Author: Dr Val Phua
Estimated reading time: 17 minutes
LASIK can provide rapid, long-lasting correction of myopia, hyperopia and astigmatism in appropriately selected patients. However, having a prescription that can technically be treated does not automatically mean that LASIK is the safest procedure for that eye.
A suitable LASIK candidate generally has:
- An adult, stable prescription
- A healthy and regularly shaped cornea
- Adequate corneal thickness for the planned treatment
- No evidence of keratoconus or corneal instability
- A healthy and well-controlled ocular surface
- No significant cataract, retinal disease or uncontrolled glaucoma
- No active eye infection or inflammation
- Realistic expectations about vision, reading glasses and possible side effects
- A lifestyle that is compatible with a permanent corneal flap
LASIK suitability is determined from the combination of the prescription, corneal structure, tear-film health, age, general health and visual priorities. No single measurement can confirm that LASIK is safe.
What Is LASIK?
LASIK stands for Laser-Assisted In Situ Keratomileusis.
During modern femtosecond LASIK:
- A femtosecond laser creates a thin, hinged corneal flap.
- The flap is gently lifted.
- An excimer laser removes microscopic amounts of tissue to reshape the underlying cornea.
- The flap is repositioned and adheres without stitches.
LASIK permanently changes the corneal shape. It may reduce or eliminate dependence on spectacles and contact lenses, but it does not prevent presbyopia, cataract, glaucoma or future changes in the prescription.
The Typical Suitable LASIK Candidate
A patient is more likely to be suitable when they:
- Are at least 18 to 21 years old, depending on the laser platform and regulatory indication
- Have had little or no prescription change during the preceding year
- Have myopia, hyperopia or regular astigmatism within the laser’s treatment range
- Have normal corneal topography and tomography
- Have sufficient corneal tissue for both the flap and laser correction
- Have no active dry-eye disease, infection or inflammation
- Have good vision with appropriate spectacles or contact lenses
- Understand that some glasses may still be required
- Accept the possibility of glare, halos, dry eye, residual prescription or enhancement
- Can attend the required follow-up visits
FDA-approved platforms differ in their age and refractive requirements. For example, one current LASIK platform is labelled for adults aged 18 or older with a change in spherical equivalent no greater than 0.50 D over the previous year, while another is approved from age 22 with similar stability requirements. Approved treatment ranges also differ by device and country.
How Old Must You Be for LASIK?
Minimum Age
LASIK is not normally performed on children.
FDA-approved laser indications generally begin at either:
- 18 years old, or
- 21 to 22 years old
depending on the specific laser and treatment profile.
However, reaching the minimum legal or regulatory age does not necessarily mean that the eyes are ready for surgery.
Some people in their late teens and early twenties continue to develop increasing myopia. Operating while the prescription is still progressing may provide an initially good result followed by a later return of short-sightedness.
Is LASIK Suitable at 18?
Possibly, but caution is appropriate.
LASIK at 18 may be reasonable when:
- The prescription has remained convincingly stable
- The patient is no longer undergoing significant myopic progression
- Corneal measurements are normal
- There are no ocular-surface or retinal concerns
- The expected benefit justifies permanent corneal surgery
It may be preferable to wait when the spectacle prescription has continued to change or when previous records are unavailable.
Is LASIK Suitable After Age 40?
Yes, selected patients over 40 may still be suitable.
A study involving patients aged 40 to 69 found reasonable safety, efficacy and predictability for appropriately selected myopic and hyperopic patients. However, age-related near-vision loss and natural-lens changes become increasingly important.
LASIK does not prevent presbyopia. If both eyes are corrected fully for distance, reading glasses may be needed even when the patient previously read by removing their myopic spectacles. FDA patient information specifically advises that LASIK does not remove the future need for reading glasses.
Possible strategies include:
- Correcting both eyes for distance and using reading glasses
- Mini-monovision
- Blended vision
- Leaving one eye mildly myopic for near tasks
A contact-lens simulation is often helpful before permanently creating monovision.
Is LASIK Suitable After Age 50?
Possibly, but the natural lens must be examined carefully.
A patient in their fifties may have:
- Early cataract
- Presbyopia
- A changing prescription caused by the natural lens
- Reduced contrast or increasing glare
- A shorter interval before cataract surgery becomes necessary
LASIK reshapes the cornea but does not treat an ageing or cloudy natural lens. Where early cataract is already contributing to symptoms, cataract surgery or lens-based correction may be more appropriate.
How Stable Must the Prescription Be?
A stable refraction is one of the most important LASIK requirements.
Many current regulatory indications define stability as no more than approximately 0.50 D of change during the previous 12 months, although the precise definition varies by laser platform.
