Author: Dr Val Phua
Estimated reading time: 18 minutes
There is no single laser eye surgery that is best for everyone.
LASIK, SMILE and PRK can all provide excellent vision in appropriately selected patients. Comparative studies generally find similar final visual acuity, refractive accuracy and patient satisfaction across the three procedures. Their main differences involve:
- How the cornea is treated
- Speed of visual recovery
- Postoperative discomfort
- Dry-eye effects
- Flap-related risks
- Corneal haze
- Treatment flexibility
- Ease of future enhancement
Long-term reviews have not identified one procedure as universally superior. Recent patient-reported outcome research has also found that LASIK, SMILE and PRK can all provide excellent functional vision with relatively few visual limitations after recovery. [1–3]
The most appropriate procedure is the one that:
- Safely corrects the prescription
- Preserves adequate corneal structure
- Matches the patient’s tear-film health
- Fits the patient’s occupation and lifestyle
- Provides an acceptable recovery period
- Minimises the risks most relevant to that individual eye
For some patients, the best laser procedure is LASIK.
For others, it is SMILE or PRK.
For patients with very high myopia, an unsuitable cornea or significant eye-surface disease, the safest recommendation may be an Implantable Collamer Lens, contact lenses, spectacles—or no elective surgery.
What Is Laser Eye Surgery?
Laser eye surgery changes the shape of the cornea so that light focuses more accurately on the retina.
It can reduce:
- Myopia, or short-sightedness
- Hyperopia, or long-sightedness
- Astigmatism
- Dependence on spectacles and contact lenses
The three main corneal laser procedures are:
- LASIK
- SMILE or another form of small-incision lenticule extraction
- PRK or another form of surface ablation, including TransPRK
All three permanently alter the cornea.
They do not:
- Cure the underlying elongated eye in myopia
- Prevent future prescription changes
- Prevent presbyopia
- Prevent cataract
- Remove the retinal risks associated with high myopia
- Guarantee complete freedom from spectacles
The Main Answer: Which Procedure Is Best?
A broad summary is:
LASIK Is Often Best When:
- The fastest visual recovery is a priority
- Minimal early discomfort is important
- The cornea is sufficiently thick and regular
- Wavefront- or topography-guided treatment is desirable
- Hyperopia or mixed astigmatism requires correction
- A relatively straightforward enhancement pathway is important
- The lifetime risk of significant eye trauma is low
SMILE Is Often Best When:
- Avoiding a corneal flap is important
- The patient plays contact or impact sports
- Early dry-eye disturbance is a concern
- The patient has suitable myopia or myopic astigmatism
- The corneal anatomy is appropriate
- A slightly slower early visual recovery is acceptable
PRK or TransPRK Is Often Best When:
- Avoiding a permanent flap is important
- The cornea is relatively thin but remains suitable for surface ablation
- Contact sports or occupational trauma are concerns
- A surface-based customised excimer treatment is needed
- The patient can accept more discomfort and slower recovery
- LASIK would leave insufficient load-bearing stromal tissue
These are general principles rather than fixed rules.
LASIK, SMILE and PRK at a Glance
LASIK
Main strength: Fast recovery and broad treatment flexibility.
Main limitation: A permanent corneal flap interface remains.
SMILE
Main strength: Small incision with no hinged flap and less early disruption of the anterior corneal nerves.
Main limitation: Treatment is mainly for myopia and myopic astigmatism, and enhancement may be less straightforward.
PRK
Main strength: No flap and preservation of more load-bearing stromal tissue.
Main limitation: More pain, slower visual recovery and a risk of corneal haze.
How Does LASIK Work?
LASIK stands for Laser-Assisted In Situ Keratomileusis.
Modern femtosecond LASIK usually involves two lasers:
- A femtosecond laser creates a thin, hinged corneal flap.
- The surgeon lifts the flap.
- An excimer laser reshapes the underlying corneal stroma.
- The flap is repositioned.
The surface epithelium remains largely intact, which is why discomfort is usually mild and vision improves quickly.
LASIK can potentially treat:
- Myopia
- Hyperopia
- Myopic astigmatism
- Hyperopic astigmatism
- Mixed astigmatism
- Monovision targets
The approved range depends on the laser platform and country.
What Is Bladeless LASIK?
Bladeless LASIK means that the flap is created with a femtosecond laser rather than a mechanical blade.
The term does not mean that no corneal flap is created.
What Is Femto-LASIK?
Femto-LASIK is another term for LASIK in which the flap is created using a femtosecond laser.
What Are Wavefront-Guided and Topography-Guided LASIK?
These describe how the excimer-laser treatment is planned.
Wavefront-guided LASIK uses measurements of the entire eye’s optical aberrations.
Topography-guided LASIK uses detailed measurements of the corneal surface.
