Author: Dr Val Phua
Estimated reading time: 13–15 minutes
What Is Glaucoma?
Glaucoma is a group of eye diseases that progressively damage the optic nerve—the structure that carries visual information from the eye to the brain.
Without treatment, glaucoma can cause:
- Permanent loss of peripheral vision
- Increasing difficulty navigating or driving
- Tunnel vision
- Central visual loss in advanced disease
- Irreversible blindness
The most important modifiable risk factor is pressure inside the eye, known as intraocular pressure or IOP.
However, glaucoma is not simply “high eye pressure.”
Some people have:
- High eye pressure without optic-nerve damage
- Glaucoma despite pressure readings within the statistically normal range
- Pressure that fluctuates and is missed during a single clinic visit
- Optic nerves that are more vulnerable to a particular pressure level
Glaucoma is therefore diagnosed by assessing the optic nerve, retinal nerve-fibre layer and visual field—not by relying on one pressure reading alone.
The National Eye Institute defines glaucoma as a group of diseases that can cause vision loss and blindness through optic-nerve damage. Early treatment can often slow or prevent further damage, but vision that has already been lost cannot usually be restored.
What Does the Optic Nerve Do?
The optic nerve is a cable-like structure connecting the retina to the brain.
It contains more than one million nerve fibres, many of which originate from retinal ganglion cells.
These fibres carry information about:
- Light
- Shape
- Colour
- Contrast
- Movement
- Position within the visual field
Glaucoma gradually damages these retinal ganglion cells and their nerve fibres.
As more fibres are lost, characteristic changes may appear in:
- The optic-nerve head
- The retinal nerve-fibre layer
- Optical coherence tomography scans
- Peripheral visual-field testing
Early damage may not affect central reading vision, so a patient can have significant glaucoma while still reading the smallest letters on an eye chart.
Why Is Glaucoma Called the “Silent Thief of Sight”?
The most common forms of glaucoma usually progress slowly and painlessly.
A person may not notice:
- Early peripheral blind spots
- Gradual loss of contrast
- Difficulty seeing in dim lighting
- Increasing reliance on the better eye
- Loss that the brain automatically fills in
The two eyes also overlap in their fields of vision. One eye may compensate for damage in the other, making the loss difficult to detect without formal testing.
By the time a patient notices tunnel vision or difficulty navigating, the disease may already be advanced.
Glaucoma therefore cannot be excluded simply because:
- Vision seems clear
- There is no pain
- The eyes look white
- The spectacle prescription is stable
- The patient can still read and drive
A comprehensive eye examination is the only reliable way to detect early glaucoma.
How Common Is Glaucoma in Singapore?
Glaucoma becomes more common with increasing age.
Singapore HealthHub reports that it affects approximately 3% of people over 40, with risk increasing in older age groups. Population studies in Singapore have found substantial burdens of both open-angle and angle-closure glaucoma across Chinese, Malay and Indian communities.
Importantly, many affected people are unaware that they have the condition.
This is because early glaucoma often causes no symptoms and cannot be diagnosed through spectacle checks alone.
What Is Eye Pressure?
The front part of the eye contains a clear fluid called aqueous humour.
This fluid:
- Is produced by the ciliary body behind the iris.
- Flows through the pupil.
- Circulates through the anterior chamber.
- Drains through the trabecular meshwork at the angle of the eye.
- Leaves through drainage channels into the bloodstream.
Eye pressure depends on the balance between:
- How much aqueous fluid the eye produces
- How easily the fluid drains
If fluid cannot leave efficiently, pressure may rise.
The eye is not filled with air, and glaucoma pressure is unrelated to blood pressure in a simple one-to-one way.
What Is a Normal Eye Pressure?
Eye pressure is commonly measured in millimetres of mercury, abbreviated as mmHg.
Many healthy eyes have pressures between approximately 10 and 21 mmHg, but this is a population range rather than a strict boundary between health and disease.
A pressure of 19 mmHg may be too high for a severely damaged or vulnerable optic nerve.
A pressure of 24 mmHg may not yet have caused damage in another person.
The significance of a pressure reading depends on:
- Optic-nerve appearance
- Visual-field results
- OCT findings
- Corneal thickness
- Age
- Family history
- Drainage-angle anatomy
- Previous pressure readings
- Rate of progression
- Other ocular and systemic factors
Glaucoma treatment therefore aims for an individualised target pressure, not simply a pressure below 21 mmHg.
Can Glaucoma Occur with Normal Eye Pressure?
Yes.
This is called normal-tension glaucoma.
The optic nerve develops characteristic glaucomatous damage even though measured pressure readings remain within the usual population range.
Possible explanations include:
- The optic nerve being unusually pressure-sensitive
- Pressure peaks occurring outside clinic hours
- Night-time pressure elevation
- Reduced blood flow or vascular regulation
- Structural susceptibility of the optic nerve
- Thin corneas affecting pressure interpretation
- Previous periods of higher pressure
The Collaborative Normal-Tension Glaucoma Study demonstrated that lowering pressure can slow progression even when the starting pressure is statistically normal.
Normal pressure therefore does not automatically mean that the optic nerve is safe.
What Is Ocular Hypertension?
Ocular hypertension means that eye pressure is higher than expected but there is no definite glaucomatous damage to the optic nerve or visual field.
Ocular hypertension is not the same as glaucoma.
Some people with ocular hypertension remain stable throughout life. Others later develop primary open-angle glaucoma.
The likelihood of conversion depends on factors including:
- Age
- Pressure level
- Central corneal thickness
- Optic-disc appearance
- Visual-field measurements
- Family history
- Other risk factors
The Ocular Hypertension Treatment Study showed that pressure-lowering treatment can reduce the risk of developing glaucoma, but not every person with ocular hypertension requires immediate treatment. Risk should be assessed individually.
What Is a Glaucoma Suspect?
A glaucoma suspect has one or more findings that raise concern but do not yet prove definite glaucoma.
Examples include:
- Elevated eye pressure
- A large optic-nerve cup
- Asymmetry between the optic nerves
- A thin retinal nerve-fibre layer
- A suspicious visual field
- A strong family history
- Narrow drainage angles
- Optic-disc haemorrhage
A suspect may require:
- Repeat pressure measurements
- Baseline optic-disc photography
- OCT
- Visual-field testing
- Gonioscopy
- Pachymetry
- Continued monitoring
Some glaucoma suspects never develop the disease.
