Author: Dr Val Phua
Estimated reading time: 13–15 minutes
What Is Eye Pressure?
Eye pressure, medically called intraocular pressure or IOP, is the pressure inside the eyeball.
The eye is a closed, fluid-filled structure. A certain amount of internal pressure helps it:
- Maintain its shape
- Keep its optical surfaces appropriately positioned
- Support normal eye function
- Allow fluid to circulate through the front of the eye
Eye pressure is most closely influenced by the clear fluid called aqueous humour, which circulates through the front portion of the eye.
The pressure is measured in millimetres of mercury, abbreviated as mmHg.
Eye pressure is an important part of glaucoma assessment, but it is not the same thing as glaucoma.
A person may have:
- High pressure without optic-nerve damage
- Glaucoma despite pressure readings within the usual population range
- Pressure that varies significantly at different times
- A pressure reading affected by corneal thickness or previous eye surgery
The National Eye Institute explains that pressure above 21 mmHg is statistically higher than normal for most people, but not everyone with elevated pressure develops glaucoma, and some people develop glaucoma at apparently normal pressure levels.
Where Does Eye Pressure Come From?
The eye continuously produces and drains aqueous humour.
The process involves several structures:
- The ciliary body produces aqueous fluid behind the iris.
- The fluid flows through the pupil.
- It enters the anterior chamber between the cornea and iris.
- Most of it drains through the trabecular meshwork.
- It then passes into Schlemm’s canal and the bloodstream.
- A smaller amount leaves through the uveoscleral pathway.
Eye pressure depends largely on the balance between:
- The amount of aqueous fluid being produced
- The resistance to fluid leaving the eye
When drainage becomes less efficient, pressure may rise even though fluid production remains normal.
Is Eye Pressure the Same as Blood Pressure?
No.
Eye pressure and blood pressure are measured differently and represent different physiological systems.
Blood pressure describes pressure within the body’s blood vessels.
Eye pressure describes pressure within the eyeball.
A person can have:
- Normal blood pressure and high eye pressure
- High blood pressure and normal eye pressure
- Low blood pressure and glaucoma
- Normal eye pressure but an optic nerve vulnerable to reduced blood flow
Although vascular health may influence the optic nerve, blood-pressure medication should never be adjusted solely to change eye pressure without consultation with the prescribing physician.
What Is Considered a Normal Eye Pressure?
A commonly quoted statistical range is approximately 10 to 21 mmHg.
However, this range should not be interpreted as:
- Below 21 means completely safe
- Above 21 means definite glaucoma
- Every person should have the same target
- One reading is sufficient to judge risk
The upper figure of 21 mmHg was derived from the distribution of pressure in the general population. It is a statistical reference rather than a biological dividing line between healthy and diseased eyes.
A pressure of 22 mmHg may be acceptable in one healthy eye but too high for another eye with advanced glaucoma.
Likewise, a pressure of 15 mmHg may be satisfactory for one patient but insufficiently low for someone whose glaucoma is continuing to progress.
Is a Pressure of 22 or 23 Automatically Dangerous?
No.
A mildly elevated reading should be interpreted in context.
The clinician may consider:
- Whether the reading is repeatable
- Which instrument was used
- Central corneal thickness
- Corneal shape and biomechanics
- Optic-nerve appearance
- OCT findings
- Visual-field results
- Family history
- Age
- Degree of myopia
- Drainage-angle anatomy
- Previous measurements
- Steroid exposure
- Rate of change over time
Some people with pressures above 21 mmHg have ocular hypertension rather than glaucoma.
What Is Ocular Hypertension?
Ocular hypertension means the eye pressure is consistently elevated but there is no definite evidence of glaucomatous optic-nerve damage.
The patient may have:
- Raised pressure
- A normal optic nerve
- Normal OCT measurements
- Normal visual fields
- An open drainage angle
Ocular hypertension is a risk factor for glaucoma, but it is not glaucoma itself.
Some patients remain stable for life. Others later develop primary open-angle glaucoma.
The Ocular Hypertension Treatment Study showed that pressure-lowering medication reduced the five-year risk of developing glaucoma by more than half, but the benefit was greatest in patients with a higher underlying risk.
This is why not every person with ocular hypertension requires immediate treatment.
Which Ocular-Hypertension Patients Are More Likely to Develop Glaucoma?
Important risk factors identified in the Ocular Hypertension Treatment Study include:
- Older age
- Higher eye pressure
- Thinner central cornea
- Larger vertical cup-to-disc ratio
- Certain baseline visual-field measurements
A thin cornea may influence both the measured pressure and the biological susceptibility of the eye. The OHTS found that eyes with thinner central corneas had a higher risk of developing glaucoma within each pressure group.
Risk calculators can help estimate probability, but they do not replace clinical judgement or ongoing examination.
Can a Person Have Glaucoma with Normal Eye Pressure?
Yes.
This is called normal-tension glaucoma.
In normal-tension glaucoma:
- Pressure readings remain within the usual statistical range.
- The optic nerve shows glaucomatous damage.
- OCT may show nerve-fibre or ganglion-cell loss.
- The visual field develops characteristic defects.
Possible explanations include:
- An optic nerve that is unusually sensitive to pressure
- Undetected pressure peaks outside clinic hours
- Night-time pressure changes
- Thin or biomechanically unusual corneas
- Vascular or perfusion factors
- Structural susceptibility of the optic nerve
Lowering pressure can slow progression even when the initial pressure is not statistically high.