These customised profiles may be valuable when:
- Astigmatic accuracy is particularly important
- Corneal optical asymmetry is present
- Night-vision quality is a major concern
- A previous refractive treatment was decentered
- Higher-order aberrations need to be considered
A 2024 meta-analysis found both SMILE and wavefront-guided LASIK safe and effective for myopia and astigmatism, but wavefront-guided LASIK produced more accurate cylinder correction and less induced coma in the included studies. [4]
How Does SMILE Work?
SMILE stands for Small-Incision Lenticule Extraction.
During SMILE:
- A femtosecond laser creates a lens-shaped piece of tissue within the cornea.
- The laser creates a small surface incision.
- The surgeon separates the tissue lenticule.
- The lenticule is removed through the incision.
- Removing it changes the corneal curvature and corrects the prescription.
No broad hinged LASIK flap is created.
The United States FDA indication for the VisuMax SMILE procedure includes myopia with or without myopic astigmatism within a defined range. Approved ranges vary by jurisdiction and laser platform. [5]
Is SMILE Truly Flapless?
SMILE is flap-free in the sense that there is no hinged LASIK flap.
However, the procedure still creates:
- An anterior corneal cap
- A posterior lenticule interface
- A small surface incision
- Internal stromal tissue planes
It is therefore more accurate to describe SMILE as a small-incision, flap-free lenticule procedure.
What Is SMILE Pro?
SMILE Pro is performed using a newer-generation femtosecond laser platform with faster lenticule creation and additional digital-assistance features.
The underlying principle remains small-incision lenticule extraction.
The clinical outcome still depends on:
- Correct patient selection
- Accurate refraction
- Centration
- Lenticule separation
- Surgeon experience
- Postoperative healing
The word “Pro” does not automatically make it the best option for every eye.
How Does PRK Work?
PRK stands for Photorefractive Keratectomy.
During PRK:
- The surface corneal epithelium is removed.
- An excimer laser reshapes the exposed corneal stroma.
- Mitomycin C may be applied when clinically appropriate to reduce haze risk.
- A bandage contact lens is placed.
- The epithelium grows back over the following days.
PRK does not create a flap.
Its final visual results are generally comparable to LASIK for appropriately selected low-to-moderate prescriptions, although the recovery is slower. [6,7]
What Is TransPRK?
TransPRK is a type of surface laser treatment in which the excimer laser removes the epithelium rather than the surgeon removing it manually or using alcohol.
The epithelial and refractive treatments may be performed as a programmed sequence.
Potential advantages include:
- No manual epithelial scraping
- No alcohol-assisted removal
- Reduced instrument contact
- A standardised treatment profile
However, TransPRK remains a surface-ablation procedure.
It still involves:
- Removal of the epithelium
- A bandage contact lens
- Postoperative discomfort
- Slower visual recovery than LASIK
- A risk of corneal haze
“Touch-free” does not mean pain-free or risk-free.
Which Procedure Gives the Best Final Vision?
For appropriately selected patients with myopia, final eye-chart vision is usually similar after LASIK, SMILE and PRK.
A meta-analysis comparing SMILE, femtosecond LASIK and transepithelial PRK found all three to be effective, predictable and safe for myopia, although individual refractive and optical-quality differences were identified. [3]
A 2025 patient-reported outcome study also found that all three procedures produced excellent functional outcomes and relatively few visual symptoms by six months. [1]
The final outcome may depend more on:
- Accuracy of the preoperative refraction
- Corneal topography and tomography
- Treatment centration
- Laser calibration and platform
- Optical-zone planning
- Astigmatism alignment
- Tear-film health
- Individual healing
- Surgeon experience
than on the name of the procedure.
Which Has the Fastest Recovery?
LASIK usually provides the fastest initial recovery.
LASIK Recovery
Many patients notice substantially clearer vision within several hours.
Office-based work may be possible within one to three days.
Fine visual quality may continue improving over several weeks.
SMILE Recovery
Many patients have useful vision by the following day, but the vision may take several days to become fully crisp.
Early symptoms may include:
- Mild haze
- Fluctuating vision
- Reduced contrast
- A slight difference between the eyes
PRK Recovery
PRK has the slowest recovery.
During the first several days, patients may experience:
- Blurred vision
- Watering
- Burning
- Significant light sensitivity
- Grittiness
- Difficulty opening the eyes
Functional vision often improves over one to two weeks, while finer visual quality may continue stabilising over one to three months.
Which Is the Least Painful?
LASIK is generally the most comfortable during early recovery.
SMILE usually causes mild grittiness or watering.
PRK is usually the most uncomfortable because the surface epithelial layer must regenerate.
PRK pain is commonly most noticeable during the first two to three days.
The choice should not be based on pain alone. A few uncomfortable days may be worthwhile when PRK provides a safer structural option for a particular cornea.
Which Procedure Causes the Least Dry Eye?
SMILE often causes less early dry-eye disturbance than LASIK.
