Author: Dr Val Phua
Estimated reading time: 10–12 minutes
Red, Itchy or Crusty Eyelids May Be a Sign of Blepharitis
Blepharitis is inflammation of the eyelid margins—the edges of the eyelids where the eyelashes and oil-gland openings are located.
It commonly causes:
- Red or swollen eyelids
- Burning or itching
- Crusting around the eyelashes
- Grittiness
- Watery eyes
- Dry-eye symptoms
- Intermittently blurred vision
Blepharitis is usually not contagious and rarely causes permanent visual damage. However, it is often chronic and may recur if the underlying cause is not addressed.
Although it may appear to be a simple eyelid infection, blepharitis can involve bacteria, skin disease, blocked oil glands, Demodex mites, inflammation and tear-film instability. Many patients have more than one contributing factor.
What Is Blepharitis?
Blepharitis is a broad term describing inflammation affecting the eyelid margins.
The eyelid margin contains:
- Eyelashes and their follicles
- Oil-producing meibomian glands
- Sweat and sebaceous glands
- Skin microorganisms
- The openings through which oil enters the tear film
Inflammation in this area may disrupt the eyelashes, block the meibomian glands and destabilise the tear film. This explains why blepharitis commonly occurs together with dry-eye disease and meibomian gland dysfunction.
What Does Blepharitis Feel Like?
Symptoms may affect one eye or both, although chronic blepharitis commonly involves both eyelids.
Possible symptoms include:
- Burning or stinging
- Itching
- Grittiness or a foreign-body sensation
- Red or swollen eyelid margins
- Crusts or flakes around the eyelashes
- Eyelashes sticking together on waking
- Watery eyes
- Dryness
- Light sensitivity
- Tired or heavy eyelids
- Contact-lens discomfort
- Blurred or fluctuating vision
- Recurrent styes or chalazia
Symptoms often fluctuate and may worsen during periods of stress, illness, heavy screen use, air-conditioning or inconsistent eyelid care.
Why Can Blepharitis Blur Your Vision?
Blepharitis affects the eyelid oil glands and may destabilise the tear film covering the cornea.
When the tear film breaks up too quickly, the eye’s optical surface becomes irregular. Vision may then become temporarily blurred and improve after blinking.
Patients may notice:
- Words becoming less clear while reading
- Vision fluctuating during computer work
- Glare or halos at night
- Contact lenses becoming uncomfortable
- Variable spectacle or cataract measurements
Persistent blur that does not improve after blinking should be assessed for other causes.
The Main Types of Blepharitis
Blepharitis is traditionally divided into anterior and posterior forms. Many patients have features of both.
Anterior Blepharitis
Anterior blepharitis affects the outer eyelid margin around the eyelashes and their follicles.
It may be associated with:
- Excess bacteria around the lashes
- Seborrhoeic dermatitis or dandruff
- Demodex mites
- Allergic or irritative eyelid disease
Typical signs include crusting, flakes around the lashes, redness and irritation.
Staphylococcal Blepharitis
Staphylococcal blepharitis is associated with an inflammatory response to bacteria normally found on the skin.
Possible features include:
- Hard crusts around the eyelashes
- Red or thickened eyelid margins
- Loss or misdirection of eyelashes
- Recurrent styes
- Small ulcers around the lash follicles
This does not necessarily mean that the eyelid has a dangerous infection. Blepharitis often involves an abnormal inflammatory response to the usual eyelid environment rather than a simple infection that can be permanently eliminated with antibiotics.
Seborrhoeic Blepharitis
Seborrhoeic blepharitis is associated with oily skin, scalp dandruff and seborrhoeic dermatitis.
The eyelid scales tend to be softer or greasier than those seen in classic staphylococcal disease.
Treating associated scalp and facial skin disease may improve the eyelids.
Posterior Blepharitis
Posterior blepharitis affects the inner eyelid margin, where the meibomian glands open.
It is closely related to meibomian gland dysfunction.
