Author: Dr Val Phua
Estimated reading time: 10–12 minutes
Your Eyes May Feel Dry Even When You Produce Plenty of Tears
Many patients with dry, burning or watery eyes assume that they are simply not producing enough tears.
However, one of the most common causes of dry eye is a problem with the tiny oil-producing glands within the eyelids. This condition is known as meibomian gland dysfunction, or MGD.
When the meibomian glands become blocked or produce poor-quality oil, the tears evaporate too quickly. The eyes may then feel dry, gritty, tired or uncomfortable—even when they are producing plenty of watery tears.
MGD is usually a chronic condition, but appropriate treatment can improve tear-film stability, relieve symptoms and help preserve the function of the remaining glands.
What Are the Meibomian Glands?
The meibomian glands are narrow oil-producing glands located inside the upper and lower eyelids.
Each time you blink, these glands release a substance called meibum onto the surface of the eye.
Meibum forms the oily outer layer of the tear film. Its main functions are to:
- Slow tear evaporation
- Keep the tear film stable between blinks
- Lubricate the eyelids
- Maintain a smooth optical surface
- Reduce friction when blinking
Healthy meibum is generally clear and flows easily.
When the glands become dysfunctional, the oil may become thick, cloudy or difficult to express. Some glands may eventually shorten, distort or become less functional.
What Is Meibomian Gland Dysfunction?
Meibomian gland dysfunction is a chronic abnormality of the eyelid oil glands.
It most commonly involves:
- Blockage of the gland openings
- Thickening of the gland secretions
- Reduced delivery of oil to the tear film
- Changes in the quality of the oil
- Inflammation around the eyelid margins
- Structural loss of gland tissue in more advanced disease
Without an adequate oily layer, the watery tears evaporate rapidly. This produces evaporative dry eye disease.
MGD may occur by itself or together with aqueous-deficient dry eye, blepharitis, allergy or other ocular-surface conditions.
How Does MGD Cause Dry Eye?
A normal blink spreads tears and oil across the eye.
When the meibomian glands are blocked:
- Less oil reaches the tear film.
- The watery tears evaporate more rapidly.
- The tear film breaks up between blinks.
- The corneal surface becomes exposed and irritated.
- Inflammation develops.
- Inflammation further disrupts gland and tear-film function.
This creates a self-perpetuating cycle:
Blocked glands → poor oil layer → rapid evaporation → irritation and inflammation → further gland dysfunction
Breaking this cycle often requires consistent treatment rather than occasional eye drops alone.
What Does MGD Feel Like?
Symptoms vary considerably and may fluctuate from day to day.
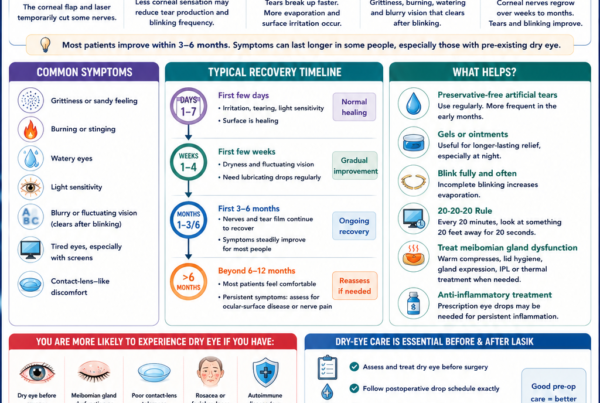
Common symptoms include:
- Burning or stinging
- Grittiness or a sandy sensation
- Tired or heavy eyes
- Redness
- Intermittent blurred vision
- Vision that improves after blinking
- Excessive watering
- Sensitivity to light
- Contact-lens discomfort
- Eyelids that feel tender or sticky
- Symptoms that worsen later in the day
- Difficulty keeping the eyes open during prolonged screen use
Some patients have visible gland abnormalities without significant symptoms. Others experience considerable discomfort despite relatively mild clinical findings.
Why Does MGD Cause Fluctuating Vision?
The tear film forms the first optical surface that light passes through when entering the eye.
When the oily layer is inadequate, the tear film breaks up rapidly and the corneal surface becomes optically irregular.
Patients may notice:
- Words becoming blurry while reading
- Vision clearing briefly after blinking
- Difficulty maintaining focus at a computer
- Glare or halos at night
- Variability during spectacle or cataract measurements
A stable tear film is therefore important not only for comfort but also for clear and consistent vision.
