Author: Dr Val Phua
Estimated reading time: 11–13 minutes
Retinal Vein Occlusion Can Cause Sudden, Painless Blurred Vision
A retinal vein occlusion occurs when a vein carrying blood away from the retina becomes partially or completely blocked.
The resulting congestion may cause retinal bleeding, leakage of fluid, reduced oxygen supply and swelling of the macula—the part of the retina responsible for detailed central vision.
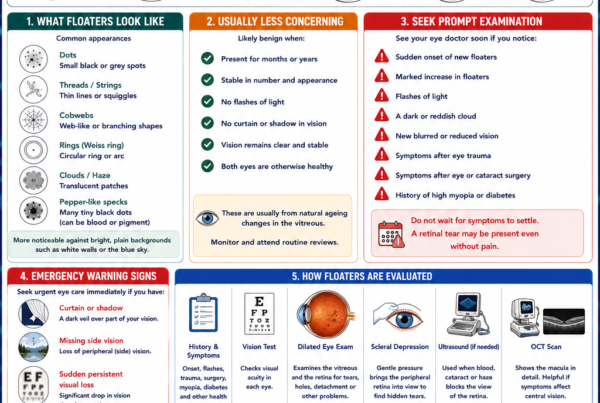
Common symptoms include:
- Sudden or gradual blurred vision
- Distorted central vision
- A dark or hazy area
- New floaters
- Reduced contrast or colour perception
- Sudden loss of vision in one eye
Retinal vein occlusion is usually painless and commonly affects only one eye. Prompt examination is important because early treatment of macular swelling can improve the likelihood of preserving useful vision, while more severe cases require monitoring for abnormal blood vessels and glaucoma.
What Is the Retina?
The retina is a thin layer of light-sensitive nerve tissue lining the back of the eye.
It converts light into electrical signals that travel through the optic nerve to the brain.
At the centre of the retina is the macula, which provides the detailed vision required for:
- Reading
- Recognising faces
- Driving
- Seeing colours
- Performing fine visual tasks
Retinal arteries carry oxygenated blood into the retina, while retinal veins drain blood away. If venous drainage is obstructed, pressure builds within the retinal circulation and the vessels may leak blood and fluid.
What Is a Retinal Vein Occlusion?
A retinal vein occlusion, or RVO, is an obstruction within the retinal venous system.
The blockage is generally associated with slowed blood flow and thrombus formation. The vein itself does not necessarily contain a large clot that can simply be removed.
The consequences depend on:
- Which vein is affected
- How completely it is blocked
- The area of retina involved
- Whether the macula becomes swollen
- How much retinal circulation is lost
- Whether abnormal new blood vessels develop
Some mild occlusions cause limited symptoms and may stabilise without ocular treatment. Others produce severe macular swelling, retinal ischaemia, bleeding or painful neovascular glaucoma.
The Main Types of Retinal Vein Occlusion
Branch Retinal Vein Occlusion
A branch retinal vein occlusion, or BRVO, occurs when one of the smaller retinal veins becomes blocked.
It commonly develops where a retinal artery crosses over a vein. Both vessels share a confined tissue sheath. When the artery becomes thickened and less flexible, it may compress the underlying vein, slowing blood flow and promoting obstruction.
BRVO usually affects one sector of the retina. Vision may remain normal if the affected area does not involve the macula, but macular leakage may produce central blur or distortion.
Central Retinal Vein Occlusion
A central retinal vein occlusion, or CRVO, occurs when the main vein draining the retina becomes obstructed.
Because this vein serves the entire retina, CRVO generally causes more widespread retinal haemorrhage, swelling and vascular congestion than BRVO.
CRVO may range from a relatively mild, non-ischaemic form to a severe ischaemic form with extensive loss of retinal circulation.
Hemi-Retinal Vein Occlusion
A hemi-retinal vein occlusion affects approximately half of the retinal circulation.
Its clinical behaviour may resemble either a large BRVO or CRVO, depending on the anatomy and degree of retinal ischaemia.
Non-Ischaemic Versus Ischaemic CRVO
Non-Ischaemic CRVO
This is the less severe and more common form.
Blood flow remains impaired, but sufficient retinal circulation is preserved. Vision may be affected mainly by macular oedema.
Some non-ischaemic occlusions improve or remain stable, although they require follow-up because retinal circulation can worsen over time.
