Author: Dr Val Phua
Estimated reading time: 17 minutes
LASIK and SMILE are two established forms of laser vision correction used to reduce dependence on spectacles and contact lenses.
Both procedures permanently reshape the cornea so that light focuses more accurately on the retina. In appropriately selected patients, both can provide excellent unaided vision, high refractive accuracy and long-term stability.
The principal difference is how the corneal tissue is treated:
- LASIK creates a thin corneal flap. An excimer laser then reshapes the underlying corneal tissue.
- SMILE uses a femtosecond laser to create a small lens-shaped piece of tissue—called a lenticule—within the cornea. The surgeon removes this lenticule through a small incision without creating a LASIK-style flap.
Comparative studies generally find that LASIK and SMILE produce similar final visual acuity, safety and refractive accuracy for myopia and myopic astigmatism. The choice usually depends on the patient’s corneal anatomy, prescription, dry-eye status, occupation, sporting activities, treatment customisation needs and tolerance for the different risks of each procedure. [1–5]
LASIK vs SMILE at a Glance
LASIK May Be Favoured When:
- Very rapid initial visual recovery is a priority
- Wavefront-guided or topography-guided treatment is desirable
- Hyperopia or mixed astigmatism requires correction
- A future enhancement may be more likely
- The surgeon wants direct access to the treatment bed
- The cornea and tear film are suitable for flap-based treatment
SMILE May Be Favoured When:
- Avoiding a corneal flap is important
- The patient participates in contact or impact sports
- Dry-eye risk is a major concern
- Preserving more anterior corneal nerves is desirable
- Myopia with or without regular astigmatism is being treated
- The patient’s corneal anatomy and prescription fit the available treatment range
Neither list replaces a comprehensive refractive assessment.
What Is LASIK?
LASIK stands for Laser-Assisted In Situ Keratomileusis.
Modern femtosecond LASIK generally uses two lasers:
- A femtosecond laser creates a thin, hinged corneal flap.
- The surgeon lifts the flap.
- An excimer laser removes microscopic amounts of tissue from the underlying corneal stroma.
- The flap is repositioned over the treated area.
The excimer laser reshapes the cornea by removing tissue according to the patient’s prescription and treatment plan.
For myopia, the central cornea is flattened. For hyperopia, the mid-peripheral cornea is reshaped to make the centre relatively steeper. Astigmatism is treated by applying different amounts of correction across different meridians. [6]
What Is Bladeless or Femto-LASIK?
Bladeless LASIK means that the corneal flap is created with a femtosecond laser rather than a mechanical microkeratome blade.
The second stage still uses an excimer laser to reshape the cornea.
Femtosecond-laser flap creation allows the surgeon to plan:
- Flap diameter
- Flap thickness
- Hinge position
- Side-cut angle
- Flap shape
Most modern LASIK procedures are performed using femtosecond-laser flap creation.
What Is SMILE?
SMILE stands for Small-Incision Lenticule Extraction.
The procedure uses a femtosecond laser to create:
- A thin, lens-shaped lenticule inside the cornea
- A small access incision at the surface of the cornea
The surgeon separates and removes the lenticule through the incision.
Removing this tissue changes the shape of the cornea and corrects the myopia and astigmatism.
Unlike LASIK:
- No broad corneal flap is created
- No excimer laser ablation is performed
- The central anterior corneal surface remains largely intact apart from the small incision
The United States FDA-approved SMILE indication includes myopia from −1.00 to −10.00 D, with astigmatism from −0.75 to −3.00 D, in adults aged 22 years or older with a stable prescription. Regulatory indications and available treatment ranges may differ in Singapore and other countries. [7,8]
What Is a Corneal Lenticule?
A lenticule is a precisely shaped piece of corneal stromal tissue.
Its:
- Thickness
- Diameter
- Shape
- Astigmatic orientation
are determined by the intended refractive correction.
For myopia, the lenticule is thicker centrally. Removing it flattens the central cornea and reduces its focusing power.
The tissue removal is permanent. SMILE should therefore not be described as reversible. [7]
What Is the Main Difference Between LASIK and SMILE?
The main structural difference is the corneal access method.
LASIK
- Creates a broad hinged flap
- Uses an excimer laser beneath the flap
- Provides direct access to the stromal treatment bed
- Allows wavefront- or topography-guided excimer treatment on appropriate platforms
- Leaves a permanent flap interface
SMILE
- Creates an internal lenticule
- Removes the lenticule through a small incision
- Avoids a LASIK-style flap
- Uses only the femtosecond laser for the refractive treatment
- Leaves a cap and internal interface rather than a hinged flap
Both procedures permanently remove corneal tissue.