What Causes Meibomian Gland Dysfunction?
MGD usually results from several overlapping factors.
Ageing
Meibomian gland structure and function may decline with age.
Older adults are also more likely to have eyelid inflammation, hormonal changes, previous eye surgery or medication use that contributes to ocular-surface disease.
Reduced and Incomplete Blinking
Blinking helps pump oil from the meibomian glands.
During concentrated visual tasks, people blink less often and may not close their eyelids completely.
This is common during:
- Computer work
- Smartphone use
- Gaming
- Reading
- Online meetings
- Watching television
Incomplete blinking may allow the oil to remain trapped within the glands.
Prolonged Screen Use
Screen use contributes to MGD mainly through reduced and incomplete blinking rather than blue light exposure.
Symptoms may be particularly troublesome when prolonged screen use is combined with air conditioning or contact-lens wear.
Blepharitis
Blepharitis is inflammation of the eyelid margins.
It may lead to:
- Red or thickened eyelid edges
- Crusting around the lashes
- Blocked gland openings
- Recurrent styes
- Burning or itching
- Poor-quality meibum
MGD and blepharitis frequently occur together.
Rosacea
Rosacea can affect both the facial skin and the eyelids.
Ocular rosacea may cause:
- Eyelid redness
- Dilated blood vessels around the lid margins
- Recurrent styes or chalazia
- Thickened meibum
- Chronic inflammation
- Corneal involvement in more severe cases
Some patients have significant ocular rosacea even when facial symptoms are subtle.
Demodex
Demodex are microscopic mites that live around the eyelashes and eyelid glands.
Excessive infestation may contribute to eyelid inflammation, itching, lash debris and gland dysfunction.
Contact-Lens Wear
Contact lenses may increase tear evaporation and interact with the eyelids and tear film.
Discomfort is more likely when lenses are worn for long hours or combined with:
- Heavy screen use
- Air conditioning
- Poor lens hygiene
- Existing gland dysfunction
- Infrequent lens replacement
Hormonal Influences
The meibomian glands are influenced by hormones, particularly androgens.
Hormonal changes associated with ageing, menopause and certain medications may affect oil production and gland function.
Medications
Medications that may contribute to gland dysfunction or dry eye include:
- Isotretinoin
- Some antihistamines
- Certain antidepressants
- Hormonal medications
- Selected glaucoma eye drops
- Other medications that reduce tear production
Do not stop prescribed medication without discussing it with your doctor.
Eye Surgery
Dry-eye symptoms and MGD may become more apparent after:
- LASIK
- SMILE
- PRK
- Cataract surgery
- Eyelid surgery
Pre-existing gland dysfunction should ideally be identified and managed before elective eye surgery because an unstable tear film can affect comfort, recovery and the accuracy of preoperative measurements.
Environmental Exposure
MGD symptoms may worsen with:
- Air conditioning
- Low humidity
- Wind
- Fans directed at the face
- Smoke
- Haze
- Air pollution
These factors increase tear evaporation even when the glands are only mildly dysfunctional.
Can the Meibomian Glands Become Permanently Damaged?
Yes.
Longstanding obstruction and inflammation may lead to:
- Gland shortening
- Distortion
- Dilation
- Loss or “dropout” of gland tissue
Once significant gland tissue has been lost, it may not fully regenerate.
Treatment therefore aims to:
- Improve the function of remaining glands
- Restore healthier oil flow
- Reduce inflammation
- Stabilise the tear film
- Prevent or slow further deterioration
This is one reason why persistent symptoms should not simply be ignored.
How Is MGD Diagnosed?
MGD is diagnosed using a combination of symptoms and clinical findings.
No single test is sufficient for every patient.
Symptom History
Your ophthalmologist may ask:
- When symptoms occur
- Whether vision fluctuates
- Whether symptoms worsen during screen use
- Whether contact lenses are worn
- Whether there is facial rosacea
- Which medications and eye drops are being used
- Whether previous eye surgery has been performed
Eyelid-Margin Examination
The gland openings are examined for:
- Blockage
- Thickening
- Capping
- Redness
- Irregularity
- Dilated blood vessels
- Crusting or Demodex-related debris
Gland Expression
Gentle pressure may be applied to the eyelids to assess:
- How easily oil is released
- How many glands are functioning
- Whether the oil is clear, cloudy, thick or toothpaste-like
- Whether expression is uncomfortable
This provides functional information that imaging alone cannot provide.
