Author: Dr Val Phua
Estimated reading time: 15 minutes
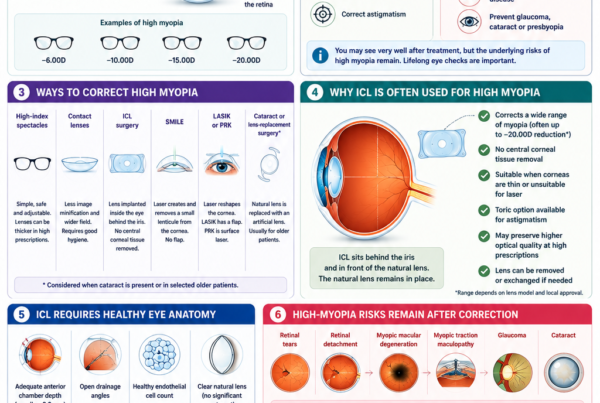
Toric Implantable Collamer Lens surgery, commonly called toric ICL surgery, corrects both short-sightedness and astigmatism by placing a specially designed corrective lens inside the eye.
The toric ICL is positioned behind the iris—the coloured part of the eye—and in front of the natural crystalline lens. It remains hidden from view and works with the eye’s natural focusing system to direct light more accurately onto the retina.
Unlike LASIK, PRK or SMILE, toric ICL surgery does not reshape the central cornea or remove corneal tissue. This makes it particularly useful for patients with moderate-to-very-high myopia, significant astigmatism, thin corneas or other features that make corneal laser treatment less suitable.
Modern EVO toric ICLs contain a small central opening that allows the eye’s natural fluid to circulate through the lens. This central-port design generally avoids the need for the preoperative peripheral iridotomy required with earlier ICL models. Clinical studies have reported high refractive accuracy, good unaided vision and stable correction with both spherical and toric EVO ICLs. [1–4]
However, toric ICL surgery is an operation inside the eye. Accurate measurement, careful lens sizing, precise axis alignment and long-term monitoring remain essential.
What Is a Toric ICL?
A toric ICL is a soft, foldable lens designed to correct:
- Myopia, or short-sightedness
- Regular astigmatism
- Myopia and astigmatism together
The term toric refers to a lens that has different optical powers in different directions.
A standard spherical ICL has the same correcting power in every meridian. It is mainly used to correct myopia.
A toric ICL incorporates:
- Spherical power to correct myopia
- Cylindrical power to correct astigmatism
- A specific axis along which the astigmatism correction must be aligned
This means a toric ICL must not only have the correct power and size—it must also be positioned at the correct rotational orientation inside the eye.
What Is Astigmatism?
Astigmatism occurs when the eye does not focus light equally in every direction.
In an eye without significant astigmatism, the central cornea is relatively symmetrical. In an astigmatic eye, the optical curvature differs between its principal meridians.
Instead of light converging to a single sharp point, different meridians may focus at different positions. This can cause:
- Blurred distance vision
- Blurred near vision
- Ghost images
- Shadowing around letters
- Distorted lines
- Eye strain
- Headaches
- Glare or difficulty driving at night
Astigmatism commonly originates from the cornea, although the natural lens can also contribute. FDA patient information explains that astigmatism causes light to focus at different points within the eye and that toric ICL correction can redirect the light more appropriately towards the retina. [2]
What Do Sphere, Cylinder and Axis Mean?
A spectacle prescription for myopic astigmatism commonly includes three measurements.
Sphere
The sphere indicates the amount of short-sightedness or long-sightedness.
For example:
- −3.00 D indicates myopia
- −8.00 D indicates a higher degree of myopia
Cylinder
The cylinder indicates the amount of astigmatism.
For example:
- −1.00 D of cylinder represents one dioptre of astigmatism
- −3.00 D represents a greater degree of astigmatism
Axis
The axis describes the orientation of the astigmatism, expressed between 1 and 180 degrees.
The axis does not describe the severity of astigmatism. It tells the surgeon how the cylindrical correction must be oriented.
A toric ICL is selected and positioned according to all three components.
How Does a Toric ICL Correct Vision?
The toric ICL contains different optical powers along perpendicular meridians.
The spherical component corrects the overall myopic error, while the toric component neutralises the difference in focusing power between the principal astigmatic meridians.
For the correction to work accurately, the toric component must be aligned with the intended axis inside the eye.
When the lens has the correct:
- Spherical power
- Cylinder power
- Axis
- Physical size
- Position and vault
light can be focused more accurately on the retina.
Where Is the Toric ICL Placed?
The lens is implanted:
- Behind the iris
- In front of the natural crystalline lens
- Within the posterior chamber of the eye
The natural lens is not removed.
The toric ICL is therefore different from the artificial lens used during cataract surgery. Cataract surgery removes the natural lens, whereas toric ICL surgery adds a corrective lens while retaining it.