When the glands become obstructed or inflamed:
- Oil becomes thick or difficult to express.
- Less oil reaches the tear film.
- Tears evaporate too rapidly.
- Dry-eye symptoms develop.
- Styes or chalazia may recur.
Posterior blepharitis is frequently associated with rosacea and may coexist with anterior disease.
Demodex Blepharitis
Demodex are microscopic mites that can live within eyelash follicles and meibomian glands.
Small numbers may be present without causing symptoms. Problems arise when the mite population increases and triggers inflammation.
Demodex blepharitis may cause:
- Itching, particularly around the eyelashes
- Red eyelid margins
- Burning or irritation
- Recurrent inflammation
- Lash loss or misdirection
- Cylindrical collars or “collarettes” around the base of the eyelashes
Prominent collarettes are highly suggestive of Demodex infestation and should prompt targeted assessment.
Treatment differs from ordinary bacterial or seborrhoeic blepharitis. In the United States, lotilaner ophthalmic solution 0.25% is approved specifically for Demodex blepharitis and is used twice daily for six weeks. Availability and regulatory approval vary between countries, so treatment options should be discussed locally with an ophthalmologist.
What Causes Blepharitis?
Blepharitis usually results from several interacting factors rather than one single cause.
Common contributors include:
- Excess bacterial colonisation around the eyelashes
- Meibomian gland dysfunction
- Seborrhoeic dermatitis
- Rosacea
- Demodex mites
- Allergies
- Contact-lens wear
- Eye makeup and cosmetic residue
- Reduced or incomplete blinking
- Preserved eye drops
- Dry-eye disease
- Environmental irritation from smoke, haze or air-conditioning
The most effective treatment depends on which of these factors is present.
Who Is More Likely to Develop Blepharitis?
Blepharitis can occur at any age.
Risk may be increased by:
- Oily skin
- Scalp dandruff
- Facial rosacea
- Meibomian gland dysfunction
- Demodex infestation
- Contact-lens wear
- Heavy screen use
- Poor eyelid or cosmetic hygiene
- Long-term use of certain eye drops
- Previous eyelid inflammation
- Increasing age
Children may also develop blepharitis. Persistent childhood eyelid inflammation associated with recurrent chalazia, light sensitivity or corneal involvement requires careful assessment.
Can Makeup Cause Blepharitis?
Eye makeup does not necessarily cause blepharitis, but it may contribute when products:
- Accumulate around the lash roots
- Block meibomian gland openings
- Are not removed thoroughly
- Are shared with other people
- Are used beyond their recommended lifespan
- Cause an allergic or irritative reaction
Applying eyeliner along the inner eyelid margin may directly cover the meibomian gland openings.
During an active flare, temporarily avoiding eye makeup may help. Old or contaminated products should be replaced rather than reused after significant inflammation or infection.
Can Contact Lenses Make Blepharitis Worse?
Yes.
Blepharitis and tear-film instability may reduce contact-lens comfort and increase deposits on the lens surface.
Contact-lens wearers should consider removing their lenses if the eyes become:
- Red
- Painful
- Light-sensitive
- Unusually watery
- Persistently uncomfortable
- Blurred despite cleaning or replacing the lenses
A painful red eye in a contact-lens wearer requires prompt assessment because corneal infection must be excluded.
How Is Blepharitis Diagnosed?
Diagnosis usually begins with a detailed examination of the eyelids, eyelashes, tear film and ocular surface.