Tear-Film Assessment
The tear film may be assessed for:
- Rapid breakup
- Reduced oily layer
- Debris or foam
- Increased evaporation
- Areas of ocular-surface staining
Meibography
Meibography uses infrared imaging to show the structure of the glands within the eyelids.
It may reveal:
- Gland shortening
- Distortion
- Dilation
- Areas of gland loss
- Differences between the upper and lower eyelids
Meibography is useful for documenting gland structure and discussing long-term risk. However, it should be interpreted together with symptoms, gland expression and tear-film findings.
Abnormal-looking glands do not always explain every symptom, and a normal image does not completely exclude functional disease.
Additional Tests
Selected patients may undergo:
- Non-invasive tear-breakup testing
- Lipid-layer assessment
- Tear osmolarity testing
- Ocular-surface staining
- Blink analysis
- Corneal topography
- Tear-volume measurement
Not every patient requires all of these tests.
How Is Meibomian Gland Dysfunction Treated?
Treatment depends on:
- The degree of gland obstruction
- The quality of the oil
- The amount of gland loss
- Eyelid inflammation
- Associated dry eye
- Rosacea or Demodex
- Symptom severity
- Previous response to treatment
MGD treatment is usually stepwise and often requires long-term maintenance.
Warm Compresses
Warm compresses help soften thickened meibum so that it can flow more easily.
For a home compress to work effectively:
- Use a clean compress designed to retain heat.
- Apply it over the closed eyelids.
- Keep it comfortably warm for approximately 5–10 minutes.
- Reheat it if it cools too quickly.
- Repeat consistently, usually once or twice daily when advised.
A cloth that becomes cold after a minute may not deliver sufficient sustained warmth.
The compress should never be hot enough to burn the eyelid skin.
Eyelid Massage
Gentle eyelid massage after warming may help move softened oil towards the gland openings.
Massage should be light and directed towards the eyelid margin:
- Downwards for the upper eyelid
- Upwards for the lower eyelid
Forceful squeezing may irritate the eye and is generally unnecessary.
Patients should follow the technique recommended by their eye-care professional.
Eyelid Hygiene
Cleaning the eyelid margins may help reduce debris, bacterial load and inflammation.
Options include:
- Commercial eyelid wipes
- Eyelid-cleansing solutions
- Treatment directed at Demodex when present
- Other clinician-recommended preparations
Eyelid hygiene should be gentle and should not involve harsh household soaps or chemicals.
Artificial Tears
Artificial tears do not unblock the meibomian glands, but they may reduce friction and improve comfort while the underlying gland problem is treated.
Lipid-containing artificial tears may be helpful for evaporative dry eye.
Preservative-free formulations are generally preferred when drops are required frequently.
Improve Blinking
During prolonged screen use:
- Blink fully and deliberately.
- Follow the 20-20-20 rule.
- Take regular breaks.
- Position the screen slightly below eye level.
- Increase the font size rather than moving closer.
- Avoid direct airflow towards the face.
Blinking exercises may be helpful for patients who habitually blink incompletely.
Treat Associated Blepharitis, Rosacea or Demodex
MGD may not improve adequately unless related eyelid disease is also controlled.
Treatment may include:
- Targeted eyelid cleansing
- Topical medications
- Oral antibiotics in selected patients
- Rosacea management
- Demodex-specific treatment
Treatment should be individualised rather than using antibiotics routinely for every patient.
Prescription Anti-Inflammatory Treatment
Ocular-surface inflammation may persist even after gland obstruction improves.
Selected patients may benefit from:
- Short courses of topical corticosteroids under supervision
- Ciclosporin
- Other anti-inflammatory or immunomodulating eye drops
- Treatment directed at associated ocular-surface disease
These medicines should be prescribed and monitored by an eye-care professional.
Oral Medication
Low-dose oral tetracycline-class medication may be considered in selected patients with significant inflammatory MGD or ocular rosacea.
These medications may alter gland secretions and reduce inflammation.
They are not appropriate for everyone and may cause side effects. Pregnancy, allergies, age and interactions with other medication must be considered.