Which Gives Better Vision: LASIK or SMILE?
For appropriately selected patients with myopia or myopic astigmatism, final visual outcomes are generally similar.
Comparative studies and meta-analyses have found broadly comparable:
- Unaided distance visual acuity
- Best-corrected visual acuity
- Refractive predictability
- Safety
- Astigmatism correction
- Patient satisfaction
A 2024 paired-eye study found similar unaided and corrected vision between SMILE and femtosecond LASIK at up to one year. A separate three-year comparison concluded that both were safe and similarly effective for myopia and astigmatism. [1,4]
The result depends more on:
- Patient selection
- Accuracy of the refraction
- Corneal measurements
- Treatment centration
- Optical-zone planning
- Laser platform
- Surgical technique
- Postoperative healing
than on the procedure name alone.
Which Has Faster Visual Recovery?
LASIK generally provides faster initial visual recovery.
Many LASIK patients see substantially better within several hours and have functional vision by the following day.
SMILE recovery is also relatively quick, but vision may take slightly longer to become crisp. Some patients notice:
- Mild haziness
- Fluctuating vision
- Reduced contrast
- A difference between the two eyes
- Slower recovery of very fine detail
during the first few days.
A prospective randomised contralateral-eye study found that wavefront-guided LASIK provided faster visual recovery and better early low-contrast visual acuity than SMILE. Reviews have similarly found that early visual recovery may be slower after SMILE, although final results generally become comparable. [9,10]
Typical Functional Recovery
Many patients can return to office-based activities:
- Within one or two days after LASIK
- Within a few days after SMILE
Individual recovery varies. Driving should resume only when vision is legally adequate and the surgeon has confirmed that it is safe.
Is LASIK More Painful Than SMILE?
Both procedures are performed using anaesthetic eyedrops and should not cause sharp pain during surgery.
Patients may feel:
- Pressure
- Tightness
- Bright lights
- Water around the eye
- Temporary loss or dimming of vision during laser docking
After LASIK, tearing, burning and light sensitivity may be most noticeable during the first several hours.
After SMILE, mild grittiness, watering or light sensitivity may occur. Some patients experience slightly more prolonged visual haze even when discomfort is mild.
Severe or increasing pain is not considered a normal feature of either recovery.
Which Procedure Causes Less Dry Eye?
SMILE generally causes less disruption to the anterior corneal nerves and may produce less early postoperative dry eye than LASIK.
The corneal nerves help regulate:
- Tear production
- Blinking
- Corneal sensation
- Eye-surface healing
Creating a broad LASIK flap cuts more of the superficial corneal nerve network. SMILE uses a smaller incision and preserves more of the anterior corneal surface.
A 2025 meta-analysis of 18 studies found better tear-film stability and some tear-production measurements after lenticule extraction compared with femtosecond LASIK. Earlier meta-analyses also found faster corneal-sensitivity recovery and fewer early dry-eye symptoms after SMILE. [2,11,12]
However:
- SMILE can still cause dry eye
- LASIK dry eye is often temporary
- Differences may become smaller over time
- Pre-existing meibomian gland dysfunction may be more important than the procedure itself
- Severe dry eye can make either procedure unsuitable
Dry-eye disease, blepharitis and eyelid-gland dysfunction should be treated before surgery.
Does SMILE Completely Avoid Corneal-Nerve Damage?
No.
The SMILE laser still creates:
- An anterior cap interface
- A posterior lenticule interface
- A small incision
- Disruption of stromal nerves within the treated area
The difference is one of degree and distribution rather than complete nerve preservation.
Corneal sensation generally recovers after either procedure, but recovery may occur earlier after SMILE.
What Is the LASIK Flap?
The LASIK flap is a thin layer of corneal tissue that remains attached by a hinge.
Once repositioned, the flap adheres without stitches.
The surface epithelium seals relatively quickly, but the deeper flap interface does not regain the same tensile strength as untouched corneal tissue.
This creates several LASIK-specific considerations:
- Flap displacement
- Flap folds or striae
- Epithelial ingrowth
- Interface inflammation
- Diffuse lamellar keratitis
- Trauma-related flap movement
These complications are uncommon with modern femtosecond LASIK but are not possible in exactly the same form after flap-free SMILE.
Can a LASIK Flap Move Years Later?
Significant late movement is uncommon, but severe trauma can disturb a LASIK flap even years after surgery.
Risk is most relevant for people exposed to:
- Direct blows to the eye
- Fingernail injuries
- Martial arts
- Boxing
- Contact sports
- Military or tactical activities
- Occupations involving facial trauma
Most LASIK patients resume normal activities without flap problems. Nevertheless, patients with a high lifetime risk of direct eye trauma may prefer SMILE or a surface-ablation procedure.