Ischaemic CRVO
In ischaemic CRVO, a substantial area of the retina receives inadequate blood flow and oxygen.
Patients may have:
- More severe visual loss
- A relative afferent pupillary defect
- Extensive retinal haemorrhage
- Cotton-wool spots
- Marked venous congestion
- A higher risk of abnormal blood-vessel growth
- A higher risk of neovascular glaucoma
Anti-VEGF treatment may reduce macular oedema, but it does not restore retinal tissue that has already been permanently damaged by severe ischaemia. Close monitoring remains essential even when swelling improves.
What Symptoms Can Retinal Vein Occlusion Cause?
Blurred Vision
Blur is the most common symptom.
It may occur suddenly or develop over several hours or days. The severity varies from slight haziness to marked central visual loss.
Blur commonly results from macular oedema, in which damaged retinal vessels leak fluid into the central retina.
Distorted Vision
Straight lines may appear:
- Bent
- Wavy
- Broken
- Uneven
Words may look crowded or parts of letters may disappear.
Distortion usually indicates that swelling is affecting the structure of the macula.
A Dark or Hazy Area
Patients may notice a grey, dim or blurry area corresponding to the part of the retina affected by the occlusion.
With BRVO, this may involve only one portion of the field. CRVO may produce more generalised visual reduction.
Floaters
New dots, strands or cobweb-like shadows may develop if abnormal retinal blood vessels bleed into the vitreous gel.
Floaters may be the presenting symptom of a previously unnoticed occlusion that has subsequently developed neovascularisation.
Sudden Severe Visual Loss
Marked visual loss may result from:
- Severe macular oedema
- Extensive retinal ischaemia
- Vitreous haemorrhage
- Retinal detachment
- Neovascular glaucoma
- Another simultaneous eye condition
Sudden or profound visual loss should be assessed promptly rather than waiting for a routine appointment.
Eye Pain and Redness
Most retinal vein occlusions are painless.
Pain, redness, headache or nausea may develop if abnormal blood vessels obstruct the eye’s drainage system and cause neovascular glaucoma.
A painful red eye with reduced vision is urgent.
Can Retinal Vein Occlusion Cause No Symptoms?
Yes.
A small BRVO that does not affect the macula may be discovered during a routine retinal examination.
Even an asymptomatic occlusion warrants medical risk-factor assessment and appropriate retinal monitoring because complications may develop later.
When Should I Seek Eye Care?
Arrange prompt ophthalmic assessment if you experience:
- Sudden blurred vision in one eye
- New central distortion
- A dark or missing area of vision
- New floaters
- Sudden worsening of existing vision
- Pain and redness with reduced vision
Retinal vein occlusion is not usually managed through the same immediate stroke pathway as an acute retinal artery occlusion. Nevertheless, sudden visual change may have several serious causes, and only an eye examination can establish the diagnosis.
What Causes Retinal Vein Occlusion?
RVO is associated mainly with vascular changes that narrow or compress retinal veins, slow blood flow and encourage thrombosis.
The blockage causes pressure to rise behind the obstruction. Retinal vessels may then leak blood, fluid and proteins.
Reduced blood flow also lowers the retina’s oxygen supply. The oxygen-deprived retina releases vascular endothelial growth factor, or VEGF, which increases vascular leakage and may stimulate abnormal new blood-vessel growth.
Who Is at Greater Risk?
High Blood Pressure
Hypertension is one of the most important associations with retinal vein occlusion.
Long-term high blood pressure damages and stiffens retinal arteries, increasing the likelihood that an artery will compress a neighbouring vein at a crossing point.
Blood pressure should be checked when an RVO is diagnosed—even when the patient has never previously been told that it is elevated.
Increasing Age
RVO becomes more common with increasing age as vascular disease, hypertension and arterial stiffness become more prevalent.
CRVO is particularly associated with adults aged 50 years and above, although younger patients can also be affected.
Diabetes
Diabetes can damage small blood vessels and frequently coexists with other vascular risk factors.
Testing blood glucose or HbA1c at diagnosis may also identify previously undiagnosed diabetes.
High Cholesterol and Cardiovascular Disease
Abnormal lipid levels and atherosclerotic cardiovascular disease may contribute to the vascular changes associated with RVO.
A diagnosis should therefore prompt a review of overall cardiovascular risk rather than being treated solely as an isolated eye problem.