Why Is Eye Pressure Important If It Is Not the Whole Diagnosis?
Eye pressure is the most important modifiable risk factor for glaucoma.
Major clinical trials have shown that lowering pressure reduces:
- The risk of ocular hypertension converting to glaucoma
- Progression of established open-angle glaucoma
- Progression of normal-tension glaucoma
In the Early Manifest Glaucoma Trial, the risk of progression decreased by approximately 10% for each 1 mmHg reduction from baseline at the first follow-up.
Pressure is therefore important, but the final goal is not merely to produce a particular number.
The goal is to prevent further optic-nerve and visual-field damage.
What Is a Target Eye Pressure?
The target pressure is the pressure range considered sufficiently low to reduce the likelihood of further glaucoma damage in an individual eye.
It is not a fixed lifelong number.
The target depends on:
- Untreated baseline pressure
- Severity of optic-nerve damage
- Visual-field loss
- Rate of progression
- Age and life expectancy
- Corneal thickness
- Glaucoma type
- Pressure in the other eye
- Treatment tolerance
- Other ocular and systemic risk factors
The 2025 American Academy of Ophthalmology guideline considers an initial reduction of approximately 20% to 30% below baseline reasonable for many patients with primary open-angle glaucoma, followed by adjustment according to disease course and severity.
Advanced or rapidly progressing glaucoma may require a substantially lower target.
Why Can the Target Pressure Change?
The target may be lowered when:
- OCT shows confirmed progression.
- The visual field deteriorates.
- An optic-disc haemorrhage appears.
- The other eye becomes severely affected.
- Pressure fluctuates above the intended range.
- The patient is young and has many years of risk ahead.
- Damage approaches central fixation.
The target may occasionally be reconsidered upward when:
- Treatment causes significant harm.
- Surgery creates dangerously low pressure.
- The original risk estimate changes.
- Repeated high-quality tests show long-term stability.
A target pressure is therefore a working clinical estimate—not a guarantee.
How Is Eye Pressure Measured?
Eye pressure is estimated using an instrument called a tonometer.
The process is called tonometry.
Clinical instruments do not directly insert a pressure gauge inside the eye. Instead, they estimate internal pressure by measuring how the cornea responds to a known force.
This means the result is influenced not only by true internal pressure but also by:
- Corneal thickness
- Curvature
- Elasticity
- Rigidity
- Scarring
- Swelling
- Previous corneal surgery
Goldmann applanation tonometry remains the conventional reference standard, but every clinical method has limitations.
What Is Goldmann Applanation Tonometry?
Goldmann applanation tonometry is commonly performed at a slit lamp.
The procedure usually involves:
- Applying a numbing eye drop.
- Applying fluorescein dye.
- Positioning the patient at the slit lamp.
- Gently touching the central cornea with a small measuring prism.
- Adjusting the force needed to flatten a standardised area of cornea.
The test is usually painless because the cornea has been numbed.
Goldmann tonometry is widely used for glaucoma diagnosis and monitoring and has been the measurement method used in many major glaucoma trials.
Can Goldmann Tonometry Scratch the Eye?
A properly performed measurement is generally very safe.
Rare problems include:
- Temporary irritation
- Corneal epithelial disturbance
- Allergy to the numbing or fluorescein drops
- Infection if instruments are not disinfected appropriately
The patient should avoid rubbing the eye while the surface remains numb.
What Is the Air-Puff Test?
Non-contact tonometry uses a brief puff of air to flatten the cornea.
The instrument estimates pressure based on how the cornea responds.
Advantages include:
- No direct instrument contact
- No numbing drop in most cases
- Quick screening
- Ease of use in high-volume settings
Limitations include:
- Greater sensitivity to corneal properties
- Possible overestimation or disagreement at higher pressures
- Startle or eyelid squeezing
- Less suitability for making major treatment decisions from one isolated reading
An air-puff result is useful for screening, but an unexpectedly high or clinically important result may need confirmation using applanation or another appropriate method. Comparisons show that non-contact and Goldmann readings are not always interchangeable.
What Is Rebound Tonometry?
Rebound tonometry uses a small lightweight probe that briefly touches the cornea and rebounds.
The device calculates pressure from the probe’s motion.
Advantages include:
- Very brief contact
- Often no numbing drop
- Portable equipment
- Easier use in children
- Use in patients unable to sit at a slit lamp
- Availability of selected home-monitoring devices
Rebound tonometry is especially useful in paediatric practice, although readings may differ systematically from Goldmann measurements and remain affected by corneal thickness and biomechanics.
What Is a Tono-Pen?
A Tono-Pen is a handheld electronic applanation instrument.
It may be useful when:
- The patient cannot sit at a slit lamp
- The cornea is irregular
- The patient is lying down
- The eye is being assessed after surgery
- A portable measurement is needed
It provides valuable clinical information but does not always match Goldmann measurements exactly.
What Are Dynamic Contour Tonometry and Corneal-Compensated Pressure?
Other devices aim to reduce the influence of corneal properties.