The surgeon may compare:
- Previous spectacle prescriptions
- Contact lens prescriptions
- Current manifest refraction
- Cycloplegic refraction
- Measurements from both eyes
- Axial length when progressive myopia is suspected
Why Does Stability Matter?
LASIK corrects the prescription present at the time of surgery. It does not stop the eye from continuing to grow or the natural lens from changing.
If myopia is still progressing:
- Short-sightedness may return
- Glasses may be needed again
- An enhancement may be requested
- Further laser treatment may not be possible if insufficient corneal tissue remains
What Can Make a Prescription Unstable?
Possible causes include:
- Continuing myopia progression
- Pregnancy or breastfeeding
- Poorly controlled diabetes
- Cataract or natural-lens changes
- Certain medications
- Contact lens-related corneal distortion
- Dry-eye-related measurement variability
- Accommodation during refraction
The FDA identifies younger age, pregnancy, breastfeeding, diabetes-related changes and medications that alter vision as factors associated with refractive instability.
What Prescriptions Can LASIK Treat?
LASIK can potentially treat:
- Myopia
- Myopic astigmatism
- Hyperopia
- Hyperopic astigmatism
- Mixed astigmatism
The safe treatment range depends on:
- The excimer-laser platform
- Local regulatory approval
- Corneal thickness
- Corneal shape
- Optical-zone size
- Flap thickness
- Pupil size
- Predicted residual stromal tissue
- The surgeon’s safety criteria
For example, one current FDA-labelled platform includes myopia below −10.00 D, cylinder up to −4.00 D, hyperopia up to +4.00 D and selected mixed astigmatism. Another approved platform has a different myopic and astigmatic range. These numbers are device-specific indications, not universal guarantees of suitability.
Can LASIK Treat High Myopia?
Sometimes.
Higher myopic correction requires greater removal of corneal tissue. This may increase concern about:
- Inadequate residual corneal tissue
- Corneal ectasia
- Refractive regression
- Glare or halos
- Reduced optical quality
- Future enhancement limitations
A patient with −8.00 D may be suitable when the cornea is thick, regular and structurally reassuring, while another patient with −5.00 D may be unsuitable because of abnormal tomography or insufficient tissue.
The degree alone does not determine suitability.
An Implantable Collamer Lens may be preferable when:
- The myopia is high or very high
- Laser treatment would remove excessive corneal tissue
- The cornea is too thin
- Preserving the central cornea is a priority
- Internal eye anatomy is suitable for ICL implantation
Can LASIK Treat Low Myopia?
Yes, but the expected benefit should still justify the risk.
A patient with a low prescription may obtain good unaided vision from LASIK, but they may already function well with occasional spectacles.
Because LASIK permanently changes a healthy cornea, the decision should consider:
- How often glasses are currently required
- Contact lens tolerance
- Lifestyle inconvenience
- Night-driving requirements
- Dry-eye risk
- Willingness to accept possible side effects
Being technically treatable does not mean that surgery is necessary.
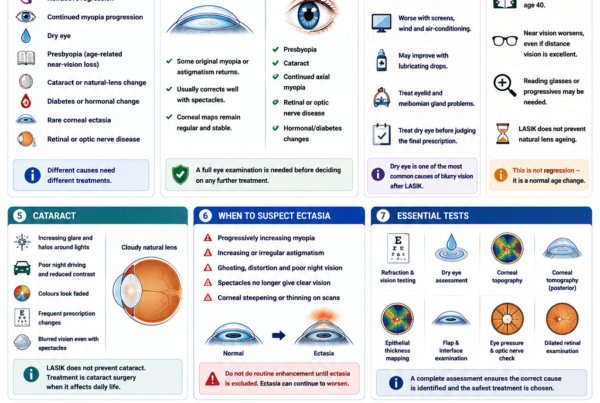
Why Is Corneal Shape Important?
The cornea must be sufficiently regular and structurally stable.
LASIK permanently removes stromal tissue and creates a flap. Performing it on a cornea with an underlying tendency to weaken may contribute to progressive bulging known as corneal ectasia.
Ectasia can cause:
- Increasing myopia
- Progressive irregular astigmatism
- Ghosting
- Reduced best-corrected vision
- Difficulty obtaining clear vision with ordinary spectacles
- Need for rigid or scleral contact lenses
- Need for corneal cross-linking
- Rarely, corneal transplantation
A validated ectasia-screening study found that risk assessment was improved by considering multiple factors together, including corneal topographic pattern, age, preoperative thickness, degree of myopia and predicted residual stromal-bed thickness. Relying only on one thickness cutoff or one topography flag missed a substantial proportion of the ectasia cases studied.
What Corneal Conditions Make LASIK Unsuitable?