Glaucoma and Raised Eye Pressure
Glaucoma and raised intraocular pressure are associated particularly with CRVO.
The exact relationship is complex, but pressure and structural changes around the optic nerve may affect venous outflow from the eye.
Eye pressure and the optic nerves should therefore be assessed in both eyes.
Smoking and Obesity
Smoking, obesity and physical inactivity contribute to vascular disease and may occur alongside hypertension, diabetes and abnormal cholesterol.
Addressing these factors protects general health, even though it cannot reverse retinal damage already present.
Blood and Clotting Disorders
Less common associations include:
- Hyperviscosity disorders
- Certain blood cancers
- Severe anaemia
- Inflammatory conditions
- Selected inherited or acquired clotting disorders
These causes are considered particularly when RVO occurs in a young patient, affects both eyes, recurs or occurs without the usual cardiovascular risk factors.
Extensive thrombophilia testing is not routinely useful for every older patient with an isolated typical RVO. Investigation should be directed by the patient’s age, history, examination and medical context.
Does Retinal Vein Occlusion Mean I Am About to Have a Stroke?
RVO and cardiovascular disease share risk factors such as hypertension, diabetes, smoking and abnormal cholesterol.
An RVO does not necessarily mean that a stroke is imminent, but it may reveal previously undiagnosed or inadequately controlled systemic vascular disease.
A medical review should generally include:
- Blood-pressure measurement
- Blood-glucose or HbA1c assessment
- Lipid assessment
- Review of smoking and weight
- Review of cardiovascular history
- Additional tests when clinically indicated
The objective is to improve overall health and reduce future vascular risk—not simply to find a laboratory explanation for the eye blockage.
Is Retinal Vein Occlusion the Same as Retinal Artery Occlusion?
No.
A retinal vein occlusion blocks blood drainage out of the retina, causing congestion, bleeding and swelling.
A retinal artery occlusion blocks blood flow into the retina and usually causes sudden, severe visual loss from acute retinal ischaemia.
Retinal artery occlusion requires an emergency stroke evaluation. RVO has a different mechanism and management pathway, although both conditions warrant assessment of systemic vascular health.
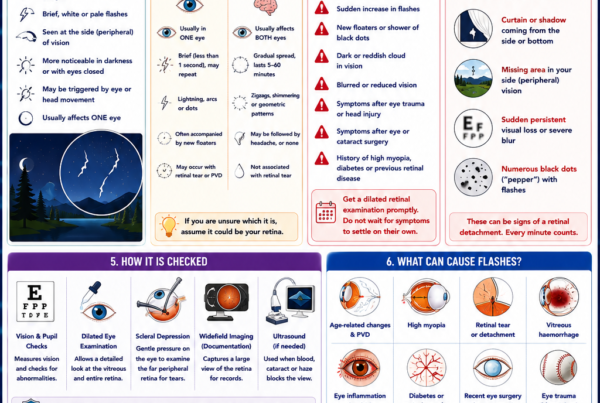
How Is Retinal Vein Occlusion Diagnosed?
Visual Acuity
Vision is measured in each eye.
The level of visual loss provides information about macular involvement, retinal ischaemia and prognosis.
Pupil Examination
A relative afferent pupillary defect may suggest severe retinal ischaemia, particularly in CRVO.
Eye-Pressure Measurement
Eye pressure is checked because glaucoma is a risk factor and abnormal new vessels may later cause neovascular glaucoma.
Dilated Retinal Examination
Dilating drops enlarge the pupils so that the retina can be examined.
Typical findings may include:
- Retinal haemorrhages
- Dilated and tortuous veins
- Cotton-wool spots
- Macular swelling
- Hard exudates
- Optic-disc swelling
- Abnormal new blood vessels
In BRVO, the changes are usually confined to one sector. In CRVO, they are more widespread throughout the retina.
Optical Coherence Tomography
Optical coherence tomography, or OCT, produces detailed cross-sectional images of the retina.
It is the key test for:
- Detecting macular oedema
- Measuring retinal thickness
- Identifying cysts or fluid
- Planning treatment
- Monitoring the response to injections
- Detecting recurrent swelling
Certain OCT features, including disruption of retinal layers from severe ischaemia, may be associated with a poorer visual outcome even when fluid resolves.
Fluorescein Angiography
During fluorescein angiography, dye is injected into a vein and retinal photographs are taken as the dye circulates through the eye.