Others show progressive structural or functional change over time, allowing a more definite diagnosis.
What Are the Main Types of Glaucoma?
Glaucoma is not one single disease.
The main categories include:
- Primary open-angle glaucoma
- Normal-tension glaucoma
- Primary angle-closure disease
- Secondary glaucoma
- Childhood and congenital glaucoma
Primary Open-Angle Glaucoma
Primary open-angle glaucoma is one of the most common forms.
In this condition:
- The drainage angle appears open.
- Aqueous fluid still encounters resistance within the drainage system.
- Pressure may be elevated, fluctuating or statistically normal.
- Optic-nerve damage develops gradually.
- Early symptoms are usually absent.
The word “open” describes the anatomical appearance of the drainage angle. It does not mean that fluid is draining normally.
Primary open-angle glaucoma usually requires lifelong monitoring and often lifelong treatment.
Normal-Tension Glaucoma
Normal-tension glaucoma is generally considered part of the open-angle glaucoma spectrum.
The drainage angle is open, but optic-nerve damage occurs at pressure levels that would not usually be considered elevated.
Patients may have:
- Optic-disc haemorrhages
- Localised nerve-fibre defects
- Visual-field loss close to fixation
- Migraine or vascular dysregulation
- Sleep apnoea
- Low night-time blood pressure
- Thin corneas
These associations do not prove the diagnosis by themselves.
Other causes of optic-nerve damage may need to be excluded when the appearance or progression is atypical.
Primary Angle-Closure Disease
In angle-closure disease, the peripheral iris narrows or blocks access to the trabecular meshwork.
This can prevent aqueous fluid from reaching the normal drainage pathway.
Angle-closure disease exists on a spectrum:
- Primary angle-closure suspect: the angle is narrow, but pressure and optic nerve remain normal.
- Primary angle closure: the narrow angle has caused pressure elevation, adhesions or other evidence of obstruction.
- Primary angle-closure glaucoma: angle closure has produced glaucomatous optic-nerve damage.
Angle closure can be chronic and silent or sudden and painful.
People of East Asian ancestry have a clinically important burden of angle-closure disease, making gonioscopy and anterior-chamber assessment particularly relevant in Singapore.
What Is Acute Angle-Closure Glaucoma?
Acute angle closure occurs when the drainage angle closes suddenly and eye pressure rises rapidly.
Symptoms may include:
- Severe eye pain
- A red eye
- Sudden blurred vision
- Halos around lights
- Headache
- Nausea
- Vomiting
- A poorly reactive or enlarged pupil
- A cloudy cornea
This is an eye emergency.
Without prompt treatment, severe and permanent optic-nerve damage can develop within a short time.
A painful red eye with headache, nausea and blurred vision should not be treated as ordinary conjunctivitis or migraine without an eye examination.
Can Angle Closure Occur Without Pain?
Yes.
Chronic or intermittent angle closure may occur with:
- No symptoms
- Mild intermittent blur
- Halos in dim lighting
- Brow ache
- Short episodes of eye discomfort
- Gradually increasing pressure
- Progressive optic-nerve damage
A patient can therefore have angle-closure glaucoma without ever experiencing a dramatic acute attack.
What Is Secondary Glaucoma?
Secondary glaucoma develops because another eye condition, injury, medication or procedure disrupts aqueous drainage or damages the optic nerve.
Possible causes include:
- Steroid use
- Eye trauma
- Uveitis
- Advanced diabetic eye disease
- Retinal vein occlusion
- Abnormal iris blood vessels
- Previous eye surgery
- Lens dislocation
- Pigment dispersion
- Pseudoexfoliation
- Corneal transplantation
- Tumours
- Severe inflammation
- Certain congenital abnormalities
Treatment must address both:
- The pressure
- The underlying cause
Secondary glaucoma can sometimes progress rapidly and may be more difficult to control than uncomplicated primary glaucoma.
Can Steroid Medication Cause Glaucoma?
Yes.
Steroids may raise eye pressure in susceptible individuals.
This can occur with:
- Steroid eye drops
- Steroid ointment around the eyes
- Oral steroids
- Inhaled steroids
- Nasal sprays
- Steroid injections
- Skin creams used near the eyelids
- Long-term systemic treatment
The risk depends on:
- Steroid strength
- Dose
- Duration
- Route of administration
- Individual susceptibility
- Existing glaucoma
- Family history
- Age
Steroid eye drops should not be self-started or continued indefinitely without pressure monitoring.
Patients should not stop medically necessary systemic steroids abruptly, but should inform the prescribing doctor and ophthalmologist.
Can Eye Trauma Cause Glaucoma?
Yes.
Blunt trauma may damage the drainage angle, a condition called angle recession.
Pressure elevation may occur:
- Immediately
- Months later
- Years or decades after the injury
Trauma may also cause glaucoma through:
- Bleeding inside the eye
- Lens damage
- Inflammation
- Scarring
- Steroid treatment
- Abnormal blood vessels
A history of significant eye injury remains relevant even when the incident occurred many years earlier.
What Is Pseudoexfoliative Glaucoma?
Pseudoexfoliation syndrome causes abnormal fibrillar material to accumulate on structures inside the eye.
It may be associated with:
- High and fluctuating eye pressure
- Poor pupil dilation
- Weakness of the lens-supporting fibres
- Faster glaucoma progression
- Greater complexity during cataract surgery
Not everyone with pseudoexfoliation develops glaucoma, but regular monitoring is important.
What Is Pigmentary Glaucoma?
Pigment dispersion occurs when pigment rubs from the back of the iris and accumulates within the drainage system.
It may cause:
- Elevated or fluctuating pressure
- Pigment in the trabecular meshwork
- Characteristic iris changes
- Glaucomatous optic-nerve damage
It is more commonly recognised in younger or middle-aged myopic adults.
What Is Neovascular Glaucoma?
Neovascular glaucoma develops when abnormal blood vessels grow over the iris and drainage angle.
Possible underlying causes include:
- Proliferative diabetic retinopathy
- Central retinal vein occlusion
- Severe retinal ischaemia
- Ocular ischaemic syndrome
The abnormal vessels can scar and pull the drainage angle closed.
Neovascular glaucoma may cause:
- Very high pressure
- Severe pain
- Redness
- Visual loss
- A poor response to ordinary drops
Treatment may require:
- Retinal laser
- Anti-VEGF injections
- Pressure-lowering medication
- Glaucoma surgery
- Treatment of the underlying vascular disease
Can Children Develop Glaucoma?