LASIK is generally unsuitable when there is:
- Keratoconus
- Forme-fruste or suspected keratoconus
- Pellucid marginal degeneration
- Progressive corneal thinning
- Abnormal posterior corneal elevation
- Concerning pachymetric progression
- Previous corneal ectasia
- Significant corneal scarring
- Unexplained irregular astigmatism
Current FDA labelling lists keratoconus, corneal ectasia, pellucid marginal degeneration and abnormal corneal topography among conditions in which LASIK should not be performed.
What if There Is a Family History of Keratoconus?
A family history does not automatically rule out surgery, but it should increase the level of caution.
The evaluation may require:
- Repeat corneal tomography
- Epithelial thickness mapping
- Corneal biomechanical assessment
- Comparison between the two eyes
- Review of old refractions
- Assessment for eye rubbing and allergy
- Observation over time before deciding
FDA patient information specifically advises patients to disclose a family history of keratoconus, pellucid marginal degeneration or other corneal thinning disorders because apparently normal eyes may have greater susceptibility.
Is Eye Rubbing Relevant?
Habitual vigorous eye rubbing is associated with corneal deformation and is particularly concerning in patients with:
- Allergic eye disease
- Keratoconus susceptibility
- Asymmetric corneal shape
- Progressive astigmatism
Active allergy and habitual rubbing should be controlled before elective corneal surgery.
A patient who cannot stop forceful eye rubbing may be a less suitable candidate even when the initial scans appear reassuring.
How Thick Must the Cornea Be?
There is no single corneal thickness that makes every patient safe or unsafe.
The surgeon must consider:
- Preoperative corneal thickness
- Planned flap thickness
- Laser-ablation depth
- Optical-zone diameter
- Amount of myopia or hyperopia
- Residual stromal-bed thickness
- Percentage of tissue altered
- Corneal tomography
- Age and other ectasia risk factors
One current FDA patient booklet lists central corneal thickness below 480 microns as a precaution for that particular platform. Another FDA-approved system contraindicates treatment when the planned procedure would leave less than 250 microns of residual corneal tissue. These are examples of device-specific labelling and should not be treated as universal safety thresholds.
Many surgeons use additional or more conservative safety margins based on the complete corneal assessment.
Can a Thick Cornea Still Be Unsuitable?
Yes.
A thick cornea can still have:
- Abnormal tomography
- Early keratoconus
- Asymmetric curvature
- Abnormal posterior elevation
- A concerning epithelial pattern
- Excessive planned tissue removal
- Poor biomechanical behaviour
Thickness cannot compensate for an unstable corneal shape.
Can a Thin Cornea Still Be Treated?
Possibly.
A relatively thin but normally shaped cornea may sometimes be suitable for:
- PRK
- TransPRK
- SMILE
- A carefully planned thin-flap LASIK
- ICL surgery
The best choice depends on how much tissue each procedure would affect.
A structurally suspicious thin cornea may be unsuitable for all forms of corneal laser correction.
Is LASIK Suitable if You Have Dry Eyes?
Mild, treatable dry eye does not always exclude LASIK, but the ocular surface should be stable before measurements and surgery.
LASIK temporarily disrupts corneal nerves involved in:
- Tear production
- Blinking
- Corneal sensation
- Ocular-surface regulation
FDA guidance states that severe dry eye is a contraindication for some LASIK systems and that mild or moderate dry eye can worsen following surgery.
A prospective study found that post-LASIK dry-eye risk was associated with higher preoperative myopia and deeper laser ablation. Another prospective analysis found that many patient-reported symptoms improved by six months, illustrating that the course differs between individuals.
Dry-Eye Conditions That Should Be Treated First
These include:
- Meibomian gland dysfunction
- Blepharitis
- Demodex infestation
- Allergic conjunctivitis
- Significant corneal staining
- Tear-film instability
- Aqueous tear deficiency
- Contact lens-related inflammation
- Incomplete eyelid closure
Treatment may include:
- Preservative-free lubricants
- Warm compresses and eyelid hygiene
- Meibomian gland treatment
- Anti-inflammatory medication
- Allergy control
- Temporary discontinuation of contact lenses
- Other targeted dry-eye treatment
The refraction and corneal maps should be repeated after the eye surface has stabilised.
When May Dry Eye Rule Out LASIK?
LASIK may be inappropriate when there is:
- Severe aqueous-deficient dry eye
- Significant autoimmune-related ocular-surface disease
- Persistent corneal staining despite treatment
- Severe contact lens intolerance caused by dryness
- Reduced corneal sensation
- Neuropathic ocular pain
- Exposure keratopathy
- Unstable measurements caused by the tear film
SMILE, PRK, ICL or continued use of spectacles may sometimes be preferable, but these alternatives have their own risks and do not automatically solve dry-eye disease.
Do Large Pupils Make LASIK Unsuitable?
Not automatically.