Creating a LASIK flap cuts more of the anterior corneal nerve network involved in:
- Corneal sensation
- Blinking
- Tear secretion
- Ocular-surface regulation
SMILE uses a small incision and preserves more of the anterior nerve architecture.
A 2025 meta-analysis of 18 studies found better tear-film stability and some tear-production measurements after small-incision lenticule extraction than after femtosecond LASIK. The difference in patient-reported dry-eye scores was less consistent. [8]
PRK does not create a flap, but it removes the epithelium and superficial nerves. It can therefore also cause temporary dryness and fluctuating vision.
Does SMILE Prevent Dry Eye?
No.
Dry eye can occur after:
- LASIK
- SMILE
- PRK
The risk is influenced by:
- Pre-existing meibomian gland dysfunction
- Blepharitis
- Contact lens intolerance
- Tear production
- Corneal sensitivity
- Screen use
- Eyelid closure
- Autoimmune disease
- Hormonal factors
Significant ocular-surface disease should be treated before any elective refractive procedure.
How Common Are Dry Eye and Visual Symptoms After LASIK?
In the FDA’s LASIK Quality of Life Collaboration Project, up to 28% of participants who reported no dry-eye symptoms before surgery reported some dry-eye symptoms at three months.
The same project found that less than 1% experienced major difficulty with or inability to perform usual activities because of any single visual symptom such as halos, glare, starbursts or ghosting. These findings demonstrate that new symptoms are not rare, but severely disabling functional symptoms were uncommon in the studied groups. [9]
Patients should be informed that excellent eye-chart vision does not guarantee perfect night vision or complete freedom from dry-eye symptoms.
Which Is Best for Contact Sports?
SMILE or PRK may be preferred when the patient has a significant lifetime risk of direct eye trauma.
Examples include:
- Boxing
- Martial arts
- Rugby
- Water polo
- Football
- Military training
- Police or security work
- Occupations involving facial impact
LASIK creates a permanent flap interface. Although late traumatic displacement is rare, a sufficiently strong direct injury can disturb the flap even years after surgery.
SMILE and PRK do not create a hinged flap.
They do not make the eye injury-proof. Trauma can still cause:
- Corneal abrasions
- Infection
- Traumatic inflammation
- Cataract
- Retinal tears
- Retinal detachment
Protective eyewear remains important.
Which Is Best for a Thin Cornea?
A thin cornea does not automatically mean that PRK or SMILE is safe.
The surgeon must evaluate:
- Total corneal thickness
- Front and back corneal elevation
- Pachymetry distribution
- Epithelial thickness
- Treatment depth
- Flap or cap thickness
- Residual stromal tissue
- Percentage of tissue altered
- Corneal biomechanics
- Keratoconus risk
LASIK in Thin Corneas
LASIK requires both:
- A flap
- An excimer-laser ablation
The flap does not disappear, but most flap tissue does not contribute fully to the deeper load-bearing residual stromal bed.
PRK in Thin Corneas
PRK avoids a flap and therefore preserves more load-bearing stromal tissue for a similar excimer-laser correction.
PRK may be suitable when LASIK would leave insufficient structural reserve.
SMILE in Thin Corneas
SMILE avoids a flap but still removes a stromal lenticule.
Its structural suitability depends on:
- Cap thickness
- Lenticule thickness
- Residual stromal bed
- Corneal shape
- The size of the optical correction
A thin, weak or suspicious cornea may be unsuitable for all three procedures.
Which Procedure Preserves the Most Corneal Strength?
PRK generally preserves more load-bearing stromal tissue because no flap or cap is separated across a broad diameter.
SMILE preserves more of the anterior stromal architecture than LASIK because it creates only a small incision rather than a hinged flap.
Biomechanical studies often place the procedures broadly in this order:
- PRK generally preserves the most load-bearing tissue.
- SMILE may preserve more anterior structural continuity than LASIK.
- LASIK introduces the greatest flap-related structural separation.
However, these are general principles.
Actual safety depends on:
- Corneal shape
- Tissue removal
- Optical zone
- Flap or cap thickness
- Prescription
- Age
- Eye rubbing
- Individual susceptibility
No procedure should be selected from a theoretical biomechanical ranking alone.
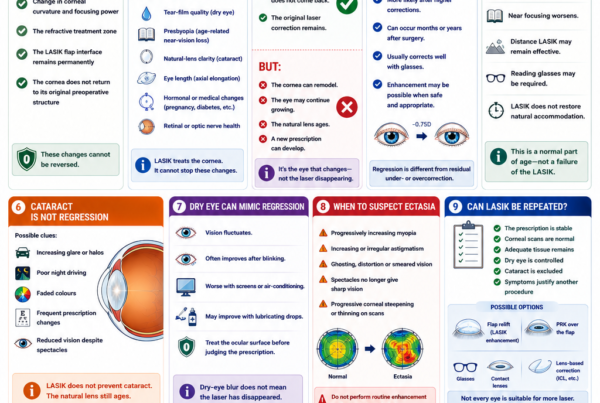
Can Corneal Ectasia Occur After All Three Procedures?