Yes, although childhood glaucoma is uncommon.
Types include:
- Primary congenital glaucoma
- Juvenile open-angle glaucoma
- Glaucoma associated with developmental abnormalities
- Glaucoma following cataract surgery
- Glaucoma related to inflammation, trauma or steroid use
Symptoms in infants may include:
- Excessive tearing
- Light sensitivity
- Eyelid squeezing
- Cloudy corneas
- Enlarged eyes
Older children may have few symptoms.
Childhood glaucoma often requires surgery and specialist long-term follow-up.
What Symptoms Does Chronic Glaucoma Cause?
Early open-angle glaucoma usually produces no noticeable symptoms.
As disease progresses, patients may experience:
- Missing areas in the peripheral vision
- Difficulty navigating crowded spaces
- Bumping into objects
- Difficulty locating steps or kerbs
- Reduced contrast
- Poorer vision in dim lighting
- Trouble driving
- Delayed adjustment between bright and dark environments
- Tunnel vision
- Central visual loss in advanced disease
Patients do not always perceive the loss as a black patch.
The brain may fill in missing information, creating an apparently complete but inaccurate scene.
Does Glaucoma Cause Blurred Vision?
It can, but blurred vision is not usually the first symptom of chronic open-angle glaucoma.
Blur may result from:
- Advanced visual-field damage
- Acute pressure elevation
- Corneal swelling
- Cataract
- Dry eye from glaucoma drops
- An incorrect spectacle prescription
- Another eye disease
A person can have severe glaucoma while maintaining 6/6 or 20/20 central visual acuity.
Does Glaucoma Cause Pain?
Most chronic glaucoma is painless.
Pain is more suggestive of:
- Acute angle closure
- Severe pressure elevation
- Inflammation
- Corneal disease
- Neovascular glaucoma
- Postoperative complications
- Another ocular condition
The absence of pain does not exclude glaucoma.
Does Glaucoma Always Affect Both Eyes?
Primary glaucoma commonly affects both eyes, but often asymmetrically.
One eye may have:
- Higher pressure
- Greater optic-nerve damage
- Faster progression
- More advanced visual-field loss
Secondary glaucoma may affect only one eye when related to:
- Trauma
- Surgery
- Inflammation
- Vascular disease
- A local eye condition
Both eyes should still be assessed because the apparently unaffected eye may have its own risk factors.
Who Is at Higher Risk of Glaucoma?
Important risk factors include:
- Increasing age
- Elevated eye pressure
- Family history of glaucoma
- Thin central cornea
- Suspicious optic-nerve appearance
- High myopia
- Narrow drainage angles
- Previous eye trauma
- Long-term steroid use
- Diabetes and vascular disease in selected contexts
- Previous eye surgery
- Certain ethnic backgrounds
- Existing glaucoma in the other eye
Risk factors do not prove that glaucoma is present.
They help determine who needs closer examination and monitoring.
How Important Is Family History?
A first-degree relative with glaucoma increases risk.
This includes an affected:
- Parent
- Sibling
- Child
Risk may be particularly important when the family member:
- Developed glaucoma at a young age
- Had severe or rapidly progressive disease
- Required glaucoma surgery
- Became visually impaired
- Had angle-closure glaucoma
Family members should know the specific diagnosis when possible because “glaucoma” includes several different conditions.
Can High Myopia Increase Glaucoma Risk?
Yes.
Moderate and high myopia are associated with a higher risk of open-angle glaucoma.
Myopic optic nerves can also be difficult to interpret because they may naturally appear:
- Tilted
- Large
- Shallowly cupped
- Surrounded by peripapillary atrophy
- Abnormal on OCT reference databases
Myopia can therefore both increase risk and complicate diagnosis.
LASIK, SMILE, PRK or ICL surgery corrects the focusing error but does not remove the glaucoma risk associated with the original long myopic eye.
Previous corneal laser surgery may also cause standard pressure measurements to underestimate the true pressure.
Does Long-Sightedness Increase Risk?
Long-sighted or hyperopic eyes are often shorter and may have shallower anterior chambers.
This can increase the likelihood of narrow drainage angles and angle-closure disease.
Not every long-sighted patient has narrow angles, and angle closure can also occur in eyes without a high hyperopic prescription.
Anatomical examination is required.
Does Diabetes Cause Glaucoma?
Diabetes is associated with several eye complications.
It may increase glaucoma risk in some populations and can cause neovascular glaucoma when diabetic retinopathy becomes severely ischaemic.
Diabetes does not mean that a patient automatically has glaucoma.
People with diabetes require regular retinal and general eye assessment.
Does Blood Pressure Affect Glaucoma?
The relationship is complex.
High blood pressure, low blood pressure and excessive night-time blood-pressure reduction may each influence optic-nerve perfusion in different circumstances.
Patients should not alter blood-pressure treatment without consulting their physician.
A glaucoma patient who experiences:
- Fainting
- Very low morning pressure
- Night-time dizziness
- Aggressive blood-pressure treatment
- Sleep apnoea
should discuss these factors with the relevant doctors.
Can Sleep Apnoea Be Associated with Glaucoma?
Obstructive sleep apnoea has been associated with glaucoma and optic-nerve changes in observational studies.
Possible mechanisms include:
- Repeated low oxygen levels
- Vascular dysregulation
- Changes in pressure around the optic nerve
- Night-time blood-pressure changes
This does not mean that every patient with sleep apnoea will develop glaucoma.
Symptoms such as loud snoring, witnessed pauses in breathing and severe daytime sleepiness should be assessed for general health reasons.
How Is Glaucoma Diagnosed?
No single test diagnoses every case.
A glaucoma assessment usually combines:
- Eye-pressure measurement
- Optic-nerve examination
- OCT
- Visual-field testing
- Gonioscopy
- Corneal-thickness measurement
- Optic-disc photography
- Review of progression over time
Eye-Pressure Measurement
Pressure may be measured using:
- Goldmann applanation tonometry
- Non-contact air-puff tonometry
- Handheld tonometry
- Rebound tonometry
- Other specialised devices
Goldmann applanation remains a standard clinical method.
Pressure varies with:
- Time of day
- Eyelid squeezing
- Breath holding
- Body position
- Corneal thickness
- Corneal biomechanics
- Medication use
- Recent exercise
- Measurement technique
One normal pressure reading cannot exclude glaucoma.