The assessment may include:
Symptom and Medical History
Your ophthalmologist may ask about:
- Itching, burning and crusting
- Dry-eye symptoms
- Recurrent styes or chalazia
- Contact-lens wear
- Skin conditions such as rosacea or dandruff
- Makeup and skincare products
- Current medications and eye drops
- Previous eye surgery
- Treatments already attempted
Eyelid-Margin Examination
A slit-lamp microscope may be used to look for:
- Redness and swelling
- Crusts or scales
- Collarettes
- Blocked oil-gland openings
- Abnormal eyelashes
- Loss of eyelashes
- Ulcers around the follicles
- Dilated eyelid blood vessels
Meibomian Gland Assessment
Gentle pressure may be applied to determine:
- Whether oil can be expressed
- How many glands are functioning
- Whether the oil is clear, cloudy or thick
- Whether gland expression is painful
Tear-Film and Corneal Examination
The tear film and ocular surface are assessed for instability, inflammation and damage.
Special dyes may reveal areas of corneal or conjunctival staining that are not otherwise visible.
Demodex Assessment
The clinician may inspect the lash bases for collarettes and other characteristic features.
In selected cases, lashes may be examined microscopically, although a clinical diagnosis is often possible from the eyelid findings.
How Is Blepharitis Treated?
Treatment is tailored to the form and severity of blepharitis.
A typical plan may combine:
- Warm compresses
- Eyelid-margin cleansing
- Artificial tears
- Treatment of meibomian gland dysfunction
- Antibiotic medication where indicated
- Short-term anti-inflammatory treatment
- Management of Demodex, rosacea or seborrhoeic dermatitis
The American Academy of Ophthalmology recommends beginning with eyelid hygiene and adding targeted medication according to the underlying condition and clinical response.
Warm Compresses
Warm compresses help soften crusts and thickened meibomian-gland secretions.
A practical routine is:
- Wash your hands.
- Place a clean, comfortably warm compress over the closed eyelids.
- Maintain the warmth for several minutes.
- Gently clean or massage the eyelids as advised.
- Repeat consistently during active treatment.
The compress should not be hot enough to burn the skin.
Warm compresses are particularly helpful when blepharitis is associated with blocked oil glands.
Eyelid Hygiene
Eyelid cleaning removes crusts, makeup, debris and inflammatory material around the lashes.
Depending on the condition, options may include:
- Purpose-made eyelid wipes
- Eyelid-cleansing foam or solution
- A clinician-recommended diluted cleanser
- Targeted Demodex treatment
Cleaning should be gentle. Vigorous scrubbing may irritate the eyelid skin and ocular surface.
Use a separate clean pad for each eye, especially when inflammation is pronounced.
Artificial Tears
Artificial tears help relieve dryness and friction but do not directly eliminate eyelid inflammation.
Preservative-free lubricants are generally preferred when drops are required frequently.
Lipid-containing formulations may be useful when meibomian gland dysfunction is present.
Antibiotic Treatment
Topical antibiotic ointment or drops may be prescribed when bacterial anterior blepharitis is significant or when there is associated infection.
Selected patients with posterior blepharitis or ocular rosacea may benefit from oral tetracycline-class or macrolide medication because of their anti-inflammatory as well as antimicrobial effects.
Antibiotics are not required for every patient and should not replace eyelid hygiene. Long-term or repeated use should be medically supervised.
Anti-Inflammatory Eye Drops
A short course of topical corticosteroid may be prescribed when there is significant inflammation involving the eyelid margin, conjunctiva or cornea.
Steroid eye drops can raise eye pressure, contribute to cataract formation and worsen certain infections when used incorrectly. They should therefore be used only under professional supervision.
Other anti-inflammatory dry-eye treatments may be considered when persistent ocular-surface inflammation is present.
Treatment for Demodex
Demodex-associated disease requires treatment directed at the mites as well as associated inflammation.
Options vary according to local availability and may include:
- Purpose-designed eyelid preparations
- In-clinic eyelid cleaning
- Prescription antiparasitic therapy
- Treatment of associated meibomian gland dysfunction
Lotilaner ophthalmic solution has demonstrated reduction in collarettes, mite density and eyelid redness in controlled clinical trials and is FDA-approved for Demodex blepharitis in the United States.
Concentrated tea-tree oil should not be applied directly around the eyes without professional guidance because it may cause significant irritation or toxicity to the ocular surface.