The lens is transparent and normally cannot be seen by other people once it has been implanted. [1,2]
What Is the Difference Between a Spherical ICL and a Toric ICL?
Spherical ICL
A spherical ICL primarily corrects myopia.
It may be suitable when:
- Astigmatism is minimal
- The remaining astigmatism is unlikely to affect vision significantly
- Corneal or incisional correction is planned separately
- The astigmatism is not appropriate for a toric lens
Toric ICL
A toric ICL corrects myopia together with regular astigmatism.
It may reduce the need for:
- Astigmatic spectacles
- Toric contact lenses
- Additional corneal laser treatment
- Separate astigmatic incisions
The appropriate option depends on the amount, source and regularity of the astigmatism.
Why Is Axis Alignment Important?
A toric lens only provides its intended astigmatism correction when it is aligned at the correct axis.
If the toric ICL rotates away from the planned position:
- The effective cylinder correction is reduced
- Residual astigmatism develops
- Vision may become blurred or distorted
- Ghosting may occur
- Night-time visual quality may worsen
The greater the rotation, the greater the potential loss of astigmatism correction.
Published long-term studies have generally found good rotational stability after toric ICL implantation. However, measurable rotation can occur, and a small number of patients may require surgical repositioning. [6–8]
How Is the Correct Axis Determined?
The surgeon uses several measurements to plan the axis.
These may include:
- Manifest refraction
- Cycloplegic refraction
- Corneal topography
- Corneal tomography
- Keratometry
- Anterior-segment imaging
- Digital iris or limbal registration
- Assessment of cyclotorsion
What Is Cyclotorsion?
Cyclotorsion refers to rotation of the eye around its visual axis.
The eye may rotate slightly when a patient changes from sitting upright during preoperative measurements to lying flat during surgery.
If this change is not accounted for, the toric lens may not be aligned exactly as planned.
The surgeon may use:
- Manual corneal markings
- Digital image-guided marking
- Intraoperative registration
- Postoperative photography or aberrometry
A recent comparison found both manual and digital marking capable of producing effective toric phakic-lens alignment, although digital systems may improve workflow and documentation in some settings. [12]
Can a Toric ICL Rotate After Surgery?
Yes, although major rotation is uncommon.
Possible contributing factors include:
- The relationship between ICL size and internal eye dimensions
- The shape of the ciliary sulcus
- Lens orientation
- Vault
- Natural movement during early healing
- Trauma
- Individual anatomical variation
Rotation may occur:
- During the operation
- Within the first few postoperative days
- During the early healing period
- Less commonly, later after surgery
Studies assessing EVO toric ICLs have generally reported stable long-term alignment, but individual variation remains. Research is continuing into imaging and artificial-intelligence models that may help predict postoperative rotation more accurately. [7,8,19]
What Symptoms Can Toric ICL Rotation Cause?
Possible symptoms include:
- Blurred distance vision
- Ghosting or double outlines
- Shadowing around text
- Reduced clarity at night
- Glare or halos
- A return of astigmatic blur
- One eye seeing less clearly than the other
- Vision that initially improves but subsequently becomes less sharp
Small rotational changes may not produce noticeable symptoms, especially when the lens cylinder is low.
A larger rotation or a high-powered toric lens may have a greater effect.
How Is Toric ICL Rotation Diagnosed?
Assessment may include:
- Unaided visual acuity
- Manifest refraction
- Measurement of residual astigmatism
- Slit-lamp examination
- Dilated examination of the toric marks
- Anterior-segment photography
- Wavefront aberrometry
- Digital rotational analysis
- Comparison with the planned axis
It is important to distinguish lens rotation from other causes of postoperative blur, such as:
- Dry eye
- Residual spherical error
- Corneal astigmatism
- Incorrect lens power
- Cataract
- Macular or retinal disease
- Temporary postoperative inflammation
What Happens if the Toric ICL Rotates?
Management depends on the degree of rotation and the effect on vision.
Observation
Observation may be appropriate when:
- Rotation is small
- Unaided vision remains good
- Residual cylinder is minimal
- The patient is not troubled by symptoms
Spectacle Correction
A small residual cylinder may be corrected with glasses, particularly for driving or fine visual tasks.
Surgical Repositioning
The lens can be rotated back to the intended axis when:
- Residual astigmatism is significant
- Vision is functionally affected
- The axis is clearly misaligned
- The expected improvement justifies another operation
Lens Exchange
Exchange may be considered when:
- The selected power is incorrect
- The lens repeatedly rotates
- The physical size is unsuitable
- The vault is inappropriate
- Repositioning alone is unlikely to solve the problem
Corneal Laser Enhancement
PRK or LASIK may occasionally be considered for a stable residual prescription when the cornea is suitable.
This requires a separate assessment and should not be assumed before the initial surgery.