Yes.
Corneal ectasia is progressive thinning, weakening and bulging of the cornea after refractive surgery.
It can cause:
- Increasing myopia
- Irregular astigmatism
- Ghosting
- Reduced best-corrected vision
- Need for rigid or scleral contact lenses
- Need for corneal cross-linking
- Rarely, corneal transplantation
A systematic review found reported ectasia after LASIK, PRK and SMILE. Reported rates differed, but direct comparison is limited by differences in procedure age, case numbers, reporting and preoperative screening. [10]
The most important protection against ectasia is not simply choosing PRK or SMILE instead of LASIK.
It is careful screening for:
- Keratoconus
- Forme-fruste keratoconus
- Abnormal posterior corneal elevation
- Abnormal pachymetry progression
- Epithelial compensation patterns
- Inadequate residual tissue
- Significant eye rubbing
- Other risk factors
Which Is Best for Keratoconus?
Routine LASIK, SMILE and PRK are not appropriate for progressive keratoconus.
Removing corneal tissue can worsen structural instability.
Patients may instead require:
- Observation
- Corneal cross-linking
- Rigid gas-permeable lenses
- Scleral lenses
- Intracorneal ring segments in selected cases
- ICL after the cornea has been shown to be stable
- Corneal transplantation in advanced disease
A “mild” prescription does not make laser treatment safe when the corneal structure is abnormal.
Which Procedure Is Best for High Myopia?
The higher the myopic correction, the more corneal tissue must generally be removed.
High corrections may be associated with:
- Greater tissue removal
- A smaller effective optical zone
- More refractive regression
- Increased higher-order aberrations
- Greater concern about ectasia
- More glare or night-vision symptoms
- A greater chance of enhancement
LASIK, SMILE and PRK can all treat significant myopia within suitable ranges, but a procedure being technically available does not mean it is the safest choice.
For high or very high myopia, an ICL should often be considered because it corrects the prescription without removing central corneal tissue.
ICL is not laser eye surgery. It is an intraocular procedure and introduces different risks, including:
- Cataract
- Raised eye pressure
- Vault problems
- Endothelial cell loss
- Inflammation
- Infection
The choice is therefore between different risk profiles rather than between a “safe” and an “unsafe” procedure.
Which Is Best for Low Myopia?
For low myopia with a healthy cornea, several procedures may produce excellent results.
The decision may be influenced by:
- Recovery preference
- Dry-eye risk
- Contact-sport participation
- Astigmatism
- Need for customised treatment
- Corneal thickness
- Cost
- Surgeon experience
For a very low prescription, the likely benefit should also be weighed against the fact that all surgery carries risk.
Spectacles or occasional contact lens use may remain the most proportionate option for some patients.
Which Is Best for Astigmatism?
LASIK, SMILE and PRK can all correct regular myopic astigmatism.
LASIK and PRK use excimer-laser platforms that may incorporate:
- Iris registration
- Cyclotorsion compensation
- Active eye tracking
- Wavefront-guided treatment
- Topography-guided treatment
SMILE depends on:
- Accurate docking
- Treatment centration
- Astigmatic-axis planning
- Cyclotorsion management
- Complete and symmetrical lenticule extraction
Overall astigmatic outcomes are good with all three procedures, but wavefront-guided LASIK may offer advantages for cylinder accuracy and induced coma in selected comparisons. [4]
The best procedure also depends on whether the astigmatism is:
- Regular
- Irregular
- Stable
- Corneal
- Partly generated by the natural lens
Irregular astigmatism may not be suitable for routine laser correction.
Which Is Best for Hyperopia?
LASIK and PRK have more established roles in treating hyperopia.
Standard SMILE is mainly used for myopia and myopic astigmatism under current widely established indications. [5]
LASIK is often preferred for suitable hyperopic patients because:
- Recovery is faster
- Haze risk is lower
- Hyperopic excimer-laser treatments are well established
- Customised tracking and centration options are available
PRK may still be considered in selected hyperopic patients.
Hyperopic corrections may be more prone to regression than low-to-moderate myopic corrections.
Which Is Best for Presbyopia?
None of the procedures restores natural accommodation.
Presbyopia occurs because the natural crystalline lens becomes less flexible with age.
LASIK, SMILE or PRK may be used to create monovision:
- One eye is corrected primarily for distance
- The other eye is left mildly myopic for near or intermediate vision
Potential limitations include:
- Reduced depth perception
- Reduced stereoacuity
- Eye imbalance
- Night-driving difficulty
- Incomplete near vision
- Adaptation problems
A contact lens trial is advisable before permanent monovision treatment whenever practical.
Patients corrected fully for distance will generally require reading glasses as presbyopia develops.
Which Is Best for Patients Over 40?
Age alone does not determine the procedure.
Important questions include:
- Is the natural lens completely clear?