Why Does Corneal Thickness Matter?
Pressure is estimated by measuring how the cornea responds to force.
A thicker or biomechanically stiffer cornea may produce a higher measured pressure.
A thinner cornea may produce a lower reading.
Central corneal thickness also contributed to risk prediction in the Ocular Hypertension Treatment Study.
Pachymetry helps interpret pressure and overall risk, but there is no universally reliable formula that converts the measured pressure into a perfectly “corrected” pressure.
What Is Gonioscopy?
Gonioscopy examines the drainage angle using a mirrored contact lens placed gently on the numbed eye.
It determines whether the angle is:
- Open
- Narrow
- Closed
- Scarred
- Abnormally pigmented
- Damaged by trauma
- Blocked by abnormal vessels
- Affected by adhesions
This test is essential for distinguishing open-angle from angle-closure disease.
A normal external eye appearance does not reveal whether the internal drainage angle is narrow.
What Is Optic-Nerve Cupping?
The centre of the optic nerve contains a depression called the cup.
Glaucoma can cause the cup to enlarge as nerve tissue is lost.
The cup-to-disc ratio describes the relationship between the cup and the overall optic-disc size.
A large cup does not automatically mean glaucoma because:
- Large optic nerves naturally have larger cups.
- Small optic nerves may develop glaucoma with a relatively small cup.
- Myopic nerves can have unusual shapes.
- Congenital anatomy varies.
More concerning features include:
- Progressive enlargement
- Thinning or notching of the neural rim
- Asymmetry between eyes
- Retinal nerve-fibre defects
- Optic-disc haemorrhage
- Corresponding OCT or visual-field loss
What Is Optical Coherence Tomography?
Optical coherence tomography, or OCT, uses light to produce detailed cross-sectional images of the retina and optic nerve.
It measures structures including:
- Peripapillary retinal nerve-fibre layer
- Macular ganglion-cell complex
- Optic-nerve head
- Neuroretinal rim
OCT can detect structural damage before the patient notices symptoms.
However, an OCT result is not a diagnosis by itself.
False abnormalities may occur because of:
- High myopia
- Tilted optic nerves
- Segmentation errors
- Poor scan quality
- Retinal disease
- Unusual but healthy anatomy
- Reference-database limitations
Progression analysis using repeat high-quality scans is often more valuable than one colour-coded report.
What Is a Visual-Field Test?
Automated perimetry measures how sensitive different areas of the visual field are.
The patient looks at a central target and presses a button when small lights are seen.
Glaucoma may cause patterns such as:
- Nasal steps
- Paracentral defects
- Arcuate scotomas
- Peripheral constriction
- Advanced central islands
The test requires concentration and learning.
An unreliable or abnormal first test may need to be repeated before being interpreted.
Visual-field testing measures function, while OCT measures structure. Both are important because one may show change before the other.
Why Are Optic-Disc Photographs Useful?
Photographs create a permanent record of the optic nerve.
They can document:
- Cup size
- Rim appearance
- Disc haemorrhage
- Peripapillary changes
- Long-term structural progression
Photographs are particularly helpful when OCT measurements are difficult to interpret, such as in highly myopic eyes.
Why Are Repeated Tests Necessary?
Glaucoma is diagnosed and managed by looking for a consistent pattern over time.
Tests have natural variability.
A single abnormal result may reflect:
- Poor concentration
- Dry eye
- Cataract
- Scan misalignment
- Incorrect refraction
- Instrument error
- Unusual anatomy
Repeated testing helps determine whether a finding is:
- Reproducible
- Progressive
- Consistent with glaucoma
- Stable and non-glaucomatous
How Often Should People Be Screened?
The interval depends on individual risk.
More frequent examinations may be appropriate for people with:
- A family history of glaucoma
- Elevated pressure
- Narrow angles
- High myopia
- Previous eye trauma
- Long-term steroid exposure
- Diabetes
- Suspicious optic nerves
- Age over 40
- Previous glaucoma findings
A routine spectacle test that checks only visual acuity and prescription may not include the full glaucoma assessment.
Patients should ask whether their examination includes:
- Eye pressure
- Optic-nerve evaluation
- Dilated retinal assessment when appropriate
- Additional testing when risk is present
Can Glaucoma Be Cured?
Glaucoma is usually controlled rather than cured.
Current treatment can:
- Lower eye pressure
- Reduce the risk of further optic-nerve damage
- Slow progression
- Preserve remaining vision
Treatment cannot usually:
- Regenerate lost optic-nerve fibres
- Restore established visual-field defects
- Permanently eliminate the need for monitoring
- Guarantee that progression will never occur
Many patients retain useful vision throughout life when the disease is detected early, pressure is adequately lowered and follow-up is consistent.
What Is the Goal of Glaucoma Treatment?
The goal is to lower eye pressure enough to reduce the rate of further damage.
This pressure level is called the target pressure.
The target depends on:
- Starting pressure
- Severity of damage
- Age and life expectancy
- Rate of progression
- Pressure in the fellow eye
- Corneal thickness
- Other risk factors
- Treatment risks
- Visual needs
The 2025 American Academy of Ophthalmology guideline describes an initial reduction of approximately 20% to 30% from baseline as reasonable for many patients with primary open-angle glaucoma, followed by adjustment according to the disease course. Advanced or rapidly progressing disease may require a lower target.
How Is Glaucoma Treated?
Treatment may involve:
- Eye drops
- Laser treatment
- Surgery
- A combination of methods
The choice depends on:
- Type of glaucoma
- Disease severity
- Target pressure
- Current medication
- Age
- Lens status
- Corneal health
- Previous surgery
- Ability to use drops
- Lifestyle
- Patient preference
Glaucoma Eye Drops
Glaucoma drops lower pressure by:
- Reducing fluid production
- Increasing fluid drainage
- Using both mechanisms
Common medication classes include:
- Prostaglandin analogues
- Beta blockers
- Alpha-adrenergic agonists
- Carbonic anhydrase inhibitors
- Rho-kinase inhibitors
- Combination preparations
Drops do not improve vision immediately and may not produce any sensation that confirms they are working.
Their benefit is preventive.