Who May Be Suitable for a Toric ICL?
A suitable candidate typically has:
- Stable myopia
- Regular astigmatism
- A prescription within the available toric ICL range
- Adequate anterior chamber depth
- Open drainage angles
- A healthy endothelial cell count
- A clear natural lens
- Acceptable eye pressure
- No active eye infection or inflammation
- Adequate retinal and optic nerve health
- Realistic expectations
- Willingness to attend long-term follow-up
Is Toric ICL Only for High Myopia?
No.
Toric ICL has traditionally been associated with moderate-to-high myopia and astigmatism, but it can also be considered for selected lower prescriptions when there is a meaningful reason to avoid corneal laser treatment.
Examples include:
- Thin corneas
- Corneal laser unsuitability
- Significant dry-eye concerns
- Previous corneal refractive surgery
- A desire to preserve central corneal tissue
- A lifestyle in which avoiding corneal ablation is beneficial
Nevertheless, the ability to correct a prescription with a toric ICL does not automatically mean that intraocular surgery is the preferred choice.
The potential benefits must be weighed against the additional risks of an implant inside the eye.
What Astigmatism Range Can a Toric ICL Correct?
The available range depends on:
- The lens model
- Local regulatory approval
- Available lens powers
- The patient’s myopia
- The type of astigmatism
- The surgeon’s planning method
Under United States FDA labelling, the EVO toric ICL is approved for patients with myopia and 1.00 to 4.00 D of astigmatism. Safety and effectiveness outside those parameters have not been established under that particular approval. Treatment ranges may differ in Singapore and other countries. [1,2]
Very low astigmatism may not require a toric lens.
Very high astigmatism may require:
- Partial toric ICL correction
- Additional spectacle correction
- A corneal laser enhancement
- Astigmatic corneal incisions
- Another customised strategy
What Type of Astigmatism Can a Toric ICL Correct?
Toric ICLs are designed mainly for regular astigmatism.
Regular Astigmatism
Regular astigmatism has two principal meridians that are approximately perpendicular to each other.
This commonly includes:
- With-the-rule astigmatism
- Against-the-rule astigmatism
- Oblique astigmatism
Regular astigmatism can usually be represented reliably by a cylinder power and axis.
Irregular Astigmatism
Irregular astigmatism does not form two simple, perpendicular principal meridians.
Possible causes include:
- Keratoconus
- Corneal scarring
- Previous corneal infection
- Previous eye trauma
- Corneal transplantation
- Post-laser corneal ectasia
- Irregular corneal surgery
A toric ICL may reduce the regular component of the prescription but may not correct irregular optical distortion.
Patients with irregular astigmatism may still need:
- Rigid gas-permeable lenses
- Scleral lenses
- Spectacles
- Corneal cross-linking
- Corneal surgery
- Other specialised treatment
Can Toric ICL Be Used in Keratoconus?
Possibly, but only in selected cases.
A toric ICL does not treat or stabilise keratoconus.
It may be considered when:
- The keratoconus is stable
- There is no evidence of progression
- Corneal cross-linking has been completed when required
- The remaining prescription is predominantly regular
- Contact lenses are poorly tolerated
- The internal eye anatomy is suitable
- The patient understands that irregular distortion may remain
Published studies have reported useful refractive outcomes in selected stable keratoconus patients, but lens rotation, residual astigmatism and the continuing need for corneal monitoring remain important considerations.
Can Toric ICL Be Used for Thin Corneas?
Potentially, yes.
Because the toric ICL does not remove central corneal tissue, corneal thickness does not limit the optical correction in the same way it may limit LASIK, PRK or SMILE.
However, a thin cornea must still be investigated properly.
Corneal topography and tomography are needed to determine whether the cornea is:
- Naturally thin but normal
- Affected by keratoconus
- Structurally unstable
- Scarred
- Previously treated with laser surgery
Toric ICL corrects the refractive error but does not strengthen an unstable cornea.
Can Toric ICL Be Used if You Have Dry Eyes?
Many patients with dry-eye concerns may be suitable.
Toric ICL causes less central corneal nerve disruption than LASIK and does not require removal of a corneal lenticule as in SMILE.
However, it does not cure dry eye.
Temporary symptoms can still occur because of:
- The corneal incision
- Surgical antiseptic
- Postoperative eyedrops
- Preservatives
- Reduced blinking
- Pre-existing blepharitis
- Meibomian gland dysfunction
Dry eye, blepharitis and allergic eye disease should be treated before surgery.
Who May Not Be Suitable for Toric ICL?