The test can demonstrate:
- Areas of leakage
- Blocked retinal circulation
- Macular ischaemia
- Peripheral non-perfusion
- Abnormal new blood vessels
It is particularly useful when the degree of retinal ischaemia is uncertain or laser treatment is being planned.
OCT Angiography
OCT angiography displays retinal blood flow without an intravenous dye.
It can map areas of capillary loss and abnormal vessels, although it does not show leakage in the same way as fluorescein angiography.
The two tests provide complementary rather than identical information.
Widefield Retinal Imaging
Widefield photography or angiography may document a larger area of peripheral retina.
It helps assess the extent of haemorrhage, ischaemia and neovascularisation, although imaging does not replace a full clinical examination.
What Are the Main Complications?
Macular Oedema
Macular oedema is the most common cause of reduced vision following RVO.
VEGF and other inflammatory signals make damaged retinal vessels increasingly permeable, allowing fluid to collect within the macula.
Macular oedema may improve spontaneously in selected mild cases, but persistent swelling can damage retinal cells and limit visual recovery.
Macular Ischaemia
Macular ischaemia occurs when the fine capillary network supplying the macula becomes severely impaired.
Treatment can reduce swelling but cannot reopen every damaged capillary or restore retinal cells lost through inadequate oxygen supply.
A patient may therefore have a dry OCT after treatment but remain visually limited by macular ischaemia.
Retinal Neovascularisation
Poorly perfused retina may release high levels of VEGF, stimulating fragile new vessels.
These vessels may develop:
- On the retinal surface
- Around the optic nerve
- On the iris
- Within the eye’s drainage angle
They can bleed, form scar tissue or cause glaucoma.
Vitreous Haemorrhage
Abnormal new vessels may bleed into the vitreous, causing:
- Sudden floaters
- A dark cloud
- Hazy vision
- Severe visual reduction
The blood may clear, but the underlying neovascularisation still requires treatment.
Neovascular Glaucoma
New vessels may grow over the iris and drainage angle, blocking fluid from leaving the eye.
Eye pressure can then rise dramatically, causing:
- Severe pain
- Redness
- Headache
- Nausea
- Further visual loss
This is an urgent and potentially difficult complication, most commonly associated with severe ischaemic CRVO.
How Is Retinal Vein Occlusion Treated?
Treatment is directed at the complications of the occlusion rather than physically removing the venous blockage.
The main aims are to:
- Reduce macular swelling
- Improve or stabilise vision
- Detect retinal ischaemia
- Prevent bleeding
- Treat abnormal new vessels
- Control glaucoma
- Address systemic vascular risk factors
Observation
Observation may be appropriate when:
- Vision remains good
- The macula is not significantly swollen
- A mild BRVO has recently developed
- There is no neovascularisation
- The expected benefit of treatment is limited
Observation still requires scheduled examinations and OCT monitoring. It does not mean that the condition has been dismissed.
In BRVO with mild recent visual impairment, an initial period of observation may be reasonable, but early treatment is often favoured when vision is meaningfully affected by macular oedema.
Anti-VEGF Eye Injections
Anti-VEGF medication is the main treatment for visually significant macular oedema caused by BRVO or CRVO.
The medication is injected into the vitreous after the eye has been cleaned and numbed.
Anti-VEGF treatment can:
- Reduce retinal leakage
- Reduce macular swelling
- Improve vision in many patients
- Cause abnormal new vessels to regress
- Lower the risk of certain neovascular complications
Treatment is usually initiated promptly when macular oedema is affecting vision because delayed treatment may produce less visual improvement.
How Many Injections Are Needed?
There is no single number for every patient.
Many patients begin with a series of injections at relatively close intervals. Treatment is then adjusted according to:
- Visual acuity
- OCT findings
- Recurrence of fluid
- Retinal ischaemia
- The medicine used
- Treatment response
Some patients require only an initial course. Others need intermittent or continuing treatment for several years.
Long-term studies show that many patients continue to require monitoring and treatment beyond the first year.
Are Eye Injections Painful?
Anaesthetic drops are used, and the surface of the eye is cleaned with antiseptic.
Most patients experience pressure or brief discomfort rather than significant sharp pain.