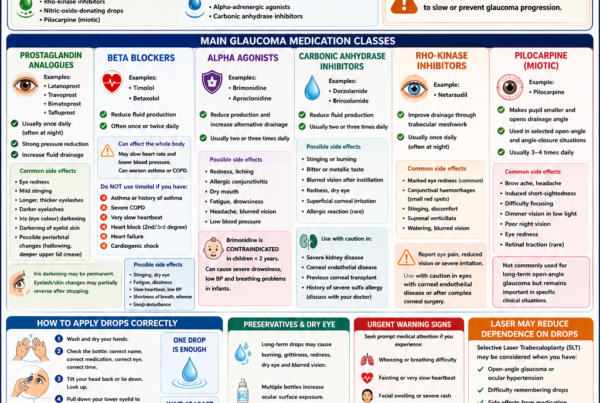
Prostaglandin Analogues
Examples include:
- Latanoprost
- Travoprost
- Bimatoprost
- Tafluprost
These are commonly used once at night and increase aqueous drainage.
Possible side effects include:
- Eye redness
- Darkening of the iris
- Darker eyelid skin
- Longer eyelashes
- Deepening around the eyelids
- Mild irritation
- Rare inflammation or macular swelling in susceptible eyes
Iris darkening may be permanent.
Beta-Blocker Drops
Timolol is a commonly used beta blocker.
It reduces aqueous-fluid production.
Possible side effects include:
- Slow heart rate
- Low blood pressure
- Fatigue
- Dizziness
- Breathing difficulty
- Worsening asthma
- Reduced exercise tolerance
- Masking low blood sugar symptoms
Patients should inform the ophthalmologist about:
- Asthma
- Chronic lung disease
- Heart block
- Slow pulse
- Heart failure
- Other beta-blocker medication
Eye drops can have effects beyond the eye.
Alpha-Adrenergic Agonists
Brimonidine reduces fluid production and increases drainage.
Possible side effects include:
- Redness
- Dry mouth
- Fatigue
- Drowsiness
- Eyelid allergy
- Low blood pressure
It may cause marked sleepiness in young children and is generally avoided in infants and very young children.
Carbonic Anhydrase Inhibitors
Examples include:
- Dorzolamide
- Brinzolamide
They reduce aqueous production.
Possible side effects include:
- Stinging
- Blurred vision
- Bitter taste
- Eye irritation
- Corneal problems in susceptible eyes
Oral carbonic anhydrase inhibitors such as acetazolamide may be used for severe pressure elevation but can cause more systemic effects.
Rho-Kinase Inhibitors
These medications improve drainage through the trabecular pathway.
Possible side effects include:
- Significant eye redness
- Small corneal deposits
- Subconjunctival haemorrhage
- Stinging
- Corneal epithelial changes in susceptible patients
Availability varies between countries.
How Should Glaucoma Drops Be Applied?
A useful technique is:
- Wash and dry the hands.
- Check the bottle label.
- Tilt the head back.
- Pull the lower eyelid down gently.
- Instil one drop without touching the eye.
- Close the eyelids gently.
- Press the inner corner of the eyelids beside the nose for one to two minutes.
- Wipe away excess medication.
- Wait approximately five to ten minutes before using another drop.
Only one drop is needed.
The eye cannot hold several drops at once, and excess medication increases waste and systemic absorption.
What If I Miss a Dose?
Use the drop when remembered unless it is almost time for the next dose.
Do not repeatedly double the dose.
An occasional missed dose is unlikely to cause sudden blindness, but frequent missed doses can allow pressure to remain above target and increase long-term risk.
Patients who struggle with adherence should discuss:
- Simpler dosing
- Combination drops
- Reminder systems
- Laser treatment
- Assistance from family
- Bottle aids
Can Preservatives Cause Dry Eye?
Yes.
Long-term glaucoma drops—especially multiple preserved medications—may cause or worsen:
- Burning
- Grittiness
- Redness
- Tear-film instability
- Eyelid inflammation
- Corneal staining
- Allergy
Options may include:
- Preservative-free formulations
- Reducing the number of bottles
- Combination drops
- Selective laser trabeculoplasty
- Ocular-surface treatment
- Surgery when clinically appropriate
Patients should not stop pressure-lowering treatment without arranging an alternative plan.
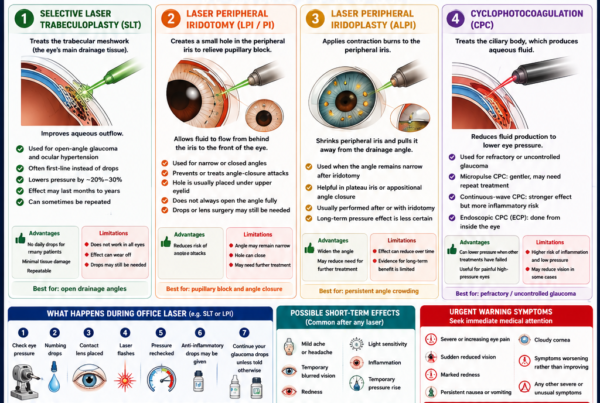
What Is Selective Laser Trabeculoplasty?
Selective laser trabeculoplasty, or SLT, treats the trabecular meshwork in open-angle glaucoma.
The laser stimulates biological changes that improve aqueous drainage.
The procedure is usually performed in the clinic.
Advantages include:
- No incision
- Minimal discomfort
- Reduced reliance on daily drops
- Repeatability in selected patients
- Avoidance of medication side effects
The LiGHT trial showed that SLT is a safe and effective first-line treatment for open-angle glaucoma and ocular hypertension. Six-year follow-up found strong long-term disease control and less need for incisional glaucoma surgery than an initial drop-based pathway.
Does SLT Work Permanently?
Not always.
The pressure-lowering effect may last:
- Months
- Several years
- Longer in some eyes
The effect can gradually diminish.
SLT may sometimes be repeated, although the response is not guaranteed.
Some patients still require drops or surgery.
What Is Laser Peripheral Iridotomy?
Laser peripheral iridotomy, or LPI, creates a small opening in the peripheral iris.
It allows aqueous fluid to pass more directly from behind the iris into the anterior chamber, reducing pressure differences that push the iris towards the drainage angle.
LPI is commonly used for:
- Pupillary-block angle closure
- Acute angle closure after initial pressure control
- Selected narrow-angle eyes at significant risk
- The fellow eye after an acute angle-closure attack
LPI does not necessarily open every narrow angle completely.