Toric ICL surgery may be unsuitable when there is:
- An unstable spectacle prescription
- Irregular astigmatism that cannot be corrected adequately
- A shallow anterior chamber
- Narrow drainage angles
- An inadequate endothelial cell count
- Significant cataract
- Moderate or advanced glaucoma
- Ocular hypertension requiring further investigation
- Active uveitis
- Active eye infection
- Progressive keratoconus
- Pregnancy or breastfeeding
- Vision-limiting retinal or optic nerve disease
- Unrealistic expectations
- Inability to attend long-term follow-up
FDA labelling also identifies several conditions in which safety and effectiveness have not been established, including unstable myopia, glaucoma or ocular hypertension, pigment dispersion, pseudoexfoliation and a history of uveitis. [2]
What Tests Are Needed Before Toric ICL Surgery?
Accurate measurements are especially important because both the spherical and astigmatic correction must be planned.
Refraction and Visual Acuity
The surgeon measures:
- Sphere
- Cylinder
- Axis
- Unaided vision
- Best-corrected vision
- Prescription stability
Repeated measurements may be needed to confirm that the cylinder and axis are consistent.
Cycloplegic Refraction
Cycloplegic drops temporarily relax the focusing muscles.
This may help identify:
- Accommodation-related measurement changes
- Over-minus prescriptions
- Latent refractive error
- Unstable measurements in younger patients
Corneal Topography and Tomography
These scans assess:
- Corneal curvature
- The magnitude and axis of corneal astigmatism
- Corneal thickness
- Regularity of the astigmatism
- Keratoconus
- Corneal scarring
- Previous laser treatment
The surgeon compares corneal measurements with the manifest refraction to determine how much astigmatism originates from the cornea and how much may arise internally.
Anterior Chamber Depth
The space between the corneal endothelium and natural lens must be sufficient to accommodate the ICL safely.
Drainage-Angle Assessment
Gonioscopy or anterior-segment imaging evaluates whether the drainage angles are sufficiently open.
Internal Eye Measurements
Measurements may include:
- White-to-white corneal diameter
- Sulcus-to-sulcus dimensions
- Anterior chamber width
- Crystalline lens rise
- Lens thickness
- Pupil diameter
These measurements help determine the physical size and expected vault of the ICL.
Endothelial Cell Count
Specular microscopy measures the corneal endothelial cells.
These cells help keep the cornea transparent and have limited regenerative ability.
An adequate age-adjusted endothelial reserve is required before surgery.
Eye Pressure and Optic Nerve Assessment
The surgeon checks for:
- Ocular hypertension
- Glaucoma
- Narrow angles
- Pigment dispersion
- Optic nerve damage
Natural-Lens Examination
The natural lens is examined for cataract or other abnormalities.
Dilated Retinal Examination
This is especially important in high myopia.
The examination looks for:
- Retinal holes
- Retinal tears
- Lattice degeneration
- Retinal detachment
- Myopic macular changes
- Other peripheral retinal abnormalities
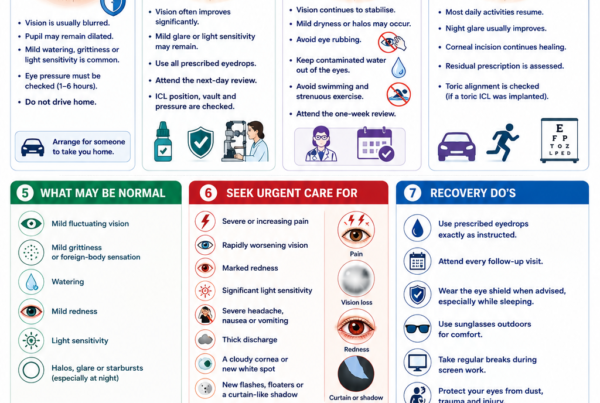
Pupil Measurement
Large pupils may increase awareness of:
- Glare
- Halos
- Starbursts
- Night-driving symptoms
How Is the Toric ICL Power Calculated?
The calculation includes:
- Manifest sphere
- Manifest cylinder
- Cylinder axis
- Corneal-plane conversion
- The expected position of the lens inside the eye
- Incision-induced astigmatism
- Lens model and available powers
- The surgeon’s intended axis
The ICL is positioned closer to the natural lens than spectacles or contact lenses. The required power therefore cannot be selected simply by copying the spectacle prescription.
High prescriptions require appropriate vertex-distance conversion.
What Happens During Toric ICL Surgery?
Toric ICL surgery is generally performed as a day procedure.
Before Surgery
The eye may be prepared with:
- Pupil-dilating drops
- Anaesthetic eyedrops
- Antiseptic cleaning
- Axis markings or digital registration
- Antibiotic or anti-inflammatory medication
During Surgery
The surgeon generally:
- Makes a small incision at the edge of the cornea.
- Inserts the folded toric ICL through the incision.
- Allows the lens to unfold inside the eye.
- Places its supporting footplates behind the iris.
- Rotates the lens to the planned axis.
- Removes surgical viscoelastic as required.