- Is presbyopia already present?
- Does the patient understand that reading glasses may be required?
- Is there early cataract?
- Is monovision acceptable?
- How long is the corneal correction likely to remain useful before cataract surgery?
A patient in their early forties with a clear lens may remain suitable for corneal laser correction.
A patient with early cataract may be better served by cataract surgery rather than reshaping the cornea in front of a lens that is already becoming cloudy.
Which Procedure Has the Best Night Vision?
There is no universal winner.
All three can produce:
- Halos
- Glare
- Starbursts
- Ghosting
- Reduced contrast
- Difficulty driving at night
Risk is influenced by:
- Pupil size
- Degree of correction
- Optical-zone diameter
- Treatment centration
- Residual astigmatism
- Dry eye
- Higher-order aberrations
- Corneal haze
- Pre-existing night-vision symptoms
LASIK can offer customised wavefront- or topography-guided treatment on appropriate platforms.
SMILE may induce different patterns of higher-order aberrations and may have less early dry-eye disturbance.
PRK avoids a flap interface but may have early haze and slower optical stabilisation.
FDA guidance cautions that glare, halos and double vision can impair low-light vision even when standard eye-chart acuity is good. [11]
Which Is Easiest to Enhance?
LASIK generally offers the most straightforward early enhancement pathway.
Enhancement After LASIK
Options may include:
- Relifting the flap
- Additional excimer-laser correction
- PRK over the flap
- Spectacles
- Contact lenses
Relifting an old flap can carry an increased risk of epithelial ingrowth and may not always be advisable.
Enhancement After SMILE
Options may include:
- PRK over the SMILE cap
- Converting the cap into a LASIK-style flap
- Repeat lenticule extraction in selected cases
- Spectacles
- Contact lenses
- ICL in suitable eyes
Enhancement is possible but may be more technically complex than an early LASIK retreatment.
Enhancement After PRK
Further surface ablation may be possible when:
- The prescription is stable
- Corneal thickness is adequate
- Tomography remains normal
- Previous haze is absent or manageable
- The eye surface is healthy
The patient must undergo another surface-healing period.
Which Has the Best Long-Term Stability?
Within suitable treatment ranges, LASIK, SMILE and PRK all have good long-term evidence.
LASIK and PRK have the longest clinical history.
SMILE now has studies extending to approximately ten years.
A review of long-term outcomes found no clear overall superiority among the procedures and noted that effectiveness was most likely to decline when very high corrections were treated using older technology. [2]
Long-term stability depends on:
- Initial prescription
- Age at treatment
- Continuing axial elongation
- Corneal remodelling
- Natural-lens changes
- Pregnancy
- Hormonal changes
- Diabetes-related refractive changes
- Development of cataract
The laser treatment does not wear off, but the eye can continue to change.
Which Procedure Is the Safest?
Safety is individual.
LASIK Avoids:
- Surface epithelial removal
- Several days of significant discomfort
- PRK haze risk
But introduces:
- A permanent flap
- Flap displacement risk
- Epithelial ingrowth
- Interface inflammation
- Greater early nerve disruption
SMILE Avoids:
- A hinged flap
- Excimer-laser ablation
- Some early anterior corneal nerve disruption
But introduces:
- Lenticule-separation difficulty
- Suction loss
- Retained lenticule tissue
- Cap tears or perforation
- Less straightforward enhancement
PRK Avoids:
- A permanent flap
- Flap displacement
- Epithelial ingrowth beneath a flap
But introduces:
- More pain
- Delayed epithelial healing
- Infection risk while the surface is open
- Corneal haze
- Longer steroid treatment
- Steroid-related pressure elevation
The safest procedure is the one that avoids the greatest risk for that particular patient.
What Are the Main Risks Shared by All Three?
LASIK, SMILE and PRK can all cause:
- Under-correction
- Overcorrection
- Residual astigmatism
- Regression
- Dry eye
- Glare
- Halos
- Starbursts
- Ghosting
- Infection
- Inflammation
- Corneal ectasia
- Reduced contrast sensitivity
- Loss of best-corrected vision
- Need for an enhancement
- Continued need for spectacles
Serious permanent visual loss is rare but possible.
Can Laser Eye Surgery Cause Neuropathic Corneal Pain?
Rarely, patients can experience persistent burning, pain or light sensitivity that is disproportionate to visible surface findings.
This may involve abnormal corneal nerve healing and central pain processing.
Neuropathic symptoms have been described after different refractive procedures, and no procedure eliminates the risk completely.
Patients with significant pre-existing ocular pain, migraine, severe dry eye or unusual nerve symptoms require careful counselling and assessment.
Who May Not Be Suitable for Any Laser Procedure?