Examples include:
- Dynamic contour tonometry
- Ocular Response Analyzer
- Corvis-based biomechanically corrected pressure
These instruments may provide additional information about:
- Corneal hysteresis
- Corneal deformation
- Biomechanically adjusted pressure
They can be particularly useful in selected patients, such as those who have undergone refractive surgery or whose glaucoma appears to progress despite apparently low Goldmann readings.
However, these measurements are not universally interchangeable with Goldmann pressure and should be interpreted according to the specific device.
Why Can Different Machines Give Different Readings?
Tonometers use different physical principles.
They may respond differently to:
- Thick or thin corneas
- Corneal stiffness
- Keratoconus
- Corneal scars
- Previous LASIK or PRK
- Corneal swelling
- High or low pressure ranges
- Eyelid tension
- Patient movement
A difference of a few mmHg between devices does not necessarily mean the pressure genuinely changed.
For long-term monitoring, it is often helpful to:
- Use the same method when practical
- Record which instrument was used
- Consider the time of measurement
- Repeat unexpected readings
- Compare the result with optic-nerve and field findings
Why Does Corneal Thickness Affect Eye-Pressure Readings?
Most tonometers estimate pressure by deforming the cornea.
A relatively thick or stiff cornea may require more force to flatten, potentially producing a higher measured pressure.
A relatively thin or flexible cornea may require less force, potentially producing a lower measured pressure.
However, central corneal thickness does not act as a simple mathematical error that can be perfectly corrected.
It is also associated independently with glaucoma risk in ocular hypertension.
For this reason, clinicians generally record the measured pressure and consider corneal thickness as part of the overall interpretation rather than relying on a universal correction table.
What Is Pachymetry?
Pachymetry measures corneal thickness.
The test may use:
- Ultrasound
- Optical scanning
- Corneal tomography
- Anterior-segment OCT
It is usually quick and painless.
Pachymetry is particularly useful when assessing:
- Ocular hypertension
- Glaucoma suspects
- Unexpectedly high or low pressure
- Previous refractive surgery
- Corneal disease
- Risk of progression
Does a Thick Cornea Protect Against Glaucoma?
Not necessarily.
A thick cornea may contribute to a higher measured pressure, but it does not make the optic nerve immune to glaucoma.
Similarly, a thin cornea may cause pressure to be underestimated and may also indicate increased risk in ocular hypertension.
The optic nerve, OCT and visual field remain essential.
How Do LASIK, PRK and SMILE Affect Pressure Measurements?
Corneal refractive surgery changes:
- Corneal thickness
- Curvature
- Biomechanical behaviour
After myopic LASIK or PRK, Goldmann and some other tonometers commonly record a lower pressure even when the actual internal pressure has not fallen by the same amount.
The degree of underestimation varies and cannot be corrected reliably using one universal formula.
Patients should tell their eye doctor if they have undergone:
- LASIK
- PRK
- SMILE
- Other corneal laser procedures
Old preoperative pressure and corneal-thickness records may be useful.
Can LASIK Hide Glaucoma?
It can complicate detection if the lower post-LASIK pressure reading is interpreted without considering the altered cornea.
The original myopic eye may also carry an increased glaucoma risk.
A patient with previous refractive surgery may require:
- Careful optic-nerve examination
- OCT
- Visual-field testing
- Alternative tonometry
- Review of preoperative records
Clear unaided vision after LASIK does not protect against glaucoma.
How Does Keratoconus Affect Eye-Pressure Measurement?
Keratoconus causes the cornea to become:
- Thinner
- Steeper
- More irregular
- Biomechanically weaker
Standard pressure measurements may therefore underestimate or vary unpredictably.
Corneal cross-linking, rigid contact lenses and previous corneal procedures can further affect interpretation.
Pressure should be assessed alongside the overall corneal and optic-nerve findings.
Can Corneal Swelling Affect the Reading?
Yes.
A swollen or diseased cornea may produce unreliable readings.
Examples include:
- Fuchs endothelial dystrophy
- Acute angle closure with corneal oedema
- Corneal infection
- Postoperative swelling
- Contact-lens-related oedema
The direction and size of the error may vary according to the degree and type of swelling.
Does Eye Pressure Change During the Day?
Yes.
Eye pressure is not fixed.
It can vary with:
- Time of day
- Sleep and waking
- Body position
- Medication timing
- Fluid intake
- Physical activity
- Hormonal and physiological factors
Many people have higher readings during the night or early morning, although the pattern is not identical or perfectly repeatable for everyone. Reviews have also found that both corneal thickness and measured IOP tend to change during the day.
A single office reading provides only a snapshot.
Why Is My Pressure Higher in the Morning?
Possible contributors include:
- Overnight body position
- Changes in aqueous production and drainage
- Corneal swelling during sleep
- Hormonal variation
- Medication effect wearing off
Not every patient has a morning peak.
Some patients experience their highest pressure outside normal clinic hours.
What Is a Diurnal Pressure Curve?
A diurnal pressure curve involves measuring pressure at several times during the day.
It may be useful when:
- Glaucoma progresses despite apparently acceptable clinic readings
- Pressure fluctuation is suspected
- Treatment timing is being evaluated
- One eye behaves differently from the other
- Normal-tension glaucoma is suspected
Office-hour testing may still miss night-time peaks.
Can Eye Pressure Be Measured at Home?
Selected patients may use a home rebound tonometer after training.