Treating Associated Skin Disease
Blepharitis may remain difficult to control if associated dandruff or rosacea is untreated.
Management may involve:
- Appropriate scalp treatment
- Facial skincare
- Rosacea treatment
- Dermatological review
- Avoiding known skin triggers
The eyelids and facial skin should be considered together rather than treated as completely separate conditions.
In-Clinic Treatments
When posterior blepharitis and meibomian gland dysfunction remain troublesome, selected patients may benefit from:
- Professional gland expression
- Thermal-pulsation treatment
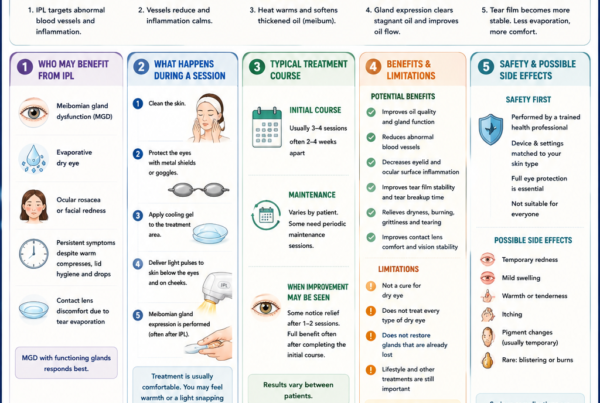
- Intense pulsed light
- Targeted eyelid cleaning
- Treatment for Demodex
- Other dry-eye therapies
These treatments are not necessary for everyone and do not replace regular home care. Evidence supports a personalised approach rather than one procedure for all patients.
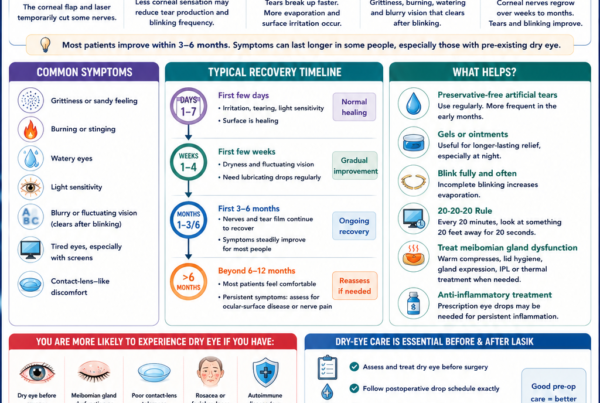
How Long Does Blepharitis Take to Improve?
Some patients notice improvement within days or weeks, but chronic blepharitis often requires longer-term maintenance.
The response depends on:
- The underlying cause
- Severity of inflammation
- Presence of MGD or dry eye
- Associated rosacea or Demodex
- Consistency of eyelid care
- Contact-lens and cosmetic habits
Symptoms often recur when eyelid hygiene is stopped completely. Blepharitis is therefore better regarded as a condition to be controlled rather than permanently cured.
Can Blepharitis Cause Complications?
Possible complications include:
- Recurrent styes
- Chalazia
- Dry-eye disease
- Loss or misdirection of eyelashes
- Chronic red eye
- Contact-lens intolerance
- Corneal inflammation
- Corneal ulceration or scarring in severe cases
Corneal complications are uncommon but potentially sight-threatening. Persistent pain, light sensitivity or reduced vision should not be attributed automatically to ordinary blepharitis.
What Can I Do Every Day?
Helpful habits include:
- Clean the eyelid margins consistently.
- Use warm compresses when advised.
- Remove eye makeup thoroughly.
- Replace old eye cosmetics.
- Avoid sharing makeup.
- Blink fully during screen use.
- Take regular screen breaks.
- Treat scalp dandruff and rosacea.
- Avoid smoke and direct airflow.
- Reduce contact-lens wear during flare-ups.
- Use prescribed medication exactly as directed.