- Checks the lens position, pupil and wound.
- Confirms the axis and vault.
The incision is normally self-sealing and usually does not require stitches.
How Long Does Surgery Take?
The operating time varies, but uncomplicated implantation is often completed in approximately 20 to 30 minutes or less per eye.
Additional time may be required when:
- Astigmatic alignment is complex
- The anatomy is unusual
- The lens requires further manipulation
- Both eyes are treated during the same session
Is Toric ICL Surgery Painful?
The eye is numbed with anaesthetic medication.
Patients may notice:
- Bright lights
- Movement
- Mild pressure
- Water around the eye
- Temporary blurring
Sharp pain is not expected.
Mild grittiness, watering or light sensitivity may occur afterwards.
Severe or increasing pain requires urgent assessment.
What Is Vault?
Vault is the space between the back surface of the ICL and the front surface of the natural lens.
An appropriate vault helps maintain safe separation between the ICL, natural lens, iris and drainage structures.
If the Vault Is Too Low
A low vault may increase concern about:
- ICL contact with the natural lens
- Anterior subcapsular lens opacity
- Cataract formation
- Reduced fluid circulation
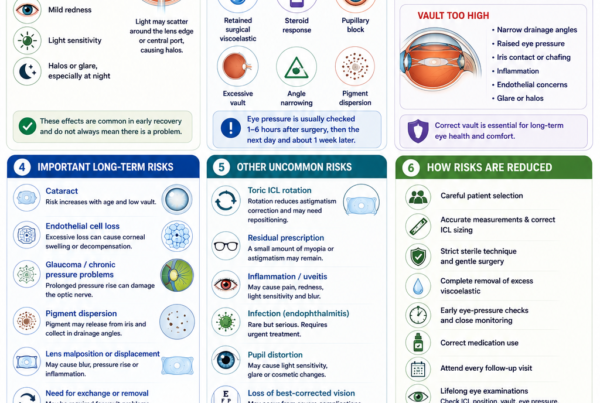
If the Vault Is Too High
A high vault may contribute to:
- Narrowing of the drainage angle
- Raised eye pressure
- Iris contact
- Pigment dispersion
- Inflammation
- Glare or optical symptoms
An unsuitable vault may require observation, pressure treatment, repositioning, lens exchange or removal.
Vault-related concerns are among the recognised reasons for ICL exchange or explantation. [14,17]
What Is Recovery Like?
Many patients notice a substantial improvement in vision by the following day.
Vision may initially fluctuate because of:
- Dilated pupils
- Mild inflammation
- Corneal incision swelling
- Tear-film disturbance
- Temporary eye-pressure changes
- Residual medication
- Neural adaptation
The eye pressure is usually checked shortly after surgery or during the early postoperative period.
Follow-up commonly includes:
- A review within the first day
- A review during the first week
- Further reviews during the first month
- Longer-term monitoring
The precise schedule depends on the surgeon and clinical findings.
What Restrictions Are Needed After Surgery?
Patients are generally advised to:
- Use prescribed eyedrops exactly as instructed
- Avoid rubbing or pressing the eyes
- Keep contaminated water away from the eyes initially
- Avoid swimming and hot tubs until permitted
- Avoid eye makeup during early healing
- Avoid strenuous exercise for the advised period
- Avoid contact sports until cleared
- Use an eye shield when advised
- Attend all follow-up appointments
Driving should resume only when vision meets the legal standard and the surgeon considers it safe.
What Results Can Patients Expect?
Studies of toric ICL implantation have generally reported:
- Effective correction of myopia
- Substantial reduction in astigmatism
- High refractive predictability
- Good unaided distance vision
- Good preservation of corrected vision
- Stable outcomes in most patients
The original United States toric ICL clinical study supported the efficacy and predictability of the lens for moderate-to-high myopic astigmatism. More recent central-port toric ICL studies have continued to report good refractive accuracy, rotational stability and long-term astigmatic correction. [3–8]
No operation can guarantee an exact zero prescription.
A small amount of residual myopia or astigmatism may remain.
Can Toric ICL Improve Vision Beyond Glasses?
Some highly myopic patients gain lines of best-corrected visual acuity after ICL surgery.
Possible reasons include:
- Reduced spectacle minification
- A larger retinal image
- Less peripheral distortion
- More effective correction of high astigmatism
- Improved optical quality
However, surgery cannot overcome vision limited by:
- Amblyopia
- Myopic macular degeneration
- Retinal scarring
- Optic nerve damage
- Irregular corneal disease
- Cataract
- Previous retinal detachment
The best spectacle- or contact-lens-corrected vision before surgery gives an indication of the eye’s visual potential.
Can Toric ICL Cause Glare or Halos?
Yes.