Home measurements can reveal:
- Early-morning peaks
- Evening changes
- Out-of-office pressure spikes
- Response to medication
- Differences between days
A 2025 study found home rebound tonometry clinically useful for detecting out-of-office pressure patterns and spikes.
Home monitoring should supplement—not replace—professional examination, OCT and visual-field testing.
Can I Check Eye Pressure by Pressing on My Eyelids?
No.
Feeling the eye through the eyelid is not a safe or accurate way to measure pressure.
Repeated pressing may:
- Irritate the eye
- Distort the cornea
- Raise pressure temporarily
- Cause injury after surgery
- Delay proper assessment
Only an appropriate tonometer can estimate pressure reliably.
Why Is My Pressure Different at Each Visit?
Possible reasons include:
- Natural fluctuation
- Different appointment times
- Different instruments
- Different examiners
- Medication timing
- Missed doses
- Corneal dryness
- Corneal thickness changes
- Eyelid squeezing
- Breath holding
- Body position
- Recent exercise
- Caffeine or fluid intake
- Stress and patient cooperation
Clinicians are generally more concerned about a consistent trend or confirmed spike than a small isolated difference.
Can Holding My Breath Raise the Reading?
Yes.
Breath holding and straining can temporarily raise venous pressure and eye pressure.
During measurement, patients should:
- Breathe normally
- Avoid squeezing the eyelids
- Relax the forehead and shoulders
- Avoid pressing the face against the slit-lamp frame
Can Eyelid Squeezing Affect the Result?
Yes.
Forceful eyelid closure may increase the reading.
This is especially relevant when the patient:
- Is anxious
- Dislikes the air puff
- Has eyelid spasm
- Presses against the examiner
- Tries to close the eye around the tonometer
The measurement may need to be repeated after the patient relaxes.
Does Body Position Affect Eye Pressure?
Yes.
Pressure is generally higher when lying flat than when sitting upright, and certain head-down positions can cause temporary elevations.
This may be relevant to:
- Night-time pressure
- Inverted yoga postures
- Postoperative instructions
- Advanced glaucoma
- Sleep-position discussions
Most patients do not need to sleep sitting upright unless specifically advised.
Does Exercise Affect Eye Pressure?
Moderate aerobic exercise commonly produces a temporary reduction in eye pressure.
However, some activities can temporarily raise it, particularly:
- Heavy straining
- Breath holding
- Very high-resistance weightlifting
- Prolonged inverted postures
Exercise remains beneficial for general health and is usually encouraged.
Patients with advanced or unstable glaucoma should obtain individual advice regarding:
- Heavy lifting
- Head-down yoga
- High-resistance activities
- Competitive wind instruments
- Tight swimming goggles
The relationship between exercise and pressure is complex and depends on the activity, breathing technique and patient.
Does Drinking a Lot of Water Raise Eye Pressure?
Rapidly drinking a large volume of water can temporarily increase eye pressure.
This principle is used in the water-drinking test, which may assess outflow reserve in selected glaucoma patients.
Ordinary hydration is appropriate.
There is generally no need to restrict normal fluid intake unless another medical condition requires it.
It is reasonable to spread fluid intake through the day rather than rapidly consuming a very large volume.
Does Coffee Raise Eye Pressure?
Caffeine may cause a mild and temporary pressure increase in some people, particularly those with glaucoma or ocular hypertension.
The response is variable.
Available systematic evidence has not shown a clinically important pressure rise in every healthy person.
Most patients do not need to eliminate moderate coffee intake.
Those with unstable or advanced glaucoma may discuss heavy caffeine consumption with their ophthalmologist.
Can Tight Neckties or Clothing Raise Eye Pressure?
Anything that markedly increases pressure in the neck veins may theoretically raise eye pressure temporarily.
Ordinary clothing is unlikely to be a major cause of glaucoma.
The more important long-term factors remain:
- Baseline pressure
- Optic-nerve susceptibility
- Adherence to treatment
- Disease progression
Can Swimming Goggles Affect Eye Pressure?
Very tight goggles that press on the tissues around the eye may raise pressure temporarily.
Goggles should rest appropriately around the bony orbit rather than compressing the eyeball.
Patients with advanced glaucoma may wish to avoid excessively tight small-socket goggles.
Does Screen Time Raise Eye Pressure?
Ordinary computer, tablet and smartphone use does not generally cause chronic high eye pressure or glaucoma.
Screen use may cause:
- Dry eye
- Eye strain
- Headache
- Temporary blur
These symptoms do not reliably indicate elevated pressure.
Can Stress Raise Eye Pressure?
Acute stress may produce small physiological changes, but everyday stress is not a reliable explanation for persistently high eye pressure.
An elevated result should not be dismissed as “just stress” without appropriate reassessment.
Can Eye Pressure Be Different Between the Two Eyes?
Yes.
Small differences are common.
A persistent or large difference may raise concern for:
- Asymmetrical glaucoma
- Previous trauma
- Steroid exposure in one eye
- Uveitis
- Angle abnormalities
- Previous surgery
- Retinal vascular disease
- Measurement differences
- Corneal-thickness differences
The significance depends on the full examination.
Does High Eye Pressure Cause Symptoms?
Usually not.
Moderately elevated pressure may remain completely painless.
A patient may have a pressure in the high twenties or beyond without feeling anything, particularly if the rise developed gradually.