Large pupils in dim lighting may increase the likelihood or awareness of:
- Halos
- Glare
- Starbursts
- Ghost images
- Reduced night-time contrast
- Difficulty driving in rain or fog
The effect also depends on:
- Optical-zone diameter
- Degree of correction
- Treatment centration
- Pre-existing optical aberrations
- Residual prescription
- Dry eye
- Laser profile
FDA guidance advises measuring pupils under dim-light conditions and counselling patients with large pupils about possible night-vision symptoms.
A large pupil is therefore a counselling and planning factor rather than an automatic disqualification.
Must the Eyes Otherwise Be Healthy?
Yes.
LASIK corrects refractive error. It does not treat diseases of the:
- Retina
- Macula
- Optic nerve
- Natural lens
- Ocular surface
A patient may have technically successful corneal surgery but remain dissatisfied if another eye condition limits visual potential.
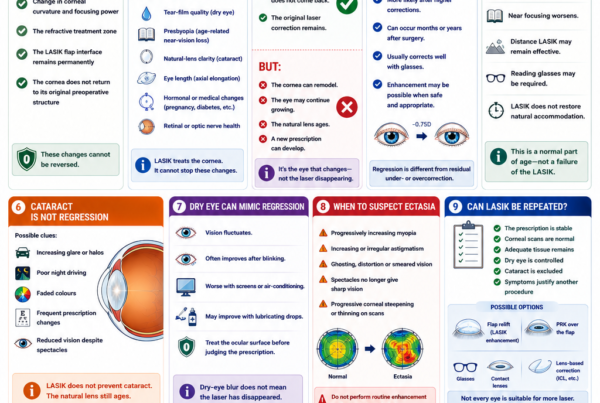
Is LASIK Suitable if You Have Cataract?
Usually not when the cataract is already affecting vision.
Symptoms of early cataract may include:
- Glare
- Halos
- Difficulty driving at night
- Reduced contrast
- A changing myopic prescription
- Reduced best-corrected vision
- Colours appearing less vivid
LASIK will not remove the cloudy natural lens.
It can also make future cataract-lens calculations more complex, so patients should tell future cataract surgeons that they have had laser vision correction.
When cataract is the main cause of visual symptoms, cataract surgery is generally more appropriate.
Is LASIK Suitable if You Have Glaucoma?
Uncontrolled glaucoma is a contraindication under current FDA laser labelling. Controlled glaucoma or glaucoma suspicion requires individual assessment.
Important considerations include:
- Existing optic nerve damage
- Visual-field loss
- Eye-pressure control
- Corneal thickness
- Steroid response
- Ability to monitor future progression
LASIK changes corneal thickness and biomechanics, which can make conventional eye-pressure readings lower and more difficult to interpret. Postoperative steroid drops can also raise pressure in susceptible patients.
A patient with moderate or advanced glaucoma may gain little from elective refractive surgery if optic nerve disease already limits vision.
Is LASIK Suitable if You Have Retinal Disease?
Retinal disease does not always make LASIK impossible, but visual potential and long-term risk must be assessed.
Particular attention is needed for patients with:
- High myopia
- Retinal tears or holes
- Previous retinal detachment
- Myopic macular degeneration
- Diabetic retinopathy
- Macular oedema
- Epiretinal membrane
- Optic nerve disease
LASIK corrects the corneal focusing error but does not shorten an elongated myopic eye or prevent retinal complications.
A dilated retinal examination is often appropriate, particularly in high myopia or when flashes, floaters or peripheral retinal abnormalities are present.
Can LASIK Improve a Lazy Eye?
LASIK does not cure amblyopia.
Amblyopia is reduced visual development in an eye that never achieved normal corrected vision during childhood.
LASIK may reduce the spectacle prescription, but the operated eye generally cannot be expected to see better than its established best-corrected visual potential.
FDA patient information identifies amblyopia as a condition requiring additional caution and counselling.
Is LASIK Suitable if You Have Strabismus?
Possibly, but careful binocular-vision assessment may be required.
Changing the refractive balance between the eyes can occasionally:
- Unmask double vision
- Disturb a previously compensated eye deviation
- Alter accommodation and convergence
- Affect monovision tolerance
Patients with previous strabismus, patching, prism glasses or intermittent diplopia should tell the surgeon before treatment. FDA patient information notes that patients with a history of strabismus may have an increased risk of double vision after selected LASIK corrections.
Is LASIK Suitable After a Previous Eye Injury or Operation?
It depends on the nature of the previous problem.
Additional caution may be needed after:
- Previous LASIK or PRK
- Radial keratotomy
- Corneal cross-linking
- Corneal transplantation
- Significant corneal injury
- Herpes keratitis
- Retinal surgery
- Glaucoma surgery
- Cataract surgery
The remaining corneal thickness, shape, scarring and visual potential must be reassessed.