Possible risks include:
- Infection inside the eye
- Inflammation
- Temporary pressure elevation
- Surface bleeding
- Retinal tear or detachment
- Cataract injury, which is uncommon
Increasing pain, worsening redness, marked light sensitivity or reduced vision after an injection requires urgent review.
Steroid Injections or Implants
Corticosteroid treatment can reduce retinal leakage and inflammation.
A dexamethasone implant may be considered when:
- Anti-VEGF response is incomplete
- Injection frequency is difficult to sustain
- Other clinical considerations favour steroid treatment
- The eye has already undergone cataract surgery
Important risks include:
- Raised eye pressure
- Glaucoma
- Cataract progression
- Infection associated with any intravitreal procedure
Steroids are therefore not automatically preferable even when they last longer between treatments.
Retinal Laser Treatment
Laser has several possible roles, but it is no longer the primary treatment for most centre-involving macular oedema.
Panretinal Photocoagulation
Panretinal photocoagulation, or PRP, is applied to the peripheral retina when abnormal new vessels develop.
It reduces the retina’s production of signals that stimulate neovascularisation and helps lower the risk of:
- Vitreous haemorrhage
- Further abnormal vessel growth
- Neovascular glaucoma
PRP may be combined with anti-VEGF treatment when iris or angle neovascularisation is present.
Macular Grid Laser
Macular grid laser may still be used in selected cases of BRVO, particularly when oedema is persistent and outside the central foveal area.
However, modern anti-VEGF treatment generally produces better visual outcomes for significant macular oedema and has largely replaced laser as first-line treatment.
Macular grid laser has not shown a meaningful role for macular oedema caused by CRVO.
Vitrectomy Surgery
Surgery is not required for an uncomplicated vein occlusion.
Vitrectomy may be considered for complications such as:
- Non-clearing vitreous haemorrhage
- Tractional retinal detachment
- Epiretinal membrane
- Significant vitreomacular traction
- Other complex retinal complications
The operation treats the complication rather than reopening the blocked retinal vein.
Should I Take Aspirin or Blood-Thinning Medication?
Aspirin, anticoagulants and antiplatelet medication are not routinely started solely to treat an isolated retinal vein occlusion.
There is no high-quality evidence that routinely thinning the blood reopens the retinal vein or improves the visual outcome.
However, these medications may be necessary for other medical reasons such as:
- Previous stroke
- Heart disease
- Atrial fibrillation
- Vascular stents
- A diagnosed clotting disorder
Do not start or stop aspirin, warfarin or another blood thinner without discussing it with the doctor managing your general health.
What Medical Assessment Is Needed?
A patient diagnosed with RVO should generally have their vascular health reviewed.
This commonly includes:
- Blood-pressure measurement
- Blood-glucose or HbA1c testing
- Lipid profile
- Review of smoking
- Review of cardiovascular history
- Review of current medications
- Further blood tests when clinically indicated
Young patients, bilateral or recurrent cases and patients without typical vascular risk factors may require more specialised investigation.
Controlling systemic risk factors protects the other eye and general health, although it cannot guarantee that the affected retina will recover.
Can the Blocked Vein Be Reopened?
There is currently no established routine procedure that safely removes the blockage and restores normal retinal venous circulation.
Treatment instead addresses:
- Leakage
- Macular oedema
- Abnormal vessel growth
- Eye pressure
- Systemic vascular risk factors
Some circulation may improve naturally as collateral drainage channels develop, particularly after BRVO.
What Determines Visual Recovery?
The final vision depends on:
- Vision at presentation
- Whether BRVO or CRVO is present
- Degree of macular oedema
- Degree of macular ischaemia
- Duration of swelling
- Damage to the photoreceptor layers
- Development of abnormal vessels
- Treatment response
- Other retinal, optic-nerve or lens disease
Patients with swelling but relatively preserved retinal circulation may improve substantially following treatment.
Eyes with severe macular ischaemia may remain visually impaired even when injections successfully remove the fluid.
Can Vision Return to Normal?
Sometimes.
A mild BRVO with limited macular damage may recover excellent vision. Other patients improve but retain:
- Mild blur
- Distortion
- Reduced contrast
- Poorer vision in dim light
- A small visual-field defect
Severe ischaemic CRVO has a less favourable visual prognosis because treatment cannot reverse extensive loss of retinal circulation.
Can RVO Occur Again?
Yes.