In-Clinic Gland Expression
An eye-care professional may manually express blocked glands after appropriate heating.
This can help release stagnant material, although it may be uncomfortable and does not replace ongoing home care.
The benefit varies according to disease severity and the amount of functioning gland tissue.
Thermal Pulsation
Thermal-pulsation systems apply controlled heat to the inner eyelid surface while using pressure or massage to clear gland obstruction.
Some patients experience improvement in gland function and symptoms following treatment.
However:
- Results vary.
- Treatment does not regenerate glands that have already been lost.
- Benefits may not be permanent.
- Maintenance therapy may still be required.
- No single device is clearly superior for every patient.
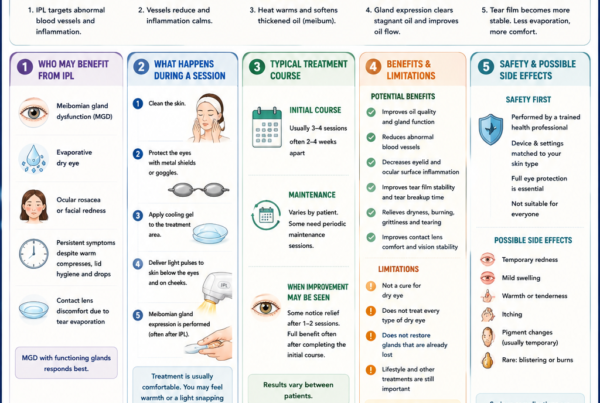
Intense Pulsed Light
Intense pulsed light, or IPL, delivers controlled pulses of light to the skin around the eyelids.
Proposed effects include:
- Reducing abnormal superficial blood vessels
- Decreasing inflammatory signalling
- Heating and softening meibum
- Improving gland expression
- Helping selected patients with rosacea-associated disease
Evidence suggests that IPL can improve symptoms and tear-film findings in selected patients with MGD, particularly when combined with gland expression.
It is not suitable for every skin type or clinical situation, and treatment should be performed using appropriate eye protection by a trained practitioner.
Other Procedures
Depending on the clinical findings, other options may include:
- Alternative heat-and-expression systems
- Low-level light therapy
- Meibomian gland probing in selected cases
- Treatment of incomplete eyelid closure
- Scleral or specialised contact lenses for severe ocular-surface disease
The evidence and indications vary between procedures.
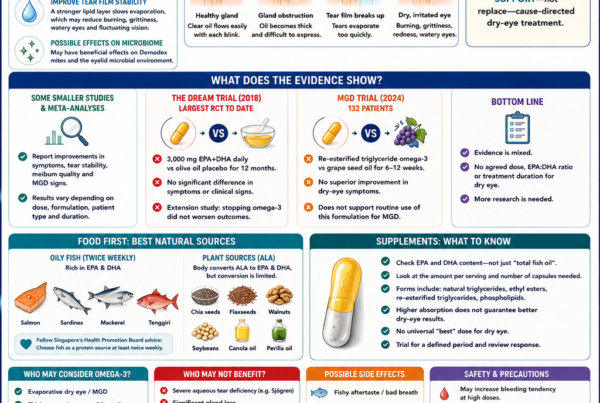
Do Omega-3 Supplements Help MGD?
Omega-3 supplements are frequently promoted for meibomian gland dysfunction.
Research results are mixed, and supplements should not be presented as a guaranteed treatment.
A balanced diet containing oily fish, nuts, seeds and other healthy fats supports general health. Patients taking anticoagulants or those with medical conditions should discuss supplements with their doctor.
How Long Does Treatment Take?
MGD is usually a chronic condition rather than a one-time blockage.
Some patients improve within weeks, while others require several months of consistent treatment.
The response depends on:
- Duration of disease
- Degree of obstruction
- Amount of gland loss
- Associated inflammation
- Adherence to treatment
- Environmental and lifestyle factors
Once symptoms improve, maintenance treatment is often needed to reduce recurrence.
Can MGD Be Cured?
MGD can usually be controlled, but it may not be permanently cured.
The gland openings may become blocked again if treatment stops, particularly when underlying risk factors remain.
The realistic goals are to:
- Improve oil flow
- Stabilise the tear film
- Reduce discomfort
- Preserve remaining gland function
- Minimise flare-ups
- Improve visual quality and contact-lens tolerance
How Can I Reduce the Risk of MGD Getting Worse?
