional surgery may be required for:
- IOL displacement
- Residual refractive error
- Retained lens fragments
- Retinal complications
- Corneal problems
- IOL exchange
PCO is usually treated with laser rather than repeating cataract surgery.
When Can I Exercise?
Light walking may resume relatively early.
More strenuous exercise should follow the surgeon’s instructions.
The timing depends on:
- Surgical complexity
- Eye pressure
- Wound status
- Combined procedures
- Type of sport
When Can I Swim?
Swimming is usually avoided during the early healing period because of contamination and infection risk.
The surgeon should confirm when it is safe to resume.
When Can I Fly?
Air travel is usually possible after uncomplicated cataract surgery when the surgeon is satisfied with recovery.
Flying restrictions are different when gas has been placed inside the eye during retinal surgery.
When Are New Glasses Prescribed?
New glasses are prescribed when:
- The eye has healed sufficiently
- The refraction is stable
- The second eye has been addressed when appropriate
- The ocular surface is stable
Temporary reading glasses may be used before the final prescription.
What Should I Do if I Miss a Drop?
Follow the clinic’s instructions.
Do not routinely double the next dose unless specifically advised.
What Should I Do if the Bottle Touches My Eye?
The bottle tip may become contaminated.
Avoid touching it again and contact the clinic if there is concern about injury or contamination.
Is Cataract Surgery Safe?
Cataract surgery is generally safe and effective.
The individual risk depends on the health and anatomy of the eye, cataract complexity, general health and surgical factors.
No surgeon can guarantee a complication-free result.
What Is the Most Important Part of Cataract Surgery?
Successful treatment depends on the whole process:
- Correct diagnosis
- Appropriate timing
- Accurate measurements
- Suitable IOL selection
- Careful surgery
- Correct postoperative medication
- Follow-up
- Realistic expectations
The operation itself is only one part of the patient’s cataract journey.
Key Takeaway
Cataract surgery replaces the cloudy natural lens with a clear artificial intraocular lens.
Before surgery, the ophthalmologist:
- Confirms that cataract is causing the symptoms
- Measures vision and spectacle power
- Examines the cornea, lens, retina and optic nerve
- Measures eye pressure
- Performs OCT or corneal mapping when needed
- Measures the eye with biometry
- Selects the IOL and refractive target
- Reviews medical conditions, medication and surgical risks
During surgery, the surgeon generally:
- Dilates and numbs the eye
- Cleans and drapes the operative area
- Holds the eyelids open
- Creates small corneal incisions
- Injects viscoelastic
- Opens the front lens capsule
- Separates and divides the cataract
- Removes it using ultrasound and aspiration
- Removes the remaining cortex
- Inserts the artificial lens into the capsular bag
- Removes the viscoelastic
- Checks that the lens is centred and the wounds are secure
After surgery, the patient:
- Rests in the recovery area
- Returns home on the same day in most cases
- Uses prescribed medication
- Avoids rubbing and contamination
- Attends follow-up examinations
- Watches for urgent warning symptoms
Vision often improves within days, but healing and refractive stabilisation may take several weeks.
Seek urgent assessment for:
- Sudden or worsening vision loss
- Severe or increasing pain
- Marked redness
- Significant discharge
- Increasing light sensitivity
- New flashes
- Many new floaters
- A curtain-like shadow
- Eye trauma
Cataract surgery is not simply the removal of a cloudy lens. It is also a refractive procedure that requires accurate measurements, thoughtful IOL selection, careful surgery and appropriate postoperative care.
References
- National Eye Institute. Cataract Surgery. Updated December 2024.
- National Eye Institute. Cataracts. Updated November 2025.
- American Academy of Ophthalmology. What Are Cataracts? Updated December 2025.
- Mayo Clinic. Cataract Surgery. Updated April 2026.
- Singapore National Eye Centre and SingHealth. Cataract Surgery: Diagnosis, Procedure and Risks.
- Chen SP, Woreta F, Chang DF. Cataracts: A Review. JAMA. 2025;333:2093–2103. PMID: 40227658.
- Gurnani B, et al. Phacoemulsification. StatPearls. Updated 2023.
- Stopyra W. A Review of Intraocular Lens Power Calculation Formulas. 2024.
- Shoshi F, et al. Refractive Outcomes After Cataract Surgery—The Impact of Biometry and Calculation Variables. 2024.
- Pantanelli SM, et al. Intraoperative Aberrometry Versus Preoperative Biometry-Based Formulas for Intraocular Lens Power Selection: An American Academy of Ophthalmology Report. 2025. PMID: 39365199.
- Pichardo-Loera NS, et al. Femtosecond Laser-Assisted Cataract Surgery Versus Conventional Phacoemulsification: Systematic Review and Meta-analysis. 2024. PMID: 38291620.
- Kolb CM, et al. Femtosecond Laser-Assisted Cataract Surgery Versus Conventional Cataract Surgery: Meta-analysis of Randomised Trials. 2020. PMID: 32358416.
- Haji O, et al. Phacoemulsification Versus Manual Small-Incision Cataract Surgery: An Umbrella Review. 2025. PMID: 41393572.
- Gautam M, et al. Intracameral Drug Delivery: A Review of Agents, Indications and Safety. 2023. PMID: 36757304.
- George NK, et al. The Routine Use of Intracameral Antibiotics to Prevent Endophthalmitis After Cataract Surgery. 2018.
- Wadbudhe AM, et al. Endophthalmitis After Cataract Surgery: A Postoperative Complication. 2022. PMID: 36381712.
- Benekos K, et al. The Effect of Phacoemulsification on Intraocular Pressure in Glaucoma and Ocular Hypertension: A Systematic Review and Meta-analysis. 2024. PMID: 38573897.