Possible symptoms include:
- Halos around lights
- Glare
- Starbursts
- Light scatter
- Ghost images
- Difficulty driving at night
Potential contributing factors include:
- Pupil size
- The central port
- Residual refractive error
- Toric misalignment
- ICL position
- Vault
- Early inflammation
- Dry eye
- Neural adaptation
Many symptoms improve over time. Long-term research suggests that glare often becomes less troublesome as patients adapt, although a small number continue to notice symptoms during night driving.
What Are the Main Risks of Toric ICL Surgery?
Toric ICL Rotation
Rotation can reduce astigmatism correction and may require repositioning or exchange.
Residual Myopia or Astigmatism
A residual prescription may result from:
- Measurement variation
- Lens-power limitations
- Axis misalignment
- Lens rotation
- Incision-induced astigmatism
- Healing
- Future refractive change
Incorrect Vault
A lens that sits too close to or too far from the natural lens may affect eye pressure, drainage-angle anatomy or cataract risk.
Raised Eye Pressure
Possible causes include:
- Retained surgical viscoelastic
- Steroid response
- Inflammation
- Excessive vault
- Angle narrowing
- Pupillary block
- Pigment dispersion
Eye-pressure complications require prompt identification and treatment. [14]
Cataract
The natural lens remains inside the eye and can develop cataract with age.
Additional risk may arise from:
- Low vault
- Proximity between the ICL and natural lens
- Surgical contact with the natural lens
- Increasing age
- Individual anatomy
Modern central-port ICL studies have reported favourable long-term outcomes, but cataract risk cannot be eliminated. [15]
Endothelial Cell Loss
The corneal endothelial cells keep the cornea clear.
Long-term monitoring is recommended because excessive cell loss could eventually contribute to corneal swelling.
Inflammation
Mild postoperative inflammation is expected.
Persistent or severe inflammation may require additional treatment and investigation.
Infection
Endophthalmitis is a rare but potentially sight-threatening infection inside the eye.
Warning symptoms include:
- Increasing pain
- Increasing redness
- Rapidly worsening vision
- Marked light sensitivity
- Eyelid swelling
- Increasing discharge
Urgent treatment is required.
Pigment Dispersion
Contact between the ICL and the back of the iris may release pigment.
In rare cases, pigment accumulation within the drainage angle may contribute to increased eye pressure or glaucoma. Long-term monitoring of the angle, pressure and optic nerve remains important.
Retinal Tear or Detachment
Many toric ICL patients have high myopia and therefore already have an increased lifetime risk of retinal tears and detachment.
The ICL corrects the refractive error but does not shorten the elongated eye or remove these retinal risks.
Long-term comparative studies have not found clear evidence that central-port ICL implantation itself increases retinal-detachment prevalence beyond the underlying risk from high myopia. Nevertheless, retinal detachment can still occur. [16]
Toric ICL vs LASIK for Astigmatism
Both procedures can correct myopic astigmatism.
Potential Advantages of Toric ICL
- No central corneal tissue removal
- No corneal flap
- Corrects a wide range of myopia
- Suitable for some thin corneas
- May induce fewer corneal higher-order aberrations
- May preserve better contrast sensitivity at high prescriptions
- Lens can be removed or exchanged
Potential Advantages of LASIK
- No implant remains inside the eye
- Avoids intraocular surgery
- Rapid visual recovery
- No vault or lens-rotation concerns
- Less implant-specific long-term monitoring
- Usually lower cost
Systematic reviews have found both LASIK and toric ICL effective for myopic astigmatism. Some evidence favours toric ICL for preservation of corrected vision, contrast sensitivity and higher-order aberrations in moderate-to-high myopia, but LASIK avoids the risks associated with an intraocular implant. [10]
Toric ICL vs SMILE for Astigmatism
Potential Advantages of Toric ICL
- No removal of central corneal tissue
- Treats a wide range of myopia
- Potentially better optical quality at high prescriptions
- Less dependence on corneal thickness
- Removable or exchangeable lens
Potential Advantages of SMILE
- No implant inside the eye
- No LASIK flap
- Small corneal incision
- Avoids vault, cataract and implant-rotation risks
- Less implant-specific long-term monitoring
Comparative studies have found both toric ICL and SMILE effective for myopic astigmatism. Some research suggests slightly more consistent axis and astigmatic correction with toric ICL in selected groups, while SMILE avoids the risks of intraocular surgery. [11,19]
Is Toric ICL Better Than a Spherical ICL With Laser Enhancement?
There is no single answer.
Toric ICL Alone
Advantages may include:
- One primary refractive procedure
- No planned corneal ablation
- Preservation of corneal tissue
- Direct correction of cylinder inside the eye
Limitations include:
- Dependence on rotational stability
- Available cylinder powers
- Possible need for repositioning
Spherical ICL Followed by Laser Enhancement
This may be considered when:
- The cylinder is outside the toric lens range
- The cornea is suitable for a small enhancement
- A very precise residual correction is desired
- The surgeon prefers a staged bioptics strategy
Limitations include:
- Two procedures
- Additional cost and recovery
- Corneal tissue removal
- Laser-related dry-eye and corneal risks
The preferred approach depends on the prescription, cornea, expected residual error and patient priorities.