Is SMILE Better for Contact Sports?
SMILE may be attractive for contact-sport athletes because there is no broad corneal flap to displace.
Potentially relevant activities include:
- Martial arts
- Boxing
- Rugby
- Football
- Basketball
- Water polo
- Military training
- Law-enforcement work
However, SMILE does not make the eye immune to injury. Trauma can still cause:
- Corneal abrasions
- Inflammation
- Retinal tears
- Retinal detachment
- Other internal eye injuries
Protective eyewear remains advisable whenever practical.
Which Procedure Preserves More Corneal Strength?
SMILE is designed to preserve more of the anterior stromal architecture because it avoids a broad flap.
The anterior corneal stromal fibres are considered to contribute significantly to corneal strength. In LASIK, these fibres are cut during flap creation and do not contribute fully to the load-bearing residual stromal bed.
In SMILE, most of the anterior surface remains continuous apart from the small incision.
Biomechanical models therefore suggest that SMILE may preserve more corneal strength for an equivalent correction.
However, the clinical difference is complex and should not be overstated.
Corneal strength after either procedure depends on:
- Preoperative corneal shape
- Corneal thickness
- Treatment depth
- Optical-zone diameter
- Cap or flap thickness
- Prescription
- Residual stromal tissue
- Undetected keratoconus susceptibility
- Individual wound healing
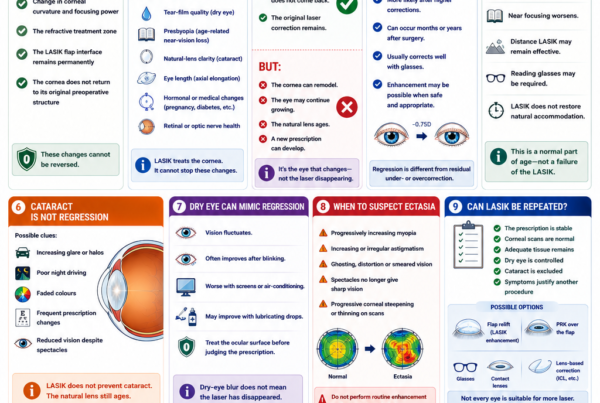
Can Corneal Ectasia Occur After LASIK or SMILE?
Yes.
Corneal ectasia is progressive weakening and bulging of the cornea after refractive surgery.
It may cause:
- Increasing myopia
- Increasing irregular astigmatism
- Ghosting
- Reduced best-corrected vision
- Difficulty wearing standard spectacles
- Need for rigid or scleral contact lenses
- Need for corneal cross-linking
A systematic review found reported post-refractive ectasia after LASIK, PRK and SMILE. The reported incidence appeared lower after SMILE than after LASIK, but the authors cautioned that SMILE had a shorter history, fewer total procedures and incomplete case reporting. The presence of pre-existing or forme-fruste keratoconus remained an important factor. [13]
No procedure eliminates ectasia risk.
The most important protection is careful preoperative screening.
Is SMILE Always Safer for a Thin Cornea?
No.
Although SMILE avoids a LASIK flap, it still removes corneal stromal tissue.
Suitability depends on:
- Total corneal thickness
- Cap thickness
- Lenticule thickness
- Residual stromal thickness
- Corneal tomography
- Epithelial thickness mapping
- Biomechanical assessment
- Degree of correction
A thin or suspicious cornea may be unsuitable for both LASIK and SMILE.
Alternative options may include:
- PRK or surface ablation
- ICL surgery
- Spectacles
- Contact lenses
- No surgery
Which Procedure Can Treat a Wider Range of Prescriptions?
LASIK generally offers greater treatment flexibility.
Depending on the laser platform and local approval, LASIK can treat:
- Myopia
- Hyperopia
- Myopic astigmatism
- Hyperopic astigmatism
- Mixed astigmatism
- Monovision targets
The FDA-approved MEL 90 LASIK indication includes myopia, hyperopia and mixed astigmatism within specified ranges. [6]
SMILE is primarily used for:
- Myopia
- Myopic astigmatism
Under current United States FDA labelling, SMILE is approved for myopia from −1.00 to −10.00 D and cylinder from −0.75 to −3.00 D. Local approved ranges may differ. [7,8]
Can SMILE Treat Hyperopia?
Hyperopic lenticule extraction is being studied and may be available in limited settings or under different regulatory frameworks.
However, SMILE remains predominantly established and approved for myopia with or without astigmatism.
LASIK currently has a more established role for hyperopia and mixed astigmatism.
Which Procedure Is Better for High Myopia?
Both LASIK and SMILE may correct high myopia when the cornea is sufficiently thick, regular and structurally suitable.