Helpful habits include:
- Taking regular screen breaks
- Blinking fully
- Managing blepharitis or rosacea
- Limiting contact-lens wear when the eyes are irritated
- Avoiding smoke and direct airflow
- Removing eye makeup thoroughly
- Replacing old cosmetic products
- Following a consistent warm-compress routine when advised
- Attending follow-up if symptoms persist
When Should I See an Eye Specialist?
Arrange an examination if:
- Symptoms persist despite artificial tears
- Vision frequently fluctuates
- Warm compresses have not helped
- Contact lenses are increasingly uncomfortable
- You experience recurrent styes or chalazia
- Eyelids remain red or tender
- Symptoms affect work, reading or driving
- You are considering cataract or refractive surgery
Warning Signs Requiring Prompt Assessment
MGD usually causes chronic irritation rather than severe pain or major visual loss.
Seek prompt care if you develop:
- Severe eye pain
- Sudden reduction in vision
- Marked light sensitivity
- Significant one-sided redness
- A white spot on the cornea
- Thick discharge
- Eye injury or chemical exposure
- A painful red eye while wearing contact lenses
These features may indicate an infection or another urgent condition rather than uncomplicated MGD.
Frequently Asked Questions
Is MGD the same as dry eye?
MGD is a major cause of evaporative dry eye, but dry eye can also result from inadequate watery tear production, inflammation, eyelid problems or nerve dysfunction.
Can artificial tears treat MGD?
Artificial tears relieve symptoms but do not usually clear blocked glands. They work best as part of a broader treatment plan.
Can blocked glands be reopened?
Some obstructed glands can release oil again after heating, expression and appropriate treatment. Glands that have undergone substantial structural loss may not fully recover.
Is MGD caused by bacteria?
Bacteria may contribute to eyelid inflammation and changes in gland secretions, but MGD is not simply a bacterial infection.
Is IPL better than thermal pulsation?
Both may help selected patients, but the best choice depends on gland structure, skin type, inflammation, rosacea, symptoms and previous treatment. Current evidence does not establish one procedure as universally best.
Can children or young adults develop MGD?
Yes. Screen use, incomplete blinking, contact lenses, acne treatments, rosacea and eyelid inflammation can contribute to MGD in younger patients.
Will warm compresses restore glands that have disappeared?
No. Warm compresses may improve oil flow from functioning glands but cannot reliably regenerate glands that have been lost.
The Bottom Line
Meibomian gland dysfunction occurs when the oil-producing glands within the eyelids become blocked, inflamed or structurally damaged.
Without sufficient healthy oil, tears evaporate quickly and the eyes become dry, irritated, watery or visually unstable.
Treatment may involve:
- Warm compresses
- Eyelid hygiene
- Improved blinking
- Artificial tears
- Treatment of blepharitis, rosacea or Demodex
- Prescription anti-inflammatory therapy
- Gland expression
- Thermal pulsation
- IPL in selected patients
No single treatment is best for everyone.
A comprehensive dry-eye assessment helps determine whether the problem is primarily gland obstruction, inflammation, gland loss, reduced tear production or a combination of factors. Identifying the mechanism allows treatment to be more precisely targeted and gives the best chance of restoring comfort and stable vision.
References
- Jones L, et al. TFOS DEWS III: Management and Therapy. American Journal of Ophthalmology. 2025.
- Wolffsohn JS, et al. TFOS DEWS III: Diagnostic Methodology. American Journal of Ophthalmology. 2025.
- Perez VL, et al. TFOS DEWS III Executive Summary. American Journal of Ophthalmology. 2025.
- Nelson JD, et al. The International Workshop on Meibomian Gland Dysfunction: Report of the Definition and Classification Subcommittee. Investigative Ophthalmology & Visual Science. 2011.
- Sabeti S, et al. Management of Meibomian Gland Dysfunction: A Review. Survey of Ophthalmology. 2020.
- Pucker AD, et al. LipiFlow for the Treatment of Dry Eye Disease. Cochrane Database of Systematic Reviews. 2024.
- Peira N, et al. Effectiveness and Safety of Intense Pulsed Light Therapy for Dry Eye Symptoms Due to Meibomian Gland Dysfunction: A Systematic Review. 2025.
- American Academy of Ophthalmology. Dry Eye Syndrome Preferred Practice Pattern.