Laser eye surgery may be unsuitable when there is:
- Progressive keratoconus
- Suspicious corneal tomography
- Inadequate residual stromal tissue
- Severe uncontrolled dry eye
- Active blepharitis
- Active eye infection
- Unstable refraction
- Pregnancy or breastfeeding
- Uncontrolled systemic disease affecting healing
- Significant cataract
- Moderate or advanced glaucoma
- Vision-limiting retinal disease
- Unrealistic expectations
FDA guidance advises careful evaluation of unstable prescriptions, corneal disease, dry eye, blepharitis and medical conditions that may interfere with healing. [12]
What Does “Stable Prescription” Mean?
A stable prescription generally means that the refractive error has changed very little over a defined period, commonly at least one year.
The exact acceptable change depends on:
- Age
- Procedure
- Laser platform
- Surgeon
- Degree of myopia
- Evidence of continuing axial elongation
A patient whose prescription is still progressing may initially achieve a good result but later become short-sighted again.
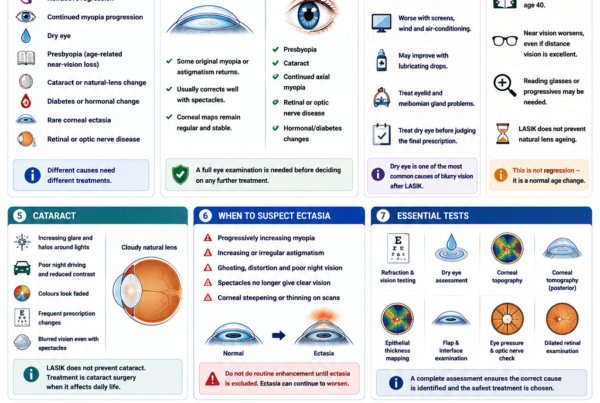
What Tests Are Needed Before Choosing a Procedure?
A refractive assessment should be designed to determine whether surgery is safe—not merely which procedure the patient prefers.
Refraction and Visual Acuity
The assessment measures:
- Myopia or hyperopia
- Astigmatism
- Best-corrected vision
- Prescription stability
Cycloplegic refraction may be performed to relax accommodation.
Corneal Topography and Tomography
These scans assess:
- Front corneal curvature
- Back corneal elevation
- Corneal thickness distribution
- Pachymetry progression
- Keratoconus risk
- Corneal asymmetry
- Treatment centration
Epithelial Thickness Mapping
The corneal epithelium can partly conceal underlying stromal irregularity.
Mapping may help identify:
- Early keratoconus patterns
- Contact lens warpage
- Localised epithelial compensation
- Previous treatment changes
Corneal Thickness and Tissue Calculations
The surgeon estimates:
- Treatment depth
- LASIK flap thickness
- SMILE cap and lenticule thickness
- Residual stromal tissue
- Percentage of tissue altered
- Structural safety margin
Corneal Biomechanical Assessment
Devices may assess how the cornea deforms in response to an air impulse.
These measurements can add information but cannot guarantee that postoperative ectasia will not occur.
Dry-Eye and Eyelid Assessment
The surgeon should evaluate:
- Tear-film stability
- Corneal staining
- Meibomian glands
- Blepharitis
- Allergy
- Eyelid closure
- Contact lens-related inflammation
Pupil Size
Pupil measurements help guide counselling about:
- Night vision
- Halos
- Glare
- Optical-zone planning
Eye Pressure and Optic Nerve
Glaucoma or ocular hypertension should be identified before elective surgery.
Corneal laser surgery can affect the interpretation of future eye-pressure readings because it changes corneal thickness and biomechanics.
Natural-Lens Examination
Early cataract may cause:
- Glare
- Halos
- Myopic shifts
- Reduced contrast
- Fluctuating vision
Laser correction will not remove a cloudy natural lens.
Dilated Retinal Examination
This is particularly important in moderate and high myopia.
Laser surgery corrects the cornea but does not reduce:
- Retinal tear risk
- Retinal-detachment risk
- Myopic macular degeneration
- Myopic traction maculopathy
Why Might Two Surgeons Recommend Different Procedures?
Different recommendations do not necessarily mean that one surgeon is wrong.
Differences may reflect:
- Preferred safety margins
- Available technology
- Familiarity with a procedure
- Different interpretation of tomography
- Different enhancement strategies
- Different tolerance for borderline anatomy
- Different views on recovery and lifestyle priorities
However, a clinic that offers only one procedure may naturally recommend that procedure more often.
Patients should ask why the proposed procedure is safer than the alternatives for their specific measurements.
Does the Newest Laser Give the Best Result?
Not automatically.
Newer platforms may offer:
- Faster laser delivery
- Better eye tracking
- Improved docking
- Digital centration assistance
- Refined treatment profiles
- Improved workflow
However, technology cannot compensate for:
- Incorrect refraction
- Inappropriate patient selection
- Abnormal corneal anatomy
- Untreated dry eye
- Poor surgical technique
- Unrealistic expectations
The quality of screening and planning is often more important than the marketing name of the laser.
Is the Most Expensive Procedure the Best?