Symptoms are more likely when pressure rises:
- Suddenly
- To a very high level
- With corneal swelling
- Because the drainage angle closes
- With significant inflammation
Possible symptoms include:
- Eye pain
- Redness
- Blurred vision
- Halos
- Headache
- Nausea
- Vomiting
When Is High Eye Pressure an Emergency?
Seek urgent eye care for:
- Severe eye pain
- A red eye with reduced vision
- Halos around lights
- Severe headache with eye symptoms
- Nausea or vomiting
- A cloudy cornea
- Sudden pressure elevation after surgery
- Trauma with pain or blur
- Rapid visual loss
These symptoms may indicate acute angle closure or another sight-threatening condition.
What Causes High Eye Pressure?
Pressure may rise because of:
- Primary open-angle outflow resistance
- Anatomically narrow or closed angles
- Steroid response
- Eye trauma
- Uveitis
- Pseudoexfoliation
- Pigment dispersion
- Abnormal iris blood vessels
- Lens-related blockage
- Bleeding inside the eye
- Previous surgery
- Certain medications
- Congenital drainage abnormalities
Identifying the cause matters because different mechanisms require different treatments.
How Do Steroids Raise Eye Pressure?
Steroids can alter the trabecular meshwork and reduce aqueous outflow.
Pressure elevation can occur with:
- Steroid eye drops
- Steroid ointments
- Injections around or inside the eye
- Oral medication
- Inhalers
- Nasal sprays
- Skin creams, particularly near the eyes
- Intravenous treatment
The response varies greatly between individuals.
Steroid-induced ocular hypertension can lead to irreversible glaucomatous damage if it remains undetected.
Patients should not stop medically necessary steroids abruptly, but pressure monitoring may be required.
Who Is More Likely to Have a Steroid Pressure Response?
Risk may be greater in:
- Existing glaucoma
- Family history of glaucoma
- High myopia
- Previous steroid response
- Younger children
- Older adults
- Diabetes
- Connective-tissue disease
- Prolonged or potent steroid exposure
Pressure may rise within weeks, but timing varies according to the medication and route.
Can Eye Injury Raise Pressure Years Later?
Yes.
Blunt trauma can damage the drainage angle, producing angle recession.
Pressure elevation may develop:
- Immediately
- Months later
- Many years after the injury
A history of significant eye trauma remains relevant even when the eye appeared to recover fully.
Can Inflammation Raise or Lower Pressure?
Yes.
Uveitis can cause pressure to rise through:
- Inflammatory blockage
- Scarring of the drainage angle
- Iris adhesions
- Steroid treatment
- Reduced outflow
Severe inflammation can also reduce aqueous production and produce low pressure.
The treatment must balance control of inflammation with pressure management.
What Is Low Eye Pressure?
Abnormally low eye pressure is called ocular hypotony.
A numerical definition varies between studies, but pressures below approximately 5 to 6.5 mmHg are commonly considered statistically low.
The more important question is whether the low pressure is causing structural or visual problems.
Some eyes tolerate a low number without major symptoms. Others develop:
- Blurred or fluctuating vision
- Corneal changes
- Choroidal detachment
- Retinal or macular folds
- A shallow anterior chamber
- Discomfort
- Distortion of the eyeball
Hypotony is uncommon but potentially sight-threatening.
What Causes Low Eye Pressure?
Possible causes include:
- A leaking surgical wound
- Overfiltration after glaucoma surgery
- Severe inflammation
- Trauma
- Cyclodialysis cleft
- Retinal detachment
- Reduced aqueous production
- Excessive pressure-lowering treatment
- Complications of retinal or glaucoma surgery
Persistent low pressure after eye surgery requires assessment.
Can Pressure Be Too Low After Glaucoma Surgery?
Yes.
Glaucoma surgery aims to lower pressure, but excessively low pressure may cause:
- Hypotony maculopathy
- Choroidal detachment
- Shallow anterior chamber
- Corneal problems
- Cataract-related complications
- Reduced vision
The ideal pressure is therefore not “as low as possible.”
It is low enough to protect the optic nerve while high enough to maintain healthy eye structure and function.
How Is High Eye Pressure Lowered?
Treatment may involve:
- Eye drops
- Laser treatment
- Surgery
- Treatment of an underlying cause
The best option depends on:
- Glaucoma type
- Pressure level
- Optic-nerve damage
- Target pressure
- Angle anatomy
- Previous treatment
- Age
- Ocular surface
- Medication tolerance
How Do Eye Drops Lower Pressure?
Pressure-lowering drops may:
- Reduce aqueous production
- Increase trabecular drainage
- Increase uveoscleral drainage
- Combine more than one mechanism
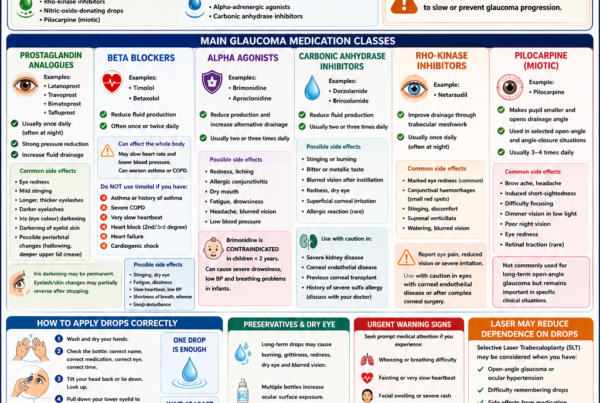
Common groups include:
- Prostaglandin analogues
- Beta blockers
- Alpha agonists
- Carbonic anhydrase inhibitors
- Rho-kinase inhibitors
- Combination drops
The choice depends on pressure reduction, medical history, side effects, dosing frequency and availability.