As the intended myopic correction increases:
- More corneal tissue must be removed
- The residual stromal tissue becomes thinner
- Regression may become more likely
- Optical-zone planning becomes more challenging
- Night-vision symptoms may become more relevant
- Ectasia risk must be assessed carefully
SMILE has shown stable outcomes in many moderate- and high-myopia studies, including follow-up extending to five, seven and ten years. However, some long-term studies found greater regression or less predictable remodelling in higher-myopia groups. [14–18]
LASIK also has extensive long-term evidence, but high corrections can show refractive regression and may require enhancement.
For very high myopia, thin corneas or borderline tissue calculations, an ICL may provide a safer alternative because it corrects the prescription without removing central corneal tissue.
Which Procedure Corrects Astigmatism Better?
Both procedures can effectively correct regular myopic astigmatism.
The result depends on:
- Accuracy of the measured cylinder
- Axis consistency
- Treatment centration
- Cyclotorsion
- Corneal healing
- Laser platform
- Degree of astigmatism
LASIK platforms may offer:
- Iris registration
- Cyclotorsion compensation
- Wavefront-guided correction
- Topography-guided correction
SMILE requires accurate docking, centration and lenticule orientation. Newer systems may provide digital alignment assistance, but available features vary by platform and market.
Comparative studies generally show similar overall cylinder correction, although results may differ in specific groups such as high or oblique astigmatism. [1,4,19]
What Is Wavefront-Guided LASIK?
Wavefront-guided LASIK uses measurements of the eye’s optical aberrations to create a customised excimer-laser treatment.
The aim is to correct the spectacle prescription while reducing the induction of additional higher-order aberrations.
It may be useful when:
- Preoperative wavefront measurements are reliable
- The optical system shows particular aberration patterns
- Night vision and low-contrast performance are priorities
- The pupil and treatment zone are appropriately planned
A randomised contralateral-eye study found faster early visual recovery and better low-contrast performance with wavefront-guided LASIK than SMILE, although both procedures provided marked visual improvement. [9]
What Is Topography-Guided LASIK?
Topography-guided LASIK uses detailed corneal surface measurements to plan treatment.
It may help address:
- Corneal asymmetry
- Decentration
- Certain regular optical irregularities
- Corneal higher-order aberrations
Topography-guided treatment is not appropriate for every irregular cornea and should not be used to conceal progressive keratoconus.
LASIK currently provides broader established options for wavefront- or topography-guided customisation than standard SMILE.
Is SMILE Less Accurate Because It Is Not Wavefront-Guided?
Not necessarily.
Standard prescriptions can be corrected very accurately using either procedure.
Most comparative studies find similar final visual acuity and refractive predictability.
Customisation becomes more relevant when a patient has:
- Significant corneal asymmetry
- Large pupils
- Previous refractive surgery
- Significant higher-order aberrations
- Unusual visual-quality complaints
In such cases, a customised LASIK or surface-ablation strategy may offer planning options that conventional SMILE does not.
Which Procedure Has Better Night Vision?
Most patients have satisfactory night vision after either procedure.
Both can temporarily or persistently cause:
- Glare
- Halos
- Starbursts
- Ghosting
- Reduced contrast sensitivity
- Difficulty driving at night
Risk is influenced by:
- Pupil size
- Optical-zone diameter
- Degree of correction
- Treatment centration
- Residual astigmatism
- Dry eye
- Higher-order aberrations
- Pre-existing night-vision symptoms
The FDA notes that visual symptoms such as glare, halos and double vision can occur after LASIK, even when standard eye-chart vision is good. The SMILE patient booklet similarly states that the procedure is not risk-free and that patients may lose some lines of vision or require further correction. [7,20]
There is no universal rule that LASIK or SMILE always provides better night vision. The treatment plan and individual eye are more important.
Does LASIK Have Better Centration?
LASIK excimer-laser systems may include active eye tracking and iris-registration technology.
These systems can compensate for:
- Small eye movements
- Cyclotorsion
- Pupil-centre shifts
- Differences between upright and lying positions
SMILE involves docking the eye to the femtosecond laser. Accurate initial centration is therefore important because the lenticule pattern is created during docking.
Experienced surgeons use:
- Visual-axis assessment
- Corneal reflexes
- Pupil position
- Fixation behaviour
- Digital guidance where available
Both procedures can be centred accurately, but the mechanisms differ.
Which Procedure Is Easier to Enhance?
LASIK generally offers a more straightforward enhancement pathway.
If a residual prescription remains after LASIK, the surgeon may sometimes:
- Relift the existing flap
- Apply additional excimer-laser treatment
- Perform PRK over the flap
- Use spectacles or contact lenses
Flap relifting is not always advisable, particularly many years later, because epithelial ingrowth and other flap-related risks may increase.