Treatment should be continued long enough to control the inflammation rather than used only on particularly uncomfortable days.
When Should I See an Eye Specialist?
Arrange an examination if:
- Symptoms persist despite regular eyelid cleaning
- Vision frequently fluctuates
- You develop recurrent styes or chalazia
- Eyelashes are falling out or growing inwards
- Contact lenses have become uncomfortable
- One eye is significantly worse than the other
- The eyelids remain swollen or tender
- You have facial rosacea
- You are considering cataract or refractive surgery
Treating blepharitis before eye surgery can improve comfort and help stabilise the ocular surface.
Warning Signs Requiring Prompt Assessment
Seek prompt ophthalmic care if you develop:
- Significant eye pain
- Reduced vision
- Marked sensitivity to light
- A white spot on the cornea
- Thick discharge
- Severe or one-sided redness
- Rapidly increasing eyelid swelling
- Fever or redness spreading around the eye
- Eye injury or chemical exposure
- A painful red eye while wearing contact lenses
These symptoms may indicate keratitis, cellulitis or another condition requiring urgent treatment.
Frequently Asked Questions
Is blepharitis contagious?
Ordinary chronic blepharitis is generally not considered contagious. However, good hygiene remains important, and towels, eye makeup and contact-lens equipment should not be shared.
Is blepharitis caused by poor hygiene?
Not necessarily.
Poor cleansing may allow crusts and debris to accumulate, but blepharitis also occurs in people with excellent hygiene because of skin disease, gland dysfunction, inflammation or Demodex.
Can blepharitis be cured permanently?
Blepharitis is often chronic and may recur. Symptoms can usually be controlled with consistent care and treatment directed at the underlying cause.
Is blepharitis the same as dry eye?
No.
Blepharitis affects the eyelid margins, while dry-eye disease involves the tear film and ocular surface. However, the two conditions frequently occur together.
Is blepharitis the same as meibomian gland dysfunction?
No.
Meibomian gland dysfunction affects the eyelid oil glands and is a major cause of posterior blepharitis. A patient may have MGD, anterior blepharitis or both.
Can blepharitis cause eyelashes to fall out?
Yes. Chronic inflammation may cause lash loss, breakage or abnormal direction of growth. Persistent localised lash loss should be examined to exclude other eyelid disease.
Should I stop wearing contact lenses?
During an active flare—particularly if there is redness, pain or blurred vision—it is generally sensible to stop wearing lenses until the eyes have been assessed and are comfortable again.
The Bottom Line
Blepharitis is chronic inflammation of the eyelid margins.
It may be related to:
- Bacteria around the eyelashes
- Seborrhoeic dermatitis
- Meibomian gland dysfunction
- Rosacea
- Demodex mites
- Allergy or environmental irritation
Treatment begins with consistent eyelid hygiene, but additional therapy should be directed at the underlying cause.
Warm compresses may help blocked oil glands. Antibiotics or anti-inflammatory medication may be appropriate for selected patients. Demodex requires targeted therapy, while rosacea and dandruff may require simultaneous skin treatment.
Blepharitis often cannot be permanently cured, but it can usually be controlled. Early, consistent and cause-directed care helps reduce flare-ups, stabilise the tear film and protect the cornea.
References
- American Academy of Ophthalmology. Blepharitis Preferred Practice Pattern. 2024.
- National Eye Institute. Blepharitis: Symptoms, Causes, Diagnosis and Treatment. Updated 2024.
- Jones L, et al. TFOS DEWS III: Management and Therapy. American Journal of Ophthalmology. 2025.
- Wolffsohn JS, et al. TFOS DEWS III: Diagnostic Methodology. American Journal of Ophthalmology. 2025.
- Yeu E, et al. Lotilaner Ophthalmic Solution 0.25% for the Treatment of Demodex Blepharitis. Clinical trial reports.
- US Food and Drug Administration. Lotilaner Ophthalmic Solution 0.25% Prescribing Information and Clinical Review.