Why Press the Inner Corner After Applying a Drop?
After instilling a drop:
- Close the eyelids gently.
- Press the inner corner beside the nose for one to two minutes.
This reduces drainage into the nose and may:
- Increase medication contact with the eye
- Reduce systemic absorption
- Reduce body-wide side effects
Only one drop is required.
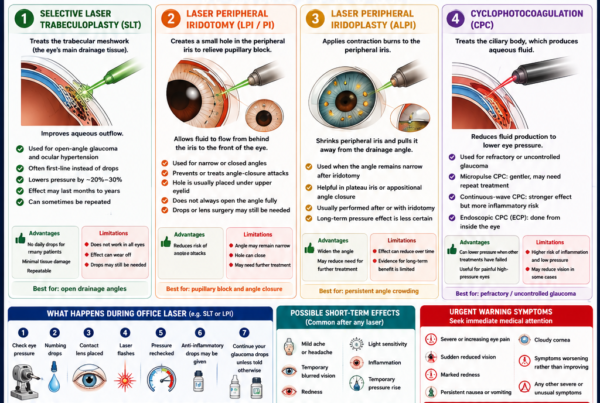
What Is Selective Laser Trabeculoplasty?
Selective laser trabeculoplasty, or SLT, applies laser energy to the trabecular meshwork to improve drainage in open-angle disease.
It may be used:
- As first-line treatment
- To reduce reliance on drops
- When drops cause side effects
- When adherence is difficult
- In addition to medication
SLT does not work for every eye, and the effect may reduce over time.
How Does Laser Iridotomy Affect Pressure?
Laser peripheral iridotomy creates a small opening in the peripheral iris.
It is used primarily when pressure risk is related to:
- Pupillary block
- Narrow drainage angles
- Acute angle closure
The opening allows fluid to move more freely from behind the iris into the anterior chamber.
It does not treat every cause of high pressure and does not guarantee that future medication will be unnecessary.
Can Cataract Surgery Lower Eye Pressure?
Yes.
Removing the natural lens can:
- Deepen the anterior chamber
- Widen the drainage angle
- Improve aqueous access to the trabecular meshwork
- Reduce pressure in selected patients
The effect is particularly relevant in angle-closure disease.
Cataract surgery may also provide a modest pressure reduction in some open-angle eyes, but it is not a substitute for glaucoma surgery when a very low target is required.
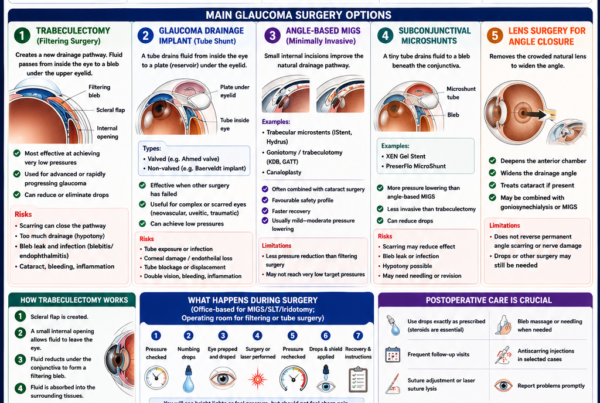
When Is Glaucoma Surgery Needed?
Surgery may be considered when:
- Pressure remains above target
- OCT or visual fields continue worsening
- Medication is not tolerated
- Adherence is unreliable
- Pressure is dangerously high
- Glaucoma is advanced
- Laser is insufficient
- The underlying mechanism requires surgery
Options include:
- Trabeculectomy
- Glaucoma drainage implants
- Minimally invasive glaucoma surgery
- Cyclophotocoagulation
- Other angle procedures
Can Lifestyle Replace Pressure-Lowering Treatment?
No.
Lifestyle measures may support general health and cause small temporary pressure changes, but they should not replace prescribed drops, laser or surgery.
Patients should not stop treatment because of:
- Exercise
- Supplements
- Dietary changes
- Meditation
- Acupuncture
- Cannabis
- Eye exercises
Pressure-lowering treatment is the only established strategy proven to modify glaucoma risk and progression.
Can Cannabis Lower Eye Pressure?
Cannabis can lower pressure temporarily, but the effect is short-lived.
Maintaining control would require repeated exposure throughout the day and night, causing significant cognitive, cardiovascular and functional effects.
It is not considered a practical or recommended glaucoma treatment.
Should Everyone with Pressure Above 21 Be Treated?
No.
Treatment decisions should consider:
- Estimated risk of developing glaucoma
- Life expectancy
- Pressure level
- Corneal thickness
- Optic-nerve appearance
- OCT
- Visual fields
- Family history
- Patient preference
- Treatment burden and side effects
A young patient with pressure of 28 mmHg, a thin cornea and suspicious nerve may warrant treatment.
An older patient with pressure of 22 mmHg, a thick cornea and decades of stable testing may be monitored.
Can a Normal Pressure Reading Exclude Glaucoma?
No.