Some patients continue to require:
- Pressure-lowering drops
- Lens extraction
- Goniosynechialysis
- Glaucoma surgery
- Long-term monitoring
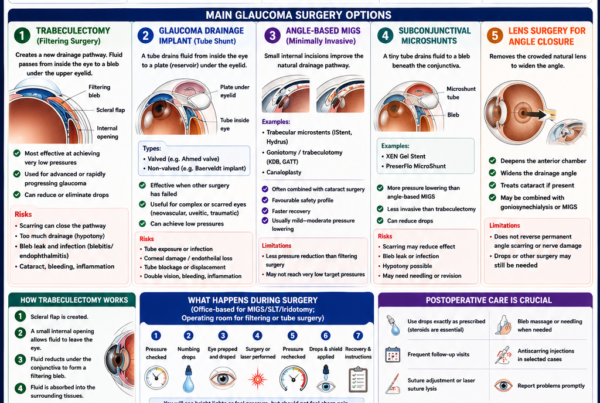
Can Cataract Surgery Help Angle Closure?
Yes.
The natural lens becomes thicker with age and can crowd the front of the eye.
Removing the lens and replacing it with a thinner artificial lens generally deepens the anterior chamber and widens the drainage angle.
Lens extraction may be considered when:
- A visually significant cataract is present
- The angle remains crowded
- Pressure is difficult to control
- There has been angle closure
- The lens is an important anatomical contributor
Cataract surgery may lower pressure, but it does not reverse established optic-nerve damage.
When Is Glaucoma Surgery Needed?
Surgery may be recommended when:
- Drops and laser do not achieve the target pressure
- Disease continues progressing
- Glaucoma is advanced
- Pressure is extremely high
- Medication cannot be tolerated
- Adherence is unreliable
- Secondary glaucoma requires stronger intervention
- The optic nerve is at immediate risk
Trabeculectomy
Trabeculectomy creates a new drainage pathway from inside the eye to a filtering reservoir beneath the upper eyelid.
It can achieve low pressures and remains an important treatment for advanced glaucoma.
Possible complications include:
- Very low pressure
- Bleeding
- Infection
- Scarring and surgical failure
- Cataract progression
- Choroidal detachment
- Persistent blurred vision
- Rare severe visual loss
Long-term monitoring remains essential because filtering blebs can develop late infections.
Glaucoma Drainage Implants
A glaucoma drainage implant uses a small tube connected to a plate placed beneath the conjunctiva.
Fluid passes through the tube to a reservoir around the plate.
Tube surgery may be considered for:
- Complex glaucoma
- Previous failed trabeculectomy
- Neovascular glaucoma
- Uveitic glaucoma
- Significant conjunctival scarring
- Selected primary glaucoma cases
Possible complications include:
- Tube blockage
- Tube exposure
- Corneal endothelial damage
- Double vision
- Low pressure
- Bleeding
- Infection
- Need for revision
Minimally Invasive Glaucoma Surgery
Minimally invasive glaucoma surgery, or MIGS, includes several procedures designed to improve drainage with less tissue disruption than traditional filtering surgery.
MIGS may be performed:
- Alone
- More commonly with cataract surgery
Advantages may include:
- Faster recovery
- Lower risk of severe pressure reduction
- Reduced medication burden
- A favourable safety profile for selected patients
Limitations include:
- Less dramatic pressure lowering than trabeculectomy
- Variable suitability by glaucoma type
- Limited effectiveness in advanced disease
- Possible need for continued drops
- Device-specific risks
MIGS is not one single operation. The expected pressure reduction depends on the particular procedure.
Cyclodestructive Treatment
Cyclophotocoagulation reduces aqueous production by treating part of the ciliary body.
Techniques include:
- Continuous-wave transscleral treatment
- Micropulse treatment
- Endoscopic cyclophotocoagulation
It may be used for:
- Refractory glaucoma
- Painful blind eyes
- Eyes unsuitable for filtering surgery
- Selected eyes with useful vision
- Combination procedures
The safety and expected effect differ between techniques.
Can Surgery Cure Glaucoma?
No.
Surgery lowers pressure but does not regenerate the optic nerve or permanently remove the need for follow-up.
After apparently successful surgery:
- Pressure can rise again.
- Scar tissue can form.
- Additional drops may be required.
- Another procedure may become necessary.
- Visual-field and OCT monitoring must continue.
Can Lost Vision Be Restored?
Established glaucomatous optic-nerve damage is generally irreversible.
Current treatment aims to protect the vision that remains.
A patient may notice improved vision after:
- New spectacles
- Cataract surgery
- Treatment of dry eye
- Relief of corneal swelling
- Pressure reduction after acute angle closure
This improvement does not mean that damaged optic-nerve fibres have regenerated.
Research into neuroprotection and nerve regeneration continues, but lowering eye pressure remains the only established treatment strategy proven to modify glaucoma progression.
Can Glaucoma Progress Despite a Normal Clinic Pressure?
Yes.
Possible reasons include:
- The target pressure is lower than the measured pressure.
- Pressure peaks occur at another time of day.
- Medication effect wears off before the next dose.
- Drops are not entering the eye consistently.
- Normal-tension glaucoma is progressing.
- Structural change reflects earlier pressure exposure.
- Another optic-nerve condition is present.
- The measurement underestimates pressure.
The target pressure may need to be lowered when OCT or visual fields show confirmed progression.
What Does “Stable Glaucoma” Mean?
Stable glaucoma means that available testing does not show clinically significant progression over the observed period.
It does not mean that the disease has disappeared.
Continued follow-up is required because:
- Pressure may change.
- Medication effect may reduce.
- Adherence may alter.
- Age-related risk may increase.
- Progression may resume.
- Tests may only detect change after several visits.
How Often Should a Patient with Glaucoma Be Reviewed?
The interval depends on:
- Disease severity
- Current pressure
- Target pressure
- Rate of progression
- Treatment changes
- Reliability of testing
- Glaucoma type
- Other eye conditions
A stable low-risk patient may be reviewed less frequently than someone with:
- Advanced disease
- Recent progression
- A new medication
- A recent laser procedure
- Recent surgery
- Very high pressure
- Visual-field damage near fixation
Patients should attend even when vision feels unchanged.
Can Glaucoma Affect Driving?
Yes.
Glaucoma may impair:
- Peripheral awareness
- Hazard detection
- Night driving
- Contrast sensitivity
- Lane positioning
- Ability to detect pedestrians or vehicles approaching from the side
A patient can have good central visual acuity but still have an unsafe visual field.