Previous refractive surgery is not an automatic indication for further LASIK. FDA guidance advises individual evaluation because another procedure may not be recommended.
Is LASIK Suitable After Herpes Eye Infection?
A previous herpes simplex or herpes zoster eye infection requires significant caution.
Laser surgery may reactivate ocular herpes, and previous infection may have caused:
- Corneal scarring
- Reduced corneal sensation
- Irregular astigmatism
- Impaired healing
- Recurrent inflammation
Recent herpes infection or corneal damage from previous ocular herpes is listed as a contraindication in current FDA patient labelling, while a more remote history remains a warning requiring individual assessment.
Can Someone With Diabetes Have LASIK?
Uncontrolled diabetes is a contraindication because:
- The prescription may fluctuate
- Healing may be delayed
- Infection risk may be greater
- Dry eye may be more significant
- Diabetic retinopathy or macular disease may limit vision
Current FDA labelling distinguishes uncontrolled diabetes from selected controlled diabetes, but advises that even well-controlled patients may have less predictable healing.
Some clinical series have reported acceptable outcomes in carefully selected patients with well-controlled diabetes, while other studies have found increased epithelial complications. This supports an individual rather than automatic approach.
A potential candidate with diabetes should generally have:
- Stable blood glucose control
- A stable refraction
- No significant diabetic retinopathy
- No diabetic macular oedema
- A healthy ocular surface
- No significant corneal neuropathy
- No major systemic complications affecting healing
Can Someone With an Autoimmune Disease Have LASIK?
Active autoimmune or connective-tissue disease is a contraindication under current FDA labelling because of concerns about healing and corneal damage. Controlled disease requires careful case-by-case consideration.
Conditions that may be relevant include:
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Sjögren syndrome
- Inflammatory bowel disease
- Psoriatic disease
- Other connective-tissue disorders
Important considerations include:
- Disease activity
- Ocular involvement
- Dry-eye severity
- Immunosuppressive medication
- Corneal sensation
- Previous inflammatory episodes
- The treating physician’s assessment
Selected patients with stable, controlled systemic disease have undergone LASIK successfully in published clinical series, but these results should not be generalised to active disease or significant ocular-surface involvement.
What Medications May Affect LASIK Suitability?
The surgeon should be told about all prescription, over-the-counter and recreational medications.
Potentially relevant medicines include:
- Isotretinoin
- Systemic steroids
- Chemotherapy
- Immunosuppressants
- Medications that worsen dryness
- Drugs that alter refraction or accommodation
- Medication associated with poor wound healing
Current FDA patient information specifically highlights isotretinoin, steroids, chemotherapy and other treatments that may affect dryness, immunity or healing.
Medication should not be stopped without agreement from the prescribing doctor.
Can LASIK Be Performed During Pregnancy or Breastfeeding?
LASIK is generally postponed during pregnancy and breastfeeding.
Hormonal and fluid changes may cause temporary changes in:
- Refraction
- Corneal thickness
- Corneal curvature
- Tear-film function
- Contact lens tolerance
Current FDA patient labelling lists pregnancy and nursing among situations in which LASIK should not be performed because the cornea and prescription may change temporarily.
Surgery should be reconsidered after:
- Pregnancy has ended
- Breastfeeding has stopped
- Hormonal changes have settled
- The prescription has again demonstrated stability
Is LASIK Suitable for Contact-Sport Athletes?
Possibly, but the permanent flap must be considered.
Activities with repeated risk of direct eye trauma include:
- Boxing
- Martial arts
- Rugby
- Football
- Water polo
- Wrestling
- Military training
- Police or security work
The LASIK flap becomes stable for normal daily life, but severe trauma can disturb it even after the early healing period.
FDA guidance specifically advises patients who participate in contact sports to discuss the increased flap-injury risk.
SMILE or PRK may be preferable when avoiding a hinged flap is a major priority.
Can Pilots, Divers or Military Personnel Have LASIK?
Possibly, but occupational requirements vary.
Before surgery, patients should check the requirements of:
- Civil aviation authorities
- Military services
- Police forces
- Diving organisations
- Transport or commercial-driving employers
- Other occupations with mandated visual standards
The FDA checklist advises patients to confirm whether their career restricts refractive surgery.
The appropriate procedure may also depend on:
- Night-vision standards
- Glare tolerance
- Trauma exposure
- Recovery time
- Documentation requirements
Are Realistic Expectations Part of Suitability?
Yes.
A technically excellent candidate may still be unsuitable if their expectations cannot be met.
LASIK aims to reduce dependence on glasses. It does not guarantee:
- Perfect vision in every environment
- Better-than-glasses vision
- No glare or halos
- No dry eye
- Permanent spectacle independence
- No need for reading glasses
- No future enhancement
- Protection against cataract or retinal disease
The PROWL studies found high overall satisfaction after LASIK, but some patients developed new halos, glare, starbursts, double images or dry-eye symptoms. Dissatisfaction was uncommon, yet the findings support detailed preoperative counselling rather than treating LASIK as risk-free.