A normal reading cannot exclude:
- Normal-tension glaucoma
- Previous pressure peaks
- Night-time elevation
- Underestimation after refractive surgery
- Thin-cornea measurement effects
- Existing optic-nerve damage
Glaucoma assessment requires more than tonometry.
What Other Tests Are Needed?
Depending on the clinical context, assessment may include:
Optic-Nerve Examination
Looks for:
- Rim thinning
- Notching
- Cupping
- Disc haemorrhage
- Asymmetry
OCT
Measures:
- Retinal nerve-fibre layer
- Macular ganglion cells
- Optic-nerve structures
Visual-Field Testing
Detects functional blind spots and progression.
Gonioscopy
Determines whether the drainage angle is:
- Open
- Narrow
- Closed
- Scarred
- Damaged by trauma
- Blocked by abnormal vessels
Pachymetry
Measures central corneal thickness.
Optic-Disc Photography
Documents long-term structural appearance.
The AAO guideline emphasises that structural OCT and functional visual-field testing provide complementary information when monitoring glaucoma.
Frequently Asked Questions
Is pressure of 18 normal?
It falls within the commonly quoted statistical range, but whether it is safe depends on the optic nerve and target pressure.
Is pressure of 20 high?
It is near the upper end of the common range but is not automatically abnormal.
Is pressure of 22 glaucoma?
No.
It may represent measurement variation, ocular hypertension or glaucoma depending on the rest of the examination.
Is pressure of 30 dangerous?
It requires prompt assessment.
Some patients have no symptoms, but the risk of optic-nerve damage is greater, and the cause must be identified.
Can pressure of 12 still be glaucoma?
Yes.
Normal-tension glaucoma can occur at low-normal pressure levels.
Which eye-pressure number causes blindness?
There is no single number.
Risk depends on:
- Duration
- Optic-nerve susceptibility
- Glaucoma type
- Existing damage
- Pressure fluctuation
- Speed of pressure rise
Can I feel when my pressure is high?
Usually not.
Chronic pressure elevation is often painless.
Why was my pressure high on the air-puff test but normal later?
Possible reasons include:
- Eyelid squeezing
- Startle response
- Corneal properties
- Device differences
- Natural fluctuation
- Measurement error
Which eye-pressure test is most accurate?
Goldmann applanation remains the conventional clinical reference, but no non-invasive instrument measures true internal pressure perfectly.
The most appropriate method depends on the cornea and clinical situation.
Why does my doctor repeat the pressure?
Repeating may confirm:
- An unexpected result
- Variation between measurements
- Whether eyelid squeezing affected the test
- Whether both eyes are genuinely different
Why is the pressure measured before pupil dilation?
Dilation can alter pressure or angle anatomy in selected eyes.
Measuring before dilation provides a baseline and helps identify patients with narrow angles.
Can dilating drops raise pressure?
They may cause a temporary rise in some patients.
In anatomically narrow eyes, dilation can occasionally precipitate angle closure.
Can contact lenses affect the measurement?
Yes.
Most accurate routine measurements are taken after removing contact lenses.
Some rebound devices can measure over selected soft lenses, but readings may differ from measurements on the bare cornea.
Does rubbing the eye raise pressure?
Rubbing or pressing can cause temporary pressure changes and may injure the cornea.
It should be avoided, particularly after eye surgery.
Can lack of sleep raise pressure?
Sleep and circadian rhythm affect pressure patterns, but one poor night does not by itself diagnose glaucoma.
Does sleep apnoea affect eye pressure?
Sleep apnoea may be associated with glaucoma through several possible mechanisms, including oxygen and vascular changes.
It should be treated for overall health, but treatment does not replace glaucoma monitoring.
Can eye pressure improve naturally?
It fluctuates and may occasionally fall without treatment, but persistently high or glaucomatous pressure should not be managed by waiting for spontaneous improvement.
Can pressure-lowering drops stop working?
Their effect may appear reduced because of:
- Disease progression
- Poor adherence
- Incorrect instillation
- Bottle problems
- Medication timing
- Biological response
- Changes in outflow resistance
Why is my pressure still high despite using drops?
Possible reasons include:
- Missed doses
- Incorrect technique
- Inadequate response
- Steroid use
- Progression of angle closure
- Secondary glaucoma
- Medication interactions
- Need for laser or surgery
Should glaucoma drops be used before the appointment?
Usually, yes.
Continue the normal schedule unless the clinic specifically asks otherwise.
Can lowering pressure restore lost vision?
No.
Lowering pressure protects remaining optic-nerve tissue but does not usually regenerate vision already lost from glaucoma.
Can pressure be checked after cataract surgery?
Yes.
Monitoring is important because pressure may rise temporarily after surgery.
Can eye pressure rise after an injection into the eye?
Yes.
Intravitreal injections may produce a temporary pressure rise. Repeated steroid injections can also produce sustained ocular hypertension in susceptible patients.
Can children have high eye pressure?
Yes.
Possible causes include:
- Congenital glaucoma
- Juvenile glaucoma
- Steroid response
- Trauma
- Uveitis
- Previous childhood eye surgery
Measurements can be more difficult in children, making rebound or handheld instruments useful.
A Practical Eye-Pressure Assessment
Step 1: Confirm the Reading
- Repeat an unexpected measurement.
- Record the instrument.
- Ensure the patient is relaxed.