Driving fitness depends on:
- Vision in both eyes
- Extent of binocular visual-field loss
- Local licensing requirements
- Other eye conditions
- Actual functional ability
Patients with advanced glaucoma may require binocular field testing such as an Esterman visual field.
Can Exercise Help Glaucoma?
Regular moderate exercise may produce a temporary reduction in eye pressure and benefits general cardiovascular health.
Suitable activities may include:
- Walking
- Jogging
- Cycling
- Swimming
- Moderate aerobic exercise
Exercise does not replace glaucoma treatment.
Certain activities may temporarily raise pressure, including:
- Prolonged breath holding
- Heavy straining
- Inverted yoga positions
- Tight swimming goggles
- Playing wind instruments at high resistance
Most patients do not need to avoid ordinary exercise, but those with advanced or unstable glaucoma should ask for individual advice.
Does Drinking Water Affect Eye Pressure?
Normal hydration is appropriate.
Rapidly drinking a very large volume of water can temporarily raise eye pressure in some people.
There is generally no need to restrict ordinary fluid intake unless advised for another medical condition.
Spreading fluid intake throughout the day is reasonable.
Does Coffee Increase Eye Pressure?
Caffeine may produce a small temporary pressure rise in some individuals.
For most patients, moderate coffee consumption is not the main factor determining glaucoma control.
Patients with very high or unstable pressure may discuss heavy caffeine intake with their ophthalmologist.
Can Diet Cure Glaucoma?
No food, vitamin or supplement has been proven to cure glaucoma or replace pressure-lowering treatment.
A balanced diet supports general health.
Patients should be cautious about products claiming to:
- Regenerate the optic nerve
- Dissolve glaucoma
- Replace eye drops
- Restore lost visual fields
- Lower pressure permanently
Some supplements can interact with medication or increase bleeding risk.
Is Marijuana a Glaucoma Treatment?
Marijuana can temporarily lower eye pressure, but the effect lasts only a few hours.
Maintaining continuous pressure control would require repeated use throughout the day and night, causing substantial cognitive, cardiovascular and functional side effects.
It is not considered a practical or recommended glaucoma treatment.
Can Screen Use Cause Glaucoma?
Ordinary computer, tablet and smartphone use does not cause glaucoma.
Screens may contribute to:
- Dry eye
- Eye strain
- Headache
- Temporary blur
These symptoms are not evidence of optic-nerve damage.
Glaucoma patients can generally use screens according to comfort and visual ability.
Does Wearing Glasses Prevent Glaucoma?
No.
Glasses correct refractive error but do not lower eye pressure or protect the optic nerve.
A patient may have excellent vision with glasses and still have glaucoma.
Does Cataract Cause Glaucoma?
An ordinary age-related cataract does not usually cause open-angle glaucoma.
However, a large or abnormal lens can contribute to:
- Angle closure
- Lens-induced inflammation
- Lens-particle glaucoma
- Severe pressure elevation in selected cases
Glaucoma and cataract commonly coexist because both become more frequent with age.
Is Glaucoma the Same as Cataract?
No.
Cataract
- Clouding of the natural lens
- Causes blur, glare and faded colours
- Usually treated by replacing the cloudy lens
- Vision can often improve substantially after surgery
Glaucoma
- Progressive optic-nerve damage
- Often affects peripheral vision first
- Usually cannot be reversed
- Requires pressure lowering and lifelong monitoring
A person can have both conditions.
Can Glaucoma Cause Blindness Even with Treatment?
Yes, but treatment substantially reduces the risk.
Vision may still deteriorate when:
- Disease was advanced at diagnosis
- The target pressure is not achieved
- Progression is unusually aggressive
- Follow-up is inconsistent
- Medication is not used reliably
- Pressure fluctuates widely
- Surgery fails or complications develop
- Other eye diseases coexist
Early diagnosis offers the greatest opportunity to preserve lifelong vision.
Why Might One Patient Need Treatment While Another Is Observed?
Treatment is based on risk and demonstrated damage.
A patient may be observed when:
- Pressure is mildly elevated.
- The optic nerves appear healthy.
- OCT and fields remain normal.
- Overall conversion risk is low.
Another patient may need immediate treatment despite a lower pressure because:
- Definite damage is present.
- Disease is progressing.
- Visual-field loss is close to fixation.
- The patient is young.
- The fellow eye is severely affected.
- The optic nerve is especially vulnerable.
The pressure number must always be interpreted in context.
Frequently Asked Questions
Is glaucoma always caused by high eye pressure?
No.
High pressure is the most important modifiable risk factor, but glaucoma can develop at statistically normal pressure.
Does high eye pressure always mean glaucoma?
No.
Ocular hypertension means the pressure is elevated without definite optic-nerve damage.
Can I feel when my pressure is high?
Usually not.
Moderately elevated pressure is often completely painless.
Can an air-puff test diagnose glaucoma?
No.
It can screen pressure, but glaucoma diagnosis requires optic-nerve and visual-function assessment.
Is glaucoma contagious?
No.
It cannot spread between people.
Is glaucoma hereditary?
It can run in families, although inheritance is complex.
Close relatives should consider regular eye assessment.
Can young adults develop glaucoma?
Yes.
Possible causes include:
- Juvenile open-angle glaucoma
- Steroid response
- Trauma
- Pigment dispersion
- Uveitis
- Congenital or developmental abnormalities
Can children inherit glaucoma from their parents?
Some childhood and juvenile glaucomas have genetic components.
Most children of adults with common age-related glaucoma will not develop childhood glaucoma, but may have higher lifetime risk.
Can glaucoma make the eye look different?
Most chronic glaucoma causes no visible external change.
Acute angle closure or advanced secondary glaucoma may cause redness, corneal clouding or pupil changes.
Why is my pressure different at each visit?
Pressure naturally fluctuates and may be influenced by time of day, medication timing, body position, corneal factors and measurement technique.
Why is my pressure higher in one eye?
The eyes may differ in:
- Drainage efficiency
- Anatomy
- Previous trauma
- Steroid response
- Surgical history
- Glaucoma type
Repeated asymmetry may be clinically important.
Why do I need both OCT and visual-field tests?
OCT measures structural nerve tissue.
The visual field measures how the nerve damage affects vision.
They provide complementary information.
Can OCT replace a visual-field test?