Another occlusion may develop:
- Elsewhere in the same eye
- In the other eye
- After a long period of stability
Good control of hypertension, diabetes, cholesterol and glaucoma is important, but recurrence cannot be prevented with certainty.
New visual symptoms in either eye require assessment.
How Often Will I Need Follow-Up?
Follow-up depends on:
- Type of occlusion
- Retinal ischaemia
- Macular oedema
- Treatment response
- Presence of abnormal vessels
- Eye pressure
- Time since diagnosis
Patients receiving injections may initially be reviewed every four to eight weeks.
Ischaemic CRVO may require monthly monitoring during the early period because new vessels can develop even when macular swelling is being treated. Monitoring may continue for several years in higher-risk cases.
When Should I Seek Urgent Review During Follow-Up?
Seek prompt care if you develop:
- Sudden further reduction in vision
- Numerous new floaters
- A dark cloud or haze
- New distortion
- A shadow or curtain
- Increasing eye pain
- Significant redness
- Headache or nausea with eye pain
- Worsening symptoms after an injection
Do not wait until the next scheduled OCT if vision changes suddenly.
Frequently Asked Questions
Is retinal vein occlusion an eye stroke?
It is sometimes informally called an “eye stroke”, but this term can be confusing.
RVO blocks venous drainage, whereas retinal artery occlusion stops arterial blood entering the retina and requires an emergency stroke pathway.
Both conditions involve the retinal circulation but have different urgency, investigation and treatment.
Is RVO caused by a blood clot?
Thrombus formation usually plays a role, but the condition often begins with compression, abnormal vessel walls or reduced blood flow rather than a clot travelling from elsewhere in the body.
Can stress cause retinal vein occlusion?
Stress is not usually regarded as a direct cause.
However, chronic stress may indirectly affect sleep, blood pressure, smoking, glucose control and cardiovascular health.
Can high blood pressure alone cause RVO?
Hypertension is a major risk factor, but most patients have a combination of age-related vascular changes and other individual factors.
Does every RVO require injections?
No.
Injections are primarily used when macular oedema is causing significant visual impairment or when abnormal new vessels require rapid control.
Will injections cure the occlusion?
No.
They treat leakage and swelling caused by the occlusion. Recurrence is possible while the underlying retinal circulation remains abnormal.
Why is my vision poor when the OCT shows no fluid?
The macula may have suffered ischaemia, photoreceptor damage or retinal thinning. Removing fluid does not necessarily restore cells already damaged by inadequate blood flow.
Can I exercise after an RVO?
Ordinary physical activity is usually beneficial for cardiovascular health unless another medical condition restricts exercise.
There is generally no need for prolonged bed rest. Follow individual advice after an injection or if there is vitreous haemorrhage.
Can I fly?
RVO itself does not usually prohibit air travel.
Restrictions may apply if the patient subsequently undergoes retinal surgery involving an intraocular gas bubble.
Can cataract surgery be performed after an RVO?
Yes, once the retinal condition has been assessed and is sufficiently stable.
Pre-existing macular ischaemia or oedema may limit the visual improvement expected from cataract surgery, and treatment may be needed before or around the time of the operation.
The Bottom Line
Retinal vein occlusion occurs when blood cannot drain normally from the retina.
The two main types are:
- Branch retinal vein occlusion, affecting part of the retina
- Central retinal vein occlusion, affecting the main retinal vein and generally carrying a greater risk of severe complications
Visual loss is commonly caused by macular oedema, retinal ischaemia or bleeding.
Anti-VEGF injections are the main treatment for visually significant macular swelling. Steroid treatment may be appropriate in selected patients, while retinal laser is used mainly when abnormal new blood vessels develop.
Treatment controls the consequences of the occlusion but does not physically remove the blockage.
A diagnosis should also prompt assessment of blood pressure, diabetes, cholesterol, glaucoma and overall cardiovascular health.
Sudden painless blur in one eye should never be ignored. Early examination and treatment provide the best opportunity to protect vision.
References
- American Academy of Ophthalmology. Retinal Vein Occlusions Preferred Practice Pattern. Ophthalmology. 2025.
- National Eye Institute. Central Retinal Vein Occlusion. Updated November 2024.
- Royal College of Ophthalmologists. Retinal Vein Occlusion Guidelines. 2022.
- American Society of Retina Specialists. Branch Retinal Vein Occlusion.
- American Society of Retina Specialists. Central Retinal Vein Occlusion.