No.
Price may reflect:
- Equipment costs
- Disposable components
- Clinic overheads
- Surgeon experience
- Follow-up arrangements
- Branding
- Included enhancement policies
It does not prove that one procedure is safer for a particular patient.
Should You Choose the Procedure With the Fastest Recovery?
Recovery matters, but it should not override structural safety.
LASIK’s rapid recovery may be attractive for work or childcare.
However, a slower PRK recovery may be worthwhile when avoiding a flap provides a safer long-term option.
Similarly, SMILE may offer a useful balance between flap avoidance and relatively quick recovery for suitable myopic patients.
A Practical Decision Guide
Healthy Cornea, Low-to-Moderate Myopia, Fast Recovery Needed
LASIK or SMILE may both be suitable.
LASIK usually provides the fastest crisp vision.
SMILE avoids a flap and may cause less early dryness.
Contact-Sport Athlete
SMILE or PRK may be preferred because neither creates a hinged flap.
Mild Dry-Eye Risk
SMILE may be favoured, provided the ocular surface is adequately treated.
PRK may also be considered.
Severe dry eye may make all three unsuitable.
Relatively Thin but Regular Cornea
PRK may preserve more load-bearing tissue.
SMILE or thin-flap LASIK may sometimes remain possible, but the full structural assessment is more important than thickness alone.
Very High Myopia
ICL should be considered when laser would remove excessive corneal tissue.
Hyperopia or Mixed Astigmatism
LASIK or PRK usually offers a more established treatment pathway.
Irregular Corneal Shape or Keratoconus Risk
Routine laser vision correction may be unsafe.
Early Cataract
Cataract surgery may be more appropriate than corneal laser surgery.
Strong Need for Customised Corneal Treatment
Wavefront- or topography-guided LASIK or PRK may be preferred.
High Likelihood of Future Enhancement
LASIK generally offers the most straightforward early enhancement pathway.
Questions to Ask Before Choosing a Procedure
Useful questions include:
- Is my corneal tomography completely normal?
- How thick is my cornea?
- How much tissue will each procedure remove?
- What will my residual stromal thickness be?
- Do I have any ectasia risk factors?
- Is my eye surface healthy?
- Do I have meibomian gland dysfunction?
- How large are my pupils in dim lighting?
- Would wavefront- or topography-guided treatment benefit me?
- Why are you recommending this procedure over the alternatives?
- Is ICL safer for my prescription?
- What visual recovery should I expect?
- What are the enhancement options?
- What happens if I develop residual astigmatism?
- How will my eye pressure be monitored later?
- Will I still require reading glasses?
- What symptoms require urgent review?
Frequently Asked Questions
Which Laser Eye Surgery Has the Best Results?
LASIK, SMILE and PRK generally provide similar final visual outcomes in suitable myopic patients.
The best result depends more on correct patient selection and planning than on the procedure name.
Which Has the Fastest Recovery?
LASIK.
SMILE is usually next, while PRK has the slowest recovery.
Which Is the Least Painful?
LASIK generally causes the least early discomfort.
PRK is usually the most uncomfortable during the first few days.
Which Causes the Least Dry Eye?
SMILE generally causes less early dry-eye disturbance than LASIK.
Dry eye can still occur after any procedure.
Which Is Best for Contact Sports?
SMILE or PRK may be preferred because they avoid a hinged flap.
Which Is Best for a Thin Cornea?
PRK may be suitable when LASIK would remove too much load-bearing tissue.
A thin or abnormal cornea may be unsuitable for every corneal laser procedure.
Which Is Best for High Myopia?
ICL may be safer when the required laser correction would remove excessive corneal tissue.
Which Is Best for Astigmatism?
All three can correct regular myopic astigmatism.
LASIK and PRK may offer more wavefront- and topography-guided customisation.
Which Is Best for Hyperopia?
LASIK or PRK usually has a more established role.
Which Is Best After Age 40?
The choice depends on presbyopia and natural-lens clarity.
Early cataract may make cataract surgery more appropriate than laser correction.
Is SMILE Safer Than LASIK?
SMILE avoids flap complications and may reduce early dry-eye disturbance.
LASIK offers faster recovery, broader treatment flexibility and easier enhancement.
Neither is universally safer.
Is PRK Safer Than LASIK?
PRK avoids a flap and preserves more load-bearing stromal tissue.
It introduces more pain, slower healing and haze risk.
Is TransPRK Better Than PRK?
TransPRK automates epithelial removal but remains a surface-ablation procedure.
Its overall healing pattern and principal risks remain similar to PRK.
Is SMILE Pro Better Than Standard SMILE?
The newer platform may shorten laser time and improve workflow or digital guidance.
The suitability of the eye and quality of surgical planning remain more important than the platform name.
Can Laser Eye Surgery Be Reversed?
No.
LASIK, SMILE and PRK permanently remove corneal tissue.