Enhancement After SMILE
After SMILE, enhancement options may include:
- PRK over the SMILE cap
- Converting the SMILE cap into a LASIK-style flap using a specialised laser pattern
- Repeat lenticule extraction in selected cases
- Spectacles or contact lenses
- ICL in selected eyes
A review of PRK enhancement after SMILE reported that enhancement is generally uncommon and that PRK can be effective when a suitable residual prescription remains. [21]
SMILE enhancement is feasible, but it is generally less direct than lifting a recent LASIK flap.
How Often Is an Enhancement Needed?
Enhancement rates vary with:
- Preoperative prescription
- Age
- Laser platform
- Treatment nomogram
- Healing
- Definition of enhancement
- Length of follow-up
- Surgeon threshold for re-treatment
Higher prescriptions and longer follow-up generally increase the chance of residual or recurrent refractive error.
A small residual prescription does not necessarily mean the operation has failed. It may be managed with spectacles for specific tasks when unaided vision remains satisfactory.
Which Is Better for Someone With Dry Eyes?
SMILE may be preferred when the patient has mild-to-moderate dry-eye risk but otherwise healthy ocular anatomy.
However, the underlying cause of dryness matters.
A patient with:
- Severe aqueous-deficient dry eye
- Significant meibomian gland dysfunction
- Active blepharitis
- Exposure keratopathy
- Autoimmune-related ocular-surface disease
- Corneal staining
may be unsuitable for either procedure until the eye surface is adequately treated.
The FDA SMILE booklet lists severe dry eye as a contraindication. The FDA also warns that LASIK can worsen dry-eye symptoms. [7,20]
Which Is Better for Someone With a Thin Cornea?
Neither procedure can be selected from corneal thickness alone.
The surgeon must consider:
- Corneal tomography
- Epithelial thickness
- Total tissue removal
- Flap or cap thickness
- Residual stromal tissue
- Percentage tissue altered
- Biomechanical risk
- Prescription
A thin but regular cornea may sometimes be suitable for:
- SMILE
- Thin-flap LASIK
- PRK
- ICL
depending on the complete assessment.
A thin cornea with suspicious tomography may be unsuitable for all corneal laser procedures.
Which Is Better for Someone With Keratoconus?
Neither LASIK nor SMILE is appropriate for progressive keratoconus.
Both permanently remove corneal tissue and can worsen structural instability.
Patients with suspected or established keratoconus may require:
- Observation
- Corneal cross-linking
- Specialised contact lenses
- Intracorneal ring segments in selected cases
- ICL for residual refractive error after the cornea is stable
- Other corneal treatment
Even stable or mild keratoconus requires specialist evaluation before any elective refractive procedure.
Can LASIK or SMILE Treat Presbyopia?
Neither procedure restores natural accommodation.
Both may be used in a monovision strategy:
- One eye is targeted for distance
- The other eye retains mild myopia for near or intermediate vision
Potential disadvantages include:
- Reduced depth perception
- Reduced stereoacuity
- Night-driving difficulty
- Eye imbalance
- Incomplete near vision
A contact-lens monovision trial is advisable before surgery whenever practical.
Patients corrected fully for distance may require reading glasses as presbyopia develops. Both FDA patient booklets emphasise that laser correction does not eliminate the future need for reading glasses. [6,7]
Are LASIK and SMILE Permanent?
Yes.
Both procedures permanently remove corneal tissue.
They cannot be reversed by replacing the removed tissue.
However, the eye can continue to change because of:
- Myopia progression
- Presbyopia
- Cataract
- Corneal remodelling
- Hormonal changes
- Diabetes-related refractive shifts
- Other eye disease
A permanent procedure does not guarantee a permanently unchanged prescription.
What Are the Main Risks of LASIK?
LASIK risks include:
- Dry eye
- Under- or overcorrection
- Residual astigmatism
- Glare, halos or ghosting
- Flap displacement
- Flap folds or striae
- Epithelial ingrowth
- Diffuse lamellar keratitis
- Infection
- Interface debris
- Corneal ectasia
- Loss of best-corrected vision
- Need for enhancement
- Persistent neuropathic corneal pain in rare cases
The FDA advises that some patients develop significant visual symptoms, reduced low-contrast vision or ongoing dryness despite good standard visual acuity. [20]
What Are the Main Risks of SMILE?