What Visual Result Should a Patient Expect?
The likely postoperative result depends partly on the patient’s preoperative best-corrected vision.
LASIK cannot overcome vision limited by:
- Amblyopia
- Retinal disease
- Macular degeneration
- Optic nerve damage
- Corneal scarring
- Cataract
- Irregular astigmatism
The realistic aim is generally to obtain unaided vision that approaches the quality previously achieved with spectacles or contact lenses.
A small residual prescription may remain, and glasses may still be useful for:
- Night driving
- Fine distance detail
- Reading
- Prolonged computer work
- Future prescription changes
What Tests Are Needed Before LASIK?
A complete assessment is more extensive than checking the spectacle prescription.
Refraction and Visual Acuity
The surgeon measures:
- Unaided vision
- Current spectacle correction
- Manifest refraction
- Best-corrected visual acuity
- Prescription stability
Cycloplegic Refraction
Cycloplegic drops temporarily relax the eye’s focusing muscles.
This can help identify:
- Over-minus prescriptions
- Latent hyperopia
- Accommodation-related variability
- A difference between manifest and cycloplegic measurements
Large differences between dilated and undilated refractions may reduce predictability and require further assessment.
Corneal Topography
Topography maps the curvature of the front corneal surface.
It helps assess:
- Regularity
- Astigmatism
- Asymmetry
- Contact lens warpage
- Possible keratoconus
Corneal Tomography
Tomography evaluates the cornea in three dimensions, including:
- Anterior elevation
- Posterior elevation
- Corneal thickness distribution
- Pachymetric progression
- The position of the thinnest point
Modern imaging has improved detection of subtle corneal abnormalities, but screening is not infallible. Post-LASIK ectasia has occasionally occurred despite apparently low preoperative risk, reinforcing the importance of combining multiple measurements and clinical judgement.
Corneal Thickness and Tissue Calculations
The surgeon calculates:
- Expected flap thickness
- Expected ablation depth
- Residual stromal-bed thickness
- Total percentage of tissue affected
- Whether an adequate structural safety margin remains
Epithelial Thickness Mapping
The epithelium can partly mask an irregular underlying stromal shape.
Mapping may help identify:
- Early keratoconus patterns
- Contact lens warpage
- Localised epithelial compensation
- Previous surgical changes
Corneal Biomechanical Assessment
Some clinics use devices that assess how the cornea deforms under an air impulse.
These measurements may add information about ectasia susceptibility, but no biomechanical test can guarantee that ectasia will never occur.
Dry-Eye and Eyelid Assessment
The examination may include:
- Tear-film break-up time
- Corneal and conjunctival staining
- Tear meniscus
- Meibomian gland assessment
- Eyelid margin examination
- Tear production
- Symptom questionnaires
The FDA checklist and current patient labelling emphasise that dry eye should be assessed before treatment.
Pupil Measurement
Pupil size should be assessed under appropriately dim conditions when night vision is relevant.
Eye-Pressure and Optic-Nerve Assessment
The surgeon checks for:
- Ocular hypertension
- Glaucoma
- Suspicious optic nerves
- Previous steroid response
Baseline measurements should be retained because LASIK may affect the interpretation of future pressure readings.
Natural-Lens Examination
The natural lens is examined for:
- Cataract
- Early nuclear change
- Causes of changing refraction
- Causes of glare or reduced contrast
Dilated Retinal Examination
A retinal examination may identify:
- Retinal holes
- Retinal tears
- Lattice degeneration
- Macular disease
- Other conditions limiting visual potential
This is especially important in moderate or high myopia.
Why Must Contact Lenses Be Stopped Before the Assessment?
Contact lenses can temporarily alter:
- Corneal curvature
- Tear-film quality
- Astigmatism
- Corneal topography
- Refraction
The FDA recommends discontinuing contact lenses for an appropriate period before the LASIK examination and surgery.
The required interval depends on:
- Soft or rigid lens type
- Toric lens use
- Overnight wear
- Duration of contact lens use
- Evidence of corneal warpage
- Stability of repeated measurements
Measurements may need to be repeated if the corneal shape continues to change after the lenses are stopped.
Who Is Definitely Not Suitable for LASIK?
LASIK is generally inappropriate when there is:
- Keratoconus or another corneal ectatic disorder
- A cornea too thin for the proposed treatment
- Severe dry-eye disease
- Active corneal infection
- Active keratitis, iritis or uveitis
- Recent ocular herpes infection or significant herpes-related corneal damage
- Active autoimmune or connective-tissue disease
- Uncontrolled diabetes
- Uncontrolled glaucoma
- Pregnancy or breastfeeding
- A prescription that is still changing
- Inadequate residual corneal tissue after the planned treatment
These contraindications are reflected in current FDA laser labelling, although precise criteria differ by device.