Can Laser Eye Surgery Cause Blindness?
Severe permanent visual loss is rare but possible.
Potential causes include:
- Infection
- Severe corneal ectasia
- Scarring
- Irregular astigmatism
- Other uncommon complications
Will I Definitely Achieve 6/6 Vision?
No procedure can guarantee a particular result.
Outcome depends on:
- Preoperative visual potential
- Prescription accuracy
- Corneal health
- Retinal and optic nerve health
- Healing
- Residual refractive error
Can I Still Need Glasses?
Yes.
Glasses may still be required for:
- Residual prescription
- Night driving
- Fine visual tasks
- Reading after presbyopia
- Future prescription changes
Which Procedure Lasts the Longest?
All three permanently change the cornea.
No procedure prevents the eye from changing with age.
Long-term stability depends more on the prescription, age and eye biology than on a universal ranking of procedures.
Is Laser Eye Surgery Worth It?
It may be worthwhile when:
- The patient is suitable
- Expectations are realistic
- Dependence on glasses or contacts is meaningfully burdensome
- The expected benefit outweighs the procedure-specific risks
It is elective surgery, not an obligation.
Key Takeaway
There is no universally best laser eye surgery.
LASIK, SMILE and PRK can all provide excellent vision in properly selected patients.
LASIK generally offers:
- The fastest visual recovery
- Less early discomfort
- Broad prescription coverage
- Wavefront- and topography-guided options
- A relatively straightforward enhancement pathway
Its main limitation is the permanent corneal flap interface.
SMILE generally offers:
- No hinged corneal flap
- A small surface incision
- Less early corneal nerve disruption
- Potentially fewer early dry-eye effects
- Advantages for contact-sport patients
Its main limitations are a narrower established treatment range and less straightforward enhancement.
PRK generally offers:
- No flap
- Preservation of more load-bearing stromal tissue
- Suitability for some relatively thinner corneas
- Advantages when eye trauma is a concern
- Access to customised excimer-laser treatments
Its main limitations are greater pain, slower recovery and corneal haze risk.
The best choice depends on:
- Prescription
- Corneal shape and thickness
- Tissue calculations
- Dry-eye status
- Astigmatism
- Pupil size
- Age and presbyopia
- Natural-lens clarity
- Occupation
- Contact-sport participation
- Recovery priorities
- Need for future enhancement
Sometimes the best choice is not laser surgery.
An ICL, spectacles, contact lenses, cataract surgery or continued observation may provide a safer balance of benefits and risks.
The most important step is a comprehensive assessment that evaluates every suitable option rather than simply matching the patient to the laser available at the clinic.
References
- Ryan DS, et al. A Comparative Analysis of LASIK, SMILE and PRK: Patient-Reported Outcomes and Quality of Vision. 2025. PMID: 39641610.
- Taneri S, et al. Long-Term Outcomes of PRK, LASIK and SMILE. 2022. PMID: 34241701.
- Cui G, et al. Efficacy, Predictability and Safety of SMILE, Femtosecond LASIK and Transepithelial PRK for Myopia: A Meta-analysis. 2023. PMID: 36743675.
- Wei C, et al. Clinical Outcomes of SMILE and Wavefront-Guided LASIK for Myopia and Astigmatism: A Meta-analysis. 2024. PMID: 38377878.
- US Food and Drug Administration. VisuMax Femtosecond Laser SMILE Patient Information Booklet and Approved Indications.
- Shortt AJ, Allan BDS, Evans JR. LASIK Versus Photorefractive Keratectomy for Myopia. Cochrane Database of Systematic Reviews. 2013. PMID: 23440799.
- Castro-Luna G, et al. Ten-Year Safety and Effectiveness of Myopia Correction With PRK and Femtosecond LASIK. 2020.
- Chen KY, et al. Effectiveness of Keratorefractive Lenticule Extraction Compared With Femtosecond LASIK for Dry Eye: A Meta-analysis. 2025. PMID: 40778870.
- US Food and Drug Administration. LASIK Quality of Life Collaboration Project.
- Moshirfar M, et al. Ectasia After Corneal Refractive Surgery: A Systematic Review. 2021. PMID: 34417707.
- US Food and Drug Administration. LASIK Risks and Patient Expectations.
- US Food and Drug Administration. When Is LASIK Not for Me? LASIK Surgery Checklist.
- Ramirez-Miranda A, et al. Visual and Refractive Outcomes After SMILE Versus Femtosecond LASIK: A Paired-Eye Study. 2024. PMID: 39591576.
- Asif MI, et al. Complications of Small-Incision Lenticule Extraction. 2020.
- Somani SN, Moshirfar M, Patel BC. Photorefractive Keratectomy. Updated 2025. PMID: 31751077.
- Chang JY, et al. Comparison of Clinical Outcomes of LASIK, TransPRK and SMILE.
- US Food and Drug Administration. LASIK: Patient Information, Risks and Surgery Guidance.