- Consider the time of day.
- Check medication timing.
Step 2: Assess the Cornea
- Measure central corneal thickness.
- Look for scarring or swelling.
- Document previous LASIK, PRK or SMILE.
- Consider corneal biomechanics.
Step 3: Examine the Drainage Angle
- Perform gonioscopy.
- Identify open, narrow or closed angles.
- Look for pigment, trauma, adhesions or abnormal vessels.
Step 4: Examine the Optic Nerve
- Assess the cup and neural rim.
- Compare the two eyes.
- Look for nerve-fibre defects and disc haemorrhage.
Step 5: Perform Structural and Functional Tests
- OCT
- Visual-field testing
- Optic-disc photography
Step 6: Determine Risk
Consider:
- Age
- Family history
- Myopia
- Steroid exposure
- Corneal thickness
- Baseline pressure
- Previous progression
Step 7: Set or Review the Target Pressure
- Consider disease severity.
- Assess treatment tolerance.
- Lower the target if progression continues.
Step 8: Choose Treatment or Monitoring
Options include:
- Observation
- Eye drops
- Laser
- Cataract or lens surgery
- Glaucoma surgery
- Treatment of the underlying cause
Common Myths About Eye Pressure
“Anything below 21 is safe.”
False.
Glaucoma can progress below 21 mmHg.
“Anything above 21 means glaucoma.”
False.
Some people have ocular hypertension without damage.
“I can feel when my pressure rises.”
Usually false.
Chronic high pressure is commonly painless.
“The air-puff test alone can diagnose glaucoma.”
False.
It measures pressure but not optic-nerve damage.
“A thick cornea means I cannot get glaucoma.”
False.
Corneal thickness affects interpretation but does not guarantee protection.
“LASIK lowers my glaucoma risk because the pressure reading fell.”
False.
The lower reading may reflect altered corneal measurement rather than a true pressure reduction.
“The lowest possible pressure is always best.”
False.
Pressure that is too low can damage the eye.
“Coffee causes glaucoma.”
Not proven.
Caffeine may cause a small temporary pressure rise in some people but is not the sole cause of glaucoma.
“Exercise can replace glaucoma drops.”
False.
Exercise supports general health but does not replace prescribed treatment.
The Bottom Line
Eye pressure is the internal fluid pressure of the eye.
It is created mainly by the balance between:
- Aqueous-humour production
- Aqueous-humour drainage
A common statistical range is approximately 10 to 21 mmHg, but there is no universal safe number.
A patient may have:
- High pressure without glaucoma
- Glaucoma with normal pressure
- Pressure affected by corneal thickness
- Underestimated pressure after LASIK or PRK
- Pressure spikes outside clinic hours
- Different target pressures in each eye
Eye pressure is estimated using tonometry.
Common methods include:
- Goldmann applanation
- Air-puff tonometry
- Rebound tonometry
- Handheld applanation devices
- Corneal-biomechanical instruments
The pressure must be interpreted together with:
- Optic-nerve examination
- OCT
- Visual-field testing
- Gonioscopy
- Corneal thickness
- Long-term progression
High pressure usually causes no symptoms. Severe pain, redness, halos, blurred vision, headache or vomiting may indicate acute angle closure and require emergency care.
Lowering pressure is the only established strategy proven to reduce the development and progression of glaucoma.
The important question is not simply, “Is my pressure normal?” It is, “Is this pressure safe for my optic nerve, and is my eye remaining stable over time?”
References
- National Eye Institute. Glaucoma and Eye Pressure. Updated December 2024.
- Gedde SJ, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. American Academy of Ophthalmology. 2025–2026.
- National Institute for Health and Care Excellence. Glaucoma: Diagnosis and Management. Guideline NG81.
- Brusini P, et al. How to Measure Intraocular Pressure: An Updated Review of Various Tonometers. Journal of Clinical Medicine. 2021.
- Gordon MO, et al. The Ocular Hypertension Treatment Study: Baseline Factors That Predict the Onset of Primary Open-Angle Glaucoma. Archives of Ophthalmology. 2002.
- Heijl A, et al. Reduction of Intraocular Pressure and Glaucoma Progression: Results from the Early Manifest Glaucoma Trial. Archives of Ophthalmology. 2002.
- Leske MC, et al. Factors for Glaucoma Progression and the Effect of Treatment. Archives of Ophthalmology. 2003.
- Collaborative Normal-Tension Glaucoma Study Group. The Effectiveness of Intraocular Pressure Reduction in Normal-Tension Glaucoma. American Journal of Ophthalmology. 1998.
- Barberán-Bernardos L, et al. Corneal and Intraocular Pressure Changes Associated with Diurnal Variation. 2024.
- De Bernardo M, et al. Reliability of Intraocular Pressure Measurement by Goldmann Applanation Tonometry After Refractive Surgery. 2020.
- Harvey DH, et al. Glucocorticoid-Induced Ocular Hypertension and Glaucoma. 2024.
- Wang Q, et al. Ocular Hypotony: A Comprehensive Review. Survey of Ophthalmology. 2019.
- Lambert SR, et al. Rebound Tonometry in Children: A Report by the American Academy of Ophthalmology. Ophthalmology. 2013.
- Perkins SW, et al. Home Tonometry: Diurnal Intraocular Pressure Patterns and Out-of-Office Pressure Spikes. 2025.