SMILE risks include:
- Dry eye
- Under- or overcorrection
- Residual astigmatism
- Glare, halos or ghosting
- Suction loss during treatment
- Difficult lenticule separation
- Retained lenticule tissue
- Cap perforation or tear
- Interface inflammation
- Interface debris
- Infection
- Corneal ectasia
- Decentration
- Loss of best-corrected vision
- Need for enhancement
The absence of a flap removes flap-specific complications but does not make SMILE risk-free. [7]
What Happens if Suction Is Lost During SMILE?
The eye is docked to the femtosecond laser during lenticule creation.
If suction is lost, management depends on:
- How far the laser treatment has progressed
- Which cutting plane was being created
- The laser platform
- The appearance of the tissue planes
- Surgeon experience
The procedure may be:
- Restarted
- Completed with an adjusted plan
- Converted to another procedure
- Postponed
Suction loss is uncommon with modern systems but remains a recognised SMILE-specific event.
Which Procedure Has More Long-Term Evidence?
LASIK has the longer overall clinical history.
LASIK has been performed widely since the 1990s, and long-term studies extend beyond 20 years for some patients and platforms.
SMILE was introduced later, but published evidence now includes:
- Five-year studies
- Seven-year studies
- Multiple ten-year studies
Ten-year SMILE studies generally support long-term safety and effectiveness, although some refractive regression may occur, particularly after higher corrections. [15–18]
A review of long-term PRK, LASIK and SMILE evidence concluded that all three can provide high long-term safety within suitable treatment ranges, without a clear universal winner. [22]
Does One Procedure Regress More?
Refractive regression can occur after both procedures.
Risk may be influenced by:
- High preoperative myopia
- Younger age
- Ongoing axial elongation
- Corneal healing
- Optical-zone size
- Natural-lens changes
- Hormonal or metabolic factors
Some comparative long-term studies have found similar stability, while others have reported slightly more favourable outcomes for one procedure within their particular patient populations.
A seven-year comparative study found good predictability with both SMILE and femtosecond LASIK and reported some refractive advantages for SMILE. These findings do not establish that SMILE will be more stable in every patient. [5]
Who May Be Suitable for Either Procedure?
A typical suitable candidate has:
- A stable prescription
- Adequate age and refractive maturity
- Healthy corneas
- Normal or acceptably stable corneal tomography
- Adequate corneal thickness
- Controlled dry-eye disease
- No significant cataract
- No active infection or inflammation
- Realistic expectations
- Willingness to attend follow-up
Who May Not Be Suitable?
LASIK and SMILE may be unsuitable when there is:
- Progressive keratoconus
- Suspicious corneal tomography
- Inadequate residual stromal tissue
- Severe dry eye
- Active blepharitis or eye-surface inflammation
- Active eye infection
- Unstable refraction
- Pregnancy or breastfeeding
- Uncontrolled diabetes
- Active autoimmune or connective-tissue disease
- Significant cataract
- Vision-limiting retinal or optic nerve disease
- Unrealistic expectations
The precise contraindications depend on the patient, laser platform and applicable regulatory guidance. [6–8,20]
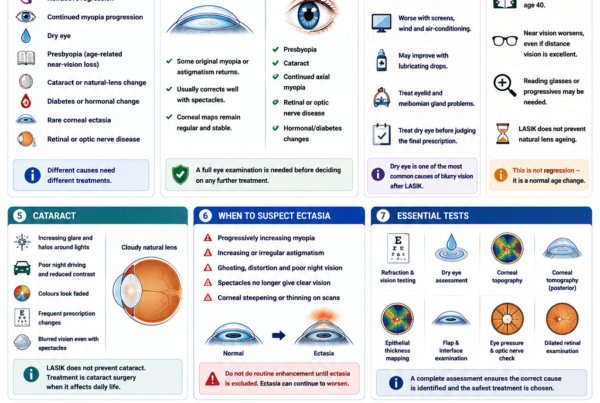
What Tests Are Required Before LASIK or SMILE?
Refraction and Visual Acuity
The assessment measures:
- Myopia or hyperopia
- Astigmatism
- Best-corrected vision
- Prescription stability
Cycloplegic refraction may be used to relax accommodation in selected patients.
Corneal Topography and Tomography
These scans assess:
- Corneal shape
- Front and back corneal elevation
- Pachymetry distribution
- Keratoconus risk
- Corneal asymmetry
- Treatment centration
Corneal Thickness
The surgeon calculates whether enough corneal tissue will remain after treatment.
Epithelial Thickness Mapping
Epithelial mapping may help identify:
- Early keratoconus patterns
- Corneal irregularity
- Contact lens warpage
- Localised epithelial compensation
Corneal Biomechanical Assessment
Devices such as dynamic Scheimpflug imaging may provide additional information about deformation behaviour.
No single test can guarantee that ectasia will not occur.