Who Requires Extra Caution?
Individualised evaluation is required when there is:
- Mild or moderate dry eye
- Controlled diabetes
- Controlled autoimmune disease
- Controlled glaucoma or glaucoma suspicion
- A history of ocular herpes
- A family history of keratoconus
- Borderline corneal thickness
- Large pupils
- Significant contact-sport exposure
- Previous eye surgery
- Strabismus
- Amblyopia
- High myopia
- Reduced vision that glasses do not fully correct
- A strong tendency to form abnormal scars
- Medications that affect healing
A warning or precaution does not automatically mean that surgery is impossible. It means that the expected benefit must be weighed more carefully against the additional risk.
What if You Are Not Suitable for LASIK?
Being unsuitable for LASIK does not necessarily mean that all refractive surgery is impossible.
SMILE
SMILE may be considered when:
- Myopia or myopic astigmatism is within the treatment range
- Avoiding a flap is important
- Contact-sport participation is relevant
- The cornea is otherwise structurally suitable
- Early dry-eye disruption is a concern
SMILE still removes corneal stromal tissue and is not suitable for unstable or ectatic corneas.
PRK or TransPRK
PRK may be considered when:
- Avoiding a flap is important
- The cornea is relatively thin but otherwise healthy
- Surface treatment leaves a safer structural margin
- Contact or combat sports are relevant
- The patient accepts more discomfort and slower recovery
PRK still carries risks of haze, infection, regression and ectasia.
Implantable Collamer Lens
ICL may be considered when:
- Myopia is high
- Corneal tissue is insufficient
- Preserving the cornea is important
- Corneal laser surgery is unsuitable
- The internal eye anatomy is appropriate
ICL avoids corneal ablation but introduces intraocular risks involving vault, eye pressure, cataract, endothelial cells and infection.
Cataract Surgery
Cataract surgery may be more appropriate when:
- The natural lens is already cloudy
- Glare or reduced contrast is caused by cataract
- The prescription is changing because of the lens
- The patient is older and lens-based correction provides a more logical long-term solution
Spectacles or Contact Lenses
These remain appropriate and safe options for many patients.
Elective refractive surgery is not necessary simply because it is technically available.
Frequently Asked Questions About LASIK Suitability
Am I Suitable for LASIK if My Prescription Is High?
Possibly.
The corneal shape, thickness and calculated tissue removal are more important than the prescription alone. ICL may be preferable if laser treatment would remove excessive tissue.
Am I Suitable if My Cornea Is Thin?
Possibly, but LASIK may not be the safest procedure.
PRK, SMILE or ICL may be considered depending on tomography and tissue calculations. A thin, abnormal cornea may be unsuitable for every corneal laser procedure.
Can I Have LASIK With Dry Eyes?
Mild, treatable dry eye may be stabilised before surgery.
Severe or persistent dry eye can make LASIK unsuitable.
Can I Have LASIK if I Cannot Tolerate Contact Lenses?
It depends on why the contact lenses are intolerable.
Intolerance caused by convenience or lens fit may not be a problem. Intolerance caused by severe dry eye, allergy or corneal inflammation requires treatment and may increase surgical risk.
Can I Have LASIK if I Am 18?
Possibly, but only when the prescription is convincingly stable and the eyes are otherwise suitable.
Waiting may be safer when myopia is still progressing.
Can I Have LASIK After 40?
Yes, but LASIK does not prevent presbyopia.
Reading glasses or a monovision strategy may be needed.
Can I Have LASIK After 50?
Selected patients can, but early cataract and natural-lens changes must be excluded.
Can LASIK Correct Astigmatism?
Yes, LASIK can correct regular astigmatism within the treatment range of the laser platform.
Irregular astigmatism may indicate corneal disease and may not be suitable.
Can LASIK Correct Hyperopia?
Yes, selected hyperopic patients can be treated.
Hyperopic suitability depends on corneal dimensions, centration, age and the amount of correction required.
Can I Have LASIK With Keratoconus?
Routine LASIK is contraindicated in keratoconus because it can worsen corneal instability.
Can I Have LASIK After Corneal Cross-Linking?
Possibly in very selected stable cases, but routine LASIK may not be appropriate.
Alternative surface or lens-based strategies may be considered after careful specialist assessment.
Can I Have LASIK With Glaucoma?
Uncontrolled glaucoma is unsuitable.
Controlled glaucoma or glaucoma suspicion requires careful assessment because postoperative pressure monitoring becomes more complex.
Can I Have LASIK With Diabetes?
