Author: Dr Val Phua
Estimated reading time: 10–12 minutes
There Is No Single “Best” Myopia Treatment
One of the first questions parents ask after their child is diagnosed with short-sightedness (myopia) is:
“Which treatment works best?”
The answer is not the same for every child.
Modern myopia management offers several evidence-based treatments that can slow the progression of myopia. The most appropriate option depends on your child’s age, prescription, lifestyle, rate of progression and individual eye characteristics.
The goal is not simply to reduce the need for stronger glasses each year—it is to reduce the lifetime risk of serious eye diseases associated with high myopia.
Why Is Myopia Control Important?
Myopia develops because the eye grows too long from front to back.
As the eye continues to elongate, the risk of future eye disease increases.
High myopia is associated with a greater risk of:
- Retinal detachment
- Myopic macular degeneration
- Glaucoma
- Cataracts
- Myopic traction maculopathy
Slowing eye growth during childhood may help reduce these long-term risks.
The Four Main Evidence-Based Treatments
1. Low-Dose Atropine Eye Drops
Atropine is one of the most widely studied medical treatments for childhood myopia.
A small drop is placed into each eye once daily, usually at night, to help slow eye growth.
Best suited for:
- Younger children
- Early-onset myopia
- Rapid progression
- Families who prefer not to use contact lenses
Advantages
- Strong scientific evidence
- Easy to use
- Well tolerated
- Minimal lifestyle restrictions
Considerations
- Daily treatment is required
- Regular follow-up is needed
- Some children may require combination therapy
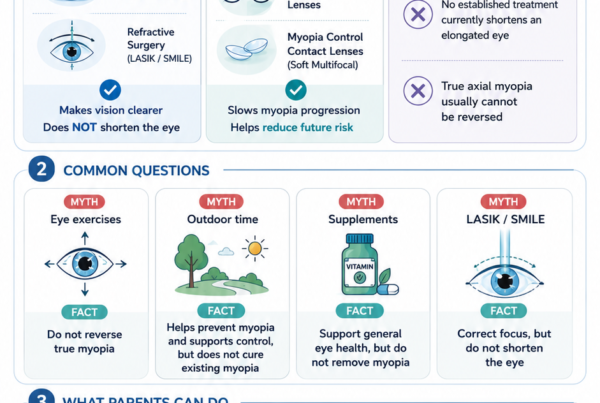
2. Orthokeratology (Ortho-K)
Orthokeratology uses specially designed contact lenses worn overnight.
The lenses temporarily reshape the cornea, allowing clear daytime vision without glasses while also helping slow myopia progression.
Best suited for:
- Active children
- Children involved in sports
- Those who prefer not to wear glasses during the day
Advantages
- Clear daytime vision
- Effective myopia control
- Excellent for sports
Considerations
- Good lens hygiene is essential
- Requires regular reviews
- Small risk of contact lens-related infection
3. Defocus Spectacle Lenses
Modern spectacle lenses are specially designed to both correct vision and reduce the stimulus for excessive eye growth.
Examples include DIMS and Highly Aspherical Lenslet (HAL) technology.
Best suited for:
- Younger children
- Families preferring spectacles
- Children not ready for contact lenses
Advantages
- Easy to use
- Non-invasive
- No eye drops required
Considerations
- Glasses should be worn consistently
- More expensive than standard lenses
4. Soft Myopia Control Contact Lenses
These specially designed daily disposable lenses create peripheral myopic defocus while providing excellent daytime vision.
Best suited for:
- Older children
- Responsible contact lens wearers
- Children wanting an alternative to glasses
Advantages
- Comfortable
- Daytime freedom from spectacles
- Evidence-based myopia control
Considerations
- Daily lens handling
- Good hygiene required
- Not suitable for every child
Can Treatments Be Combined?
Yes.
Children with rapidly progressing myopia sometimes benefit from combination therapy.
Examples include:
- Low-dose atropine + Orthokeratology
- Low-dose atropine + Defocus spectacle lenses
- Low-dose atropine + Soft myopia control contact lenses
Combination therapy may offer additional benefit in selected children, although treatment should always be individualised.
Lifestyle Still Matters
No treatment works in isolation.
Parents should also encourage:
- Around 2 hours of outdoor activity daily, where practical
- Regular breaks during prolonged near work
- A comfortable reading distance
- Balanced recreational screen use
- Adequate sleep
- Regular eye examinations
Healthy habits complement medical treatment.
Comparison of Myopia Control Treatments
| Treatment | Slows Myopia Progression | Daytime Glasses Needed | Contact Lenses | Daily Eye Drops | Suitable for Younger Children |
|---|---|---|---|---|---|
| Low-dose atropine | ✅ | Usually yes | ❌ | ✅ | ✅ |
| Orthokeratology | ✅ | Usually no | Overnight | ❌ | Selected children |
| Defocus spectacle lenses | ✅ | ✅ | ❌ | ❌ | ✅ |
| Soft myopia control contact lenses | ✅ | No | Day wear | ❌ | Older children |
Which Treatment Do I Usually Recommend?
Rather than asking “Which treatment is the strongest?”, a better question is:
“Which treatment is the best fit for my child?”
When recommending treatment, I consider:
- Age
- Degree of myopia
- Rate of progression
- Corneal shape
- Lifestyle
- Sporting activities
- Ability to comply with treatment
- Family preferences
Every child is different, and treatment should be personalised rather than adopting a one-size-fits-all approach.
Frequently Asked Questions
Which treatment slows myopia the most?
No single treatment is superior for every child. Clinical studies show that atropine, orthokeratology, defocus spectacle lenses and soft myopia control contact lenses can all significantly slow myopia progression. The response varies from one child to another.
Can my child switch treatments later?
Yes.
Treatment plans are often adjusted as children grow or if myopia progresses despite therapy.
Will my child still need glasses?
Usually yes.
The aim is to slow progression, not eliminate the need for vision correction.
Should treatment start immediately?
In many children, early treatment offers the greatest long-term benefit, especially if myopia develops at a young age or progresses rapidly.
The Bottom Line
There is no universal “best” treatment for childhood myopia. Instead, the most effective approach is one that matches your child’s eyes, lifestyle and risk of progression.
Evidence-based treatments—including low-dose atropine, orthokeratology, defocus spectacle lenses and soft myopia control contact lenses—can all play an important role in slowing myopia progression. Combined with healthy visual habits, regular outdoor activity and routine eye examinations, these treatments help protect your child’s vision both now and in the future.
References
- International Myopia Institute. IMI Clinical Management Guidelines and White Papers.
- World Society of Paediatric Ophthalmology and Strabismus. Consensus Statement on Myopia Management.
- American Academy of Ophthalmology. Myopia in Children.
- Brien Holden Vision Institute. Evidence-Based Myopia Control.
- Singapore Eye Research Institute. Clinical Research on Childhood Myopia and Myopia Control.