No.
A normal OCT does not exclude every functional defect, and an abnormal OCT may be caused by anatomy or scan error.
Why do I need repeated visual fields?
The first test may be affected by unfamiliarity or poor concentration.
Several tests help establish a reliable baseline and determine the rate of change.
Can I stop drops after laser treatment?
Some patients can reduce or stop drops after successful SLT, while others must continue them.
Only stop medication when instructed.
Can I stop drops after glaucoma surgery?
Sometimes, but not always.
The need for medication depends on postoperative pressure and target.
What if my drops make my eyes red?
Do not stop them without advice.
Options may include a different drug, preservative-free drops, laser or surgery.
Can glaucoma drops change eye colour?
Prostaglandin analogues may gradually darken the iris, particularly in hazel or mixed-colour eyes.
Why are my eyelashes longer?
Prostaglandin medications can stimulate eyelash growth.
Can glaucoma drops affect breathing?
Beta-blocker drops may worsen asthma or certain lung conditions.
Can glaucoma drops affect the heart?
Some drops can slow the heart rate or lower blood pressure.
All current medication and medical conditions should be disclosed.
Why press the corner of the eye after using drops?
This reduces drainage into the nose and may limit systemic absorption.
Can glaucoma improve?
Pressure control can improve, and progression may stop or slow.
Existing optic-nerve damage usually remains.
Can acupuncture, massage or eye exercises treat glaucoma?
No established evidence shows that these methods provide reliable long-term pressure control or prevent optic-nerve damage.
Should I avoid flying?
Ordinary commercial air travel is generally safe for stable glaucoma.
Different advice applies after certain eye surgeries involving an intraocular gas bubble.
Can I dive?
Many patients with stable glaucoma can dive, but mask pressure, medication, previous surgery and disease severity should be discussed individually.
Can pregnancy affect glaucoma treatment?
Some glaucoma medications may be absorbed systemically and require modification during pregnancy or breastfeeding.
Treatment planning should involve the ophthalmologist and obstetric clinician.
Is glaucoma treatment lifelong?
Often, yes.
Even after laser or surgery, continued monitoring is required.
A Practical Glaucoma Assessment
A complete assessment may include:
Medical History
- Family history
- Previous trauma
- Steroid exposure
- Current medication
- Vascular conditions
- Sleep apnoea
- Migraine
- Previous surgery
- Symptoms of angle closure
Eye Examination
- Visual acuity
- Intraocular pressure
- Pupil assessment
- Slit-lamp examination
- Gonioscopy
- Dilated optic-nerve examination
- Corneal thickness
Structural Testing
- OCT retinal nerve-fibre layer
- Macular ganglion-cell analysis
- Optic-nerve photography
Functional Testing
- Standard automated visual field
- Alternative field strategies when required
- Binocular functional field testing for driving when indicated
Follow-Up Assessment
- Compare pressure with target.
- Assess medication adherence.
- Review side effects.
- Look for OCT progression.
- Review visual-field progression.
- Adjust treatment when necessary.
Warning Signs Requiring Urgent Eye Care
Seek urgent assessment for:
- Severe eye pain
- A red eye with blurred vision
- Halos around lights
- Headache with nausea or vomiting
- Sudden visual loss
- A cloudy cornea
- Rapid pupil change
- Sudden pain after glaucoma surgery
- Discharge or marked redness around a filtering bleb
- Trauma to an eye with previous glaucoma surgery
These symptoms may indicate acute angle closure, severe pressure elevation, infection or another sight-threatening condition.
The Bottom Line
Glaucoma is a group of diseases that progressively damage the optic nerve.
It is not defined by pressure alone.
A person may have:
- High pressure without glaucoma
- Glaucoma with normal pressure
- Open-angle glaucoma
- Angle-closure glaucoma
- Secondary glaucoma from another eye condition
- Childhood or congenital glaucoma
The most common chronic forms are painless and often cause no early symptoms.
Diagnosis requires a combination of:
- Eye-pressure measurement
- Optic-nerve assessment
- OCT
- Visual-field testing
- Gonioscopy
- Corneal-thickness measurement
- Observation for progression
Treatment lowers eye pressure through:
- Eye drops
- Laser treatment
- Cataract or lens surgery in selected angle-closure cases
- Trabeculectomy
- Glaucoma drainage implants
- MIGS
- Cyclophotocoagulation
Treatment cannot usually restore vision already lost, but early and sustained pressure control can preserve remaining sight.
Glaucoma is not simply a high pressure reading. It is progressive damage to the optic nerve—and because early disease is usually silent, regular eye examination is the key to detecting it before vision is permanently lost.
References
- American Academy of Ophthalmology. Primary Open-Angle Glaucoma Preferred Practice Pattern. 2025.
- American Academy of Ophthalmology. Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern. 2025.
- American Academy of Ophthalmology. Primary Angle-Closure Disease Preferred Practice Pattern. 2025.
- National Eye Institute. Glaucoma. Updated November 2025.
- National Eye Institute. Types of Glaucoma. Updated December 2024.
- National Eye Institute. Glaucoma and Eye Pressure. Updated December 2024.
- National Eye Institute. Glaucoma Medicines, Laser Treatment and Surgery. 2024–2025.
- Singapore HealthHub. Glaucoma.
- National Institute for Health and Care Excellence. Glaucoma: Diagnosis and Management. Reviewed March 2025.
- Gordon MO, et al. The Ocular Hypertension Treatment Study: Baseline Factors That Predict the Onset of Primary Open-Angle Glaucoma. Archives of Ophthalmology. 2002.
- Collaborative Normal-Tension Glaucoma Study Group. The Effectiveness of Intraocular Pressure Reduction in the Treatment of Normal-Tension Glaucoma. American Journal of Ophthalmology. 1998.
- Gazzard G, et al. Selective Laser Trabeculoplasty Versus Eye Drops for First-Line Treatment of Ocular Hypertension and Glaucoma: The LiGHT Trial. The Lancet. 2019.
- Gazzard G, et al. Laser in Glaucoma and Ocular Hypertension Trial: Six-Year Results. Ophthalmology. 2023.
- Baskaran M, et al. The Prevalence and Types of Glaucoma in an Urban Chinese Population: The Singapore Chinese Eye Study. JAMA Ophthalmology. 2015.
- Chua J, et al. The Singapore Epidemiology of Eye Diseases Study. Ophthalmology. 2015.