Does Toric ICL Correct Presbyopia?
No.
A standard toric ICL corrects myopia and astigmatism but does not prevent the age-related loss of near focusing ability.
Patients approaching or over 40 may still require:
- Reading glasses
- Progressive lenses
- A monovision strategy
- Another presbyopia-management option
A myopic patient who currently reads by removing their glasses may lose that unaided near vision when both eyes are corrected for distance.
Can Toric ICL Be Used After Age 40?
Possibly.
Published studies have reported satisfactory long-term visual quality and manageable rotational stability in selected patients over 40. However, suitability requires careful consideration of:
- Presbyopia
- Early cataract
- Natural-lens thickness
- Anterior chamber space
- Endothelial cell reserve
- Expected time before cataract surgery
- Near-vision expectations
A patient with early cataract may be better served by cataract surgery rather than toric ICL implantation. [9]
What Happens if Cataract Develops Later?
When a visually significant cataract develops:
- The toric ICL is usually removed.
- The cloudy natural lens is removed.
- A cataract intraocular lens is implanted.
The cataract lens may itself be toric if significant corneal astigmatism remains.
Previous toric ICL surgery does not normally prevent cataract surgery, but the cataract surgeon should know:
- The previous ICL power
- The previous toric axis
- Preoperative refraction
- Corneal measurements
- Retinal status
- Whether any previous laser enhancement was performed
Does Toric ICL Cure High Myopia?
No.
It corrects the optical blur caused by myopia and astigmatism.
It does not:
- Shorten the eyeball
- Reverse retinal stretching
- Prevent retinal detachment
- Prevent myopic macular degeneration
- Prevent glaucoma
- Prevent cataract
- Prevent presbyopia
Highly myopic patients still require regular retinal, macular and optic nerve examinations.
When Should You Seek Urgent Care After Surgery?
Seek urgent assessment for:
- Severe or increasing eye pain
- Rapidly worsening vision
- Marked redness
- Significant light sensitivity
- Severe headache
- Nausea or vomiting with eye pain
- Increasing discharge
- A distorted or non-reactive pupil
- A new white or grey spot on the cornea
- New flashes or floaters
- A curtain-like shadow across the vision
- Significant trauma to the eye
Do not wait for the next scheduled review if symptoms are worsening rapidly.
Frequently Asked Questions About Toric ICL
Is Toric ICL the Same as EVO ICL?
EVO refers to a modern central-port ICL design.
EVO is available in spherical and toric versions. The toric model corrects myopia together with astigmatism.
Can Toric ICL Correct Both Myopia and Astigmatism?
Yes.
The spherical component corrects myopia, while the cylinder component corrects regular astigmatism.
How Much Astigmatism Can Toric ICL Correct?
This depends on the model, available lens powers and local regulatory approval.
Under current United States labelling, EVO toric ICL is approved for 1.00 to 4.00 D of astigmatism. Other markets may have different ranges. [1,2]
Can Toric ICL Correct Irregular Astigmatism?
It can correct a regular refractive component but may not eliminate irregular distortion caused by keratoconus, scarring or corneal ectasia.
Rigid or scleral contact lenses may still be needed for the best optical quality.
How Long Does a Toric ICL Last?
The lens is designed to remain inside the eye long term.
It does not have a routine expiry date after implantation.
It may require removal or exchange if cataract, pressure problems, unsuitable vault, rotation or another complication develops.
Can You Feel the Toric ICL?
Normally not.
The lens is located behind the iris and should not produce a sensation after the eye has healed.
Can Other People See It?
Usually not.
It is transparent and hidden behind the iris.
Can the Lens Rotate?
Yes, although major rotation is uncommon.
If significant rotation causes residual astigmatism or blurred vision, surgical repositioning may be required.
Can the Lens Rotate Again After Repositioning?
It is possible.
Repeated rotation may raise concern about:
- Lens sizing
- Internal eye shape
- Vault
- The chosen orientation
Lens exchange may be considered if repeated repositioning does not provide stable alignment.
Is Toric ICL Reversible?
The lens can usually be removed or exchanged.
However, removal requires another intraocular operation. It is more accurate to call it removable rather than completely reversible.
Will I Need Glasses After Surgery?
Possibly.
Glasses may still be needed for:
- Reading
- Night driving
- Fine visual tasks
- A small residual prescription
- Future refractive changes
Can Toric ICL Correct Astigmatism After LASIK or SMILE?
Potentially.