Dry-Eye and Eyelid Assessment
The examination may evaluate:
- Tear-film stability
- Corneal staining
- Tear production
- Meibomian glands
- Blepharitis
- Allergy
Pupil Size
Large pupils may increase the relevance of optical-zone planning and night-vision counselling.
Eye Pressure and Optic Nerve
Glaucoma and ocular hypertension should be identified before elective surgery.
Dilated Retinal Examination
This is particularly important in moderate and high myopia.
Laser vision correction does not remove the retinal risks associated with an elongated eye.
LASIK May Be the Better Choice When:
- The patient wants the fastest possible early visual recovery
- Hyperopia or mixed astigmatism requires correction
- Wavefront-guided treatment is appropriate
- Topography-guided treatment is desirable
- A straightforward enhancement pathway is important
- There is no significant dry-eye or trauma concern
- The cornea is suitable for a flap
SMILE May Be the Better Choice When:
- Avoiding a flap is a major priority
- The patient plays contact sports
- Dry-eye risk is a concern
- Myopia or myopic astigmatism is within the suitable range
- The cornea is suitable for lenticule extraction
- A slightly slower early visual recovery is acceptable
- Extensive customised excimer treatment is not required
PRK May Be Better Than Both When:
- The cornea is unsuitable for a LASIK flap
- Surface treatment preserves a safer residual structure
- The patient can accept slower recovery
- Avoiding both a flap and an internal lenticule interface is preferred
- A customised excimer treatment is required
ICL May Be Better Than Both When:
- The myopia is very high
- Corneal tissue is insufficient
- Corneal tomography is unsuitable for laser correction
- Preserving central corneal tissue is important
- The internal eye anatomy is suitable for an implant
ICL introduces intraocular risks and requires different long-term monitoring.
Frequently Asked Questions About LASIK vs SMILE
Is SMILE Safer Than LASIK?
SMILE avoids flap-specific complications and may cause less early dry eye.
LASIK provides faster early recovery and broader customisation.
Both have uncommon but potentially serious risks, including infection, ectasia and loss of best-corrected vision.
Which Procedure Gives Sharper Vision?
Final eye-chart vision is generally similar.
Wavefront-guided or topography-guided LASIK may provide advantages for selected optical profiles, while many standard myopic patients achieve equally sharp functional vision with SMILE.
Which Has Faster Recovery?
LASIK usually provides faster initial recovery.
SMILE vision may take several additional days to become fully crisp.
Which Causes Less Dry Eye?
SMILE generally causes less early corneal denervation and may produce less early postoperative dryness.
Neither procedure eliminates dry-eye risk.
Which Is Better for Contact Sports?
SMILE is often favoured because it avoids a corneal flap.
Which Is Better for High Myopia?
Either may be suitable when the cornea is sufficiently healthy and thick.
ICL should also be considered when a high correction would require excessive corneal tissue removal.
Which Is Better for Astigmatism?
Both can correct regular myopic astigmatism.
LASIK provides broader customisation options on certain platforms.
Can SMILE Correct Long-Sightedness?
SMILE remains primarily established for myopia and myopic astigmatism.
LASIK has a more established role for hyperopia.
Is SMILE Flapless?
Yes, in the sense that it does not create a hinged LASIK flap.
It still creates an anterior corneal cap, internal tissue planes and a small surface incision.
Is SMILE Reversible?
No.
The removed corneal lenticule cannot simply be replaced.
Is LASIK Reversible?
No.
The excimer laser permanently removes corneal tissue.
Can the LASIK Flap Heal Completely?
The flap seals and becomes stable for normal life, but the deeper interface does not regain the strength of untouched corneal tissue.
Can I Rub My Eyes After Surgery?
Eye rubbing should be avoided during early recovery after either procedure.
Habitual vigorous rubbing should also be avoided long term because it may contribute to corneal deformation in susceptible eyes.
Can LASIK or SMILE Cause Blindness?
Severe permanent visual loss is rare but possible.
Potential causes include:
- Infection
- Severe corneal ectasia
- Scarring
- Irregular astigmatism
- Other uncommon complications
Can I Still Need Glasses?
Yes.
Glasses may still be required for:
- A residual prescription
- Night driving
- Reading after presbyopia develops
- Future refractive changes
Which Procedure Is Easier to Enhance?
LASIK generally has a more straightforward enhancement pathway.
SMILE enhancement may involve PRK, cap-to-flap conversion or another technique.
Can I Have LASIK After SMILE?
Potentially.
A SMILE cap can sometimes be converted into a flap, or PRK may be performed over the cornea.
Suitability depends on tissue thickness, anatomy and the residual prescription.
Can I Have SMILE After LASIK?
SMILE is generally not the routine enhancement procedure after LASIK because the existing flap changes the corneal anatomy.