Possibly when diabetes is well controlled, the refraction is stable and there is no significant retinopathy, neuropathy or healing concern.
Uncontrolled diabetes is unsuitable.
Can I Have LASIK With an Autoimmune Disease?
Active autoimmune disease is unsuitable.
Stable controlled disease may occasionally be considered after consultation with the treating specialist, but significant dry eye or systemic treatment may still rule it out.
Can I Have LASIK During Pregnancy?
No. Surgery should generally be postponed until pregnancy and breastfeeding are over and the refraction has restabilised.
Can I Have LASIK if I Play Contact Sports?
Possibly, but flap trauma must be considered.
SMILE or PRK may offer a better structural match for patients with repeated impact risk.
Does LASIK Guarantee 6/6 Vision?
No.
The outcome depends on the eye’s preoperative visual potential, measurements, healing and residual prescription.
Will I Never Need Glasses Again?
Not necessarily.
Glasses may still be required for reading, night driving, residual refractive error or future changes.
Can LASIK Be Reversed?
No.
The corneal tissue removed by the excimer laser cannot be replaced.
Does Passing a Basic Screening Mean LASIK Is Safe?
Not necessarily.
A thorough evaluation should assess corneal shape, thickness, tissue calculations, ocular surface, pupil size, natural lens, eye pressure and retinal health.
Key Takeaway
A suitable LASIK candidate is not simply someone who is short-sighted and does not like wearing glasses.
Good candidates generally have:
- A stable adult prescription
- A healthy, regularly shaped cornea
- Adequate corneal tissue
- No evidence of keratoconus or ectasia susceptibility
- A stable ocular surface
- No significant cataract or uncontrolled eye disease
- No active infection or inflammation
- Realistic expectations
- A lifestyle compatible with a permanent flap
Important reasons to postpone or avoid LASIK include:
- Progressive prescription change
- Keratoconus or abnormal tomography
- Insufficient corneal tissue
- Severe dry eye
- Active eye disease
- Uncontrolled diabetes or glaucoma
- Active autoimmune disease
- Pregnancy or breastfeeding
- Significant cataract
- Expectations that surgery cannot realistically meet
Suitability should be determined from a comprehensive examination rather than an online degree or corneal-thickness cutoff.
For some patients, LASIK provides the best combination of rapid recovery, accurate correction and convenience.
For others, SMILE, PRK, ICL, cataract surgery, spectacles or contact lenses provide a safer balance of benefits and risks.
References
- US Food and Drug Administration. ZEISS MEL 90 LASIK Patient Information Booklet. Updated 2024.
- US Food and Drug Administration. LASIK Surgery Checklist.
- US Food and Drug Administration. When Is LASIK Not for Me?
- US Food and Drug Administration. TECHNOLAS TENEO 317 Model 2: Summary of Safety and Effectiveness Data. 2023.
- Randleman JB, Trattler WB, Stulting RD. Validation of the Ectasia Risk Score System for Preoperative LASIK Screening. American Journal of Ophthalmology. 2008;145:813–818. PMID: 18328998.
- El-Naggar MT, et al. Assessment of Preoperative Risk Factors for Post-LASIK Ectasia Development. 2023. PMID: 38073674.
- De Paiva CS, Chen Z, Koch DD, et al. The Incidence and Risk Factors for Developing Dry Eye After Myopic LASIK. American Journal of Ophthalmology. 2006;141:438–445. PMID: 16490488.
- Rush SW, et al. Patient-Reported Dry Eye Outcomes After Myopic Femtosecond LASIK: A Six-Month Prospective Analysis. 2023. PMID: 37521150.
- Eydelman M, Hilmantel G, Tarver ME, et al. Symptoms and Satisfaction of Patients in the Patient-Reported Outcomes With LASIK Studies. JAMA Ophthalmology. 2017;135:13–22. PMID: 27893066.
- Ghanem RC, de la Cruz J, Tobaigy FM, Ang LPK, Azar DT. LASIK in the Presbyopic Age Group: Safety, Efficacy and Predictability in Patients Aged 40 to 69 Years. 2007. PMID: 17382397.
- Halkiadakis I, Belfair N, Gimbel HV. LASIK in Patients With Well-Controlled Diabetes. 2005. PMID: 16338557.
- Fraunfelder FW, Rich LF. LASIK Complications in Diabetes Mellitus. 2002. PMID: 11917170.
- Cobo-Soriano R, Beltrán J, Baviera J. LASIK Outcomes in Patients With Underlying Systemic Contraindications. 2006. PMID: 16647130.
- Garcia-Gonzalez M, et al. Effect of Age on Visual and Refractive Results After LASIK. 2019.
- Alió JL, Muftuoglu O, Ortiz D, et al. A 10-Year Prospective Audit of LASIK Outcomes for Myopia. 2010. PMID: 20153899.