It may be considered when:
- Significant myopia and astigmatism remain
- Further corneal tissue removal is undesirable
- The cornea is stable
- The natural lens is clear
- Internal eye dimensions are suitable
The cause of the residual astigmatism must first be determined.
Is Toric ICL Better Than LASIK?
Toric ICL may be advantageous for high myopia, thin corneas or when preservation of corneal tissue is important.
LASIK avoids intraocular surgery and implant-related risks.
The better choice depends on the individual eye.
Is Toric ICL Better Than SMILE?
Toric ICL may provide advantages in high myopia, corneal tissue preservation and certain visual-quality measurements.
SMILE avoids an intraocular implant, vault issues, cataract risk related to the ICL and toric-lens rotation.
Does Toric ICL Prevent Retinal Detachment?
No.
The underlying retinal risk associated with high myopia remains.
Do I Need Lifelong Follow-Up?
Regular long-term eye examinations are recommended.
Follow-up may include:
- Vision and refraction
- Toric-axis alignment
- ICL position
- Vault
- Eye pressure
- Drainage-angle examination
- Endothelial cell count
- Natural-lens examination
- Retinal and macular examination
Key Takeaway
A toric ICL is a corrective lens implanted behind the iris to treat myopia and regular astigmatism.
It may be particularly useful for patients with:
- Moderate-to-very-high myopia
- Significant regular astigmatism
- Thin or laser-unsuitable corneas
- Dry-eye concerns
- A desire to preserve central corneal tissue
The toric lens must be aligned accurately with the intended astigmatic axis. Most lenses remain sufficiently stable, but rotation can reduce the astigmatism correction and may occasionally require surgical repositioning or exchange.
Like all ICL procedures, toric ICL surgery carries risks involving:
- Eye pressure
- Vault
- Cataract
- Endothelial cells
- Inflammation
- Infection
- Residual prescription
- Lens rotation
A detailed assessment of the prescription, cornea, internal eye anatomy, natural lens, eye pressure and retina is essential before deciding whether toric ICL is the most appropriate form of vision correction.
References
- US Food and Drug Administration. EVO/EVO+ Visian Implantable Collamer Lens: Recently Approved Device. 2022.
- US Food and Drug Administration. EVO and EVO+ Visian Implantable Collamer Lens Patient Information Booklet and Instructions for Use. 2022.
- Packer M, et al. Evaluation of the EVO/EVO+ Sphere and Toric Visian Implantable Collamer Lens. 2022.
- Parkhurst G, et al. Three-Year Results From the United States FDA Prospective Multicentre Clinical Study of the EVO ICL. 2025.
- Sanders DR, et al. Toric Implantable Collamer Lens for Moderate-to-High Myopic Astigmatism. 2007.
- Shiga S, et al. Long-Term Clinical Outcomes After Toric Implantable Collamer Lens Implantation. 2023.
- Chen X, et al. Effect of Long-Term Rotation on Astigmatism Following EVO Toric Implantable Collamer Lens Implantation. 2023.
- Cano-Ortiz A, et al. Objective Rotational Analysis of EVO Toric ICLs Using Infrared Retinal Retroillumination Photography. 2025.
- Ye Y, et al. Long-Term Visual Quality and Rotational Stability After ICL and Toric ICL Implantation in Patients Older Than 40 Years. 2024.
- Goes S, et al. Posterior Chamber Toric Implantable Collamer Lenses Versus LASIK for Myopic Astigmatism: A Systematic Review. 2022.
- Ganesh S, et al. Matched-Population Comparison of Toric ICL, SMILE and Femtosecond LASIK for Myopic Astigmatism. 2017.
- List W, et al. Digital Versus Manual Axis Marking for Toric Phakic Intraocular Lens Implantation. 2025.
- Carreras-Díaz H, et al. Refractive Outcomes After V4c Toric Collamer Lens Implantation: Vector Analysis. 2024.
- Gong D, et al. Causes and Management Strategies for Elevated Intraocular Pressure After Implantable Collamer Lens Implantation. 2024.
- Alfonso-Bartolozzi B, et al. Ten-Year Follow-up of Posterior Chamber Phakic Intraocular Lenses With Central-Port Design. 2024.
- Xu W, et al. Long-Term Outcomes of Retinal Detachment in Phakic Eyes After ICL Implantation. 2020.
- AlSabaani NA, et al. Causes of Phakic Implantable Collamer Lens Explantation or Exchange. 2016.
- Brar S, et al. Visual and Refractive Outcomes With Toric Phakic Intraocular Lenses for High Myopic Astigmatism. 2021.
- Assaf A, et al. Comparative Analysis of SMILE and Toric ICL for Myopic Oblique Astigmatism. 2026.
- Jiang Y, et al. Artificial-Intelligence Prediction of Postoperative Toric ICL Rotation and Its Effect on Refraction and Vision. 2025.