Other enhancement strategies are usually considered.
Does Either Procedure Prevent Presbyopia?
No.
Reading glasses may still be required with age.
Do I Still Need Eye Examinations After Surgery?
Yes.
Regular examinations remain important for:
- Eye pressure
- Glaucoma
- Cataract
- Corneal health
- Retinal health
- Myopia-related complications
Key Takeaway
LASIK and SMILE are both effective forms of laser vision correction.
In most appropriately selected myopic patients, they provide similar final:
- Unaided vision
- Refractive accuracy
- Safety
- Patient satisfaction
LASIK generally offers:
- Faster early visual recovery
- Broader treatment of myopia, hyperopia and mixed astigmatism
- Greater wavefront- and topography-guided customisation
- A more straightforward enhancement pathway
SMILE generally offers:
- No hinged corneal flap
- Less early corneal-nerve disruption
- Potentially fewer early dry-eye symptoms
- Advantages for patients exposed to contact or impact sports
- Good long-term stability for myopia and myopic astigmatism
Neither procedure is universally better.
LASIK may be preferred when rapid recovery, customised optical treatment, hyperopia correction or easier enhancement is important.
SMILE may be preferred when avoiding a flap and reducing early eye-surface disruption are priorities.
Both procedures:
- Permanently remove corneal tissue
- Can cause glare, halos or residual prescription
- Carry a small risk of corneal ectasia
- Do not prevent presbyopia
- Do not eliminate the retinal risks of high myopia
- Require careful preoperative screening
The safest procedure is the one that best matches the patient’s prescription, corneal anatomy, tear-film health, lifestyle and long-term visual priorities.
References
- Zhang Y, et al. Clinical Outcomes of SMILE and Femtosecond LASIK Used to Treat Myopia: A Meta-analysis. 2016. PMID: 27070233.
- Chen KY, et al. Effectiveness of Keratorefractive Lenticule Extraction Compared With Femtosecond LASIK for Dry Eye: A Meta-analysis. 2025. PMID: 40778870.
- Ramirez-Miranda A, et al. Visual and Refractive Outcomes After SMILE Versus Femtosecond LASIK: A Paired-Eye Study. 2024. PMID: 39591576.
- Han T, et al. Three-Year Outcomes of SMILE and Femtosecond LASIK for Myopia and Astigmatism. 2019. PMID: 30061116.
- Zhang L, et al. Seven-Year Refractive Outcomes Comparing SMILE and Femtosecond LASIK. 2024. PMID: 39373787.
- US Food and Drug Administration. ZEISS MEL 90 LASIK Patient Information Booklet. 2024.
- US Food and Drug Administration. ZEISS VisuMax SMILE Patient Information Booklet.
- US Food and Drug Administration. VisuMax Femtosecond Laser SMILE Premarket Approval and Indications for Use.
- Chiang B, et al. Prospective Randomised Contralateral-Eye Comparison of Wavefront-Guided LASIK and SMILE. 2022. PMID: 34788593.
- Lau YTY, et al. Comparison of Visual, Refractive and Ocular-Surface Outcomes Between SMILE and LASIK. 2019. PMID: 31325106.
- Wong AHY, et al. Dry Eyes After SMILE. 2019. PMID: 31490199.
- Zhang Y, et al. Corneal Sensitivity and Dry-Eye Outcomes After SMILE and Femtosecond LASIK. 2016. PMID: 27070233.
- Moshirfar M, et al. Ectasia After Corneal Refractive Surgery: A Systematic Review. 2021. PMID: 34417707.
- Tian M, et al. Five-Year Follow-up of Visual Outcomes and Optical Quality After SMILE. 2021.
- Blum M, et al. Ten-Year Results of Small-Incision Lenticule Extraction. 2019. PMID: 31610002.
- Damgaard IB, et al. Seven-Year Results of SMILE for High Myopia. 2021. PMID: 34661473.
- Pedersen IB, et al. Ten-Year Outcomes Following SMILE for Myopia Up to −10 Dioptres. 2023. PMID: 37194118.
- Zhao GH, et al. Ten-Year Evaluation of Efficacy, Safety and Predictability After SMILE. 2024. PMID: 39525777.
- Liu M, et al. Five-Year Results of SMILE Versus Femtosecond LASIK. 2019. PMID: 30632671.
- US Food and Drug Administration. LASIK: Risks, Patient Selection and Postoperative Expectations.
- Moshirfar M, et al. Photorefractive Keratectomy Enhancement After SMILE. 2022. PMID: 36119391.
- Taneri S, et al. Long-Term Outcomes of PRK, LASIK and SMILE. 2022. PMID: 34241701.