Author: Dr Val Phua
Estimated reading time: 14–16 minutes
What Is Distorted Vision?
Distorted vision means that an object is visible but appears to have the wrong:
- Shape
- Size
- Position
- Angle
- Proportion
- Orientation
The medical term often used for this symptom is metamorphopsia.
Patients may report that:
- Straight lines look wavy
- Doorframes appear bent
- Words look crowded or stretched
- Part of a face appears larger or smaller
- Tiles seem uneven
- A window frame has a bump in it
- Objects seem tilted
- Letters appear displaced
- Part of an image looks compressed
- One section of a picture appears missing
Metamorphopsia is especially associated with diseases affecting the macula, the central retinal area responsible for reading, recognising faces and seeing fine detail. It may also result from corneal irregularity, differences in image size between the eyes or, less commonly, neurological disease.
Is Distorted Vision the Same as Blurred Vision?
No.
Blurred Vision
Blurred vision means an object appears:
- Out of focus
- Hazy
- Smudged
- Less sharp
The object usually retains its normal shape.
Distorted Vision
Distorted vision means the object itself appears:
- Bent
- Wavy
- Stretched
- Shrunken
- Tilted
- Displaced
- Uneven
A patient can have clear visual acuity on an eye chart yet still experience troubling distortion.
Blur and distortion can also occur together.
Is Distorted Vision the Same as Double Vision?
No.
Distorted Vision
A single object appears misshapen.
Double Vision
Two separate or overlapping images of one object are seen.
Macular disease may occasionally produce retinal image misregistration that patients describe as doubling, particularly when each eye sees an image of a different size or position. However, true binocular diplopia usually disappears when either eye is covered and is more often caused by eye misalignment.
Why Is the Macula Important?
The retina is the light-sensitive tissue lining the back of the eye.
The macula is its specialised central area.
It provides the detailed vision required for:
- Reading
- Recognising faces
- Driving
- Using a phone
- Seeing colours
- Sewing
- Drawing
- Performing precise work
When the macula becomes swollen, wrinkled, stretched, displaced or damaged, the arrangement of its light-sensing cells changes.
A straight object may then stimulate retinal cells in an uneven pattern, causing the brain to perceive the line as bent or wavy.
What Does Metamorphopsia Look Like?
Common descriptions include:
- Straight lines appearing curved
- Letters changing size across a sentence
- Words looking compressed
- Faces appearing asymmetrical
- A central portion of an object appearing enlarged
- A part of the image appearing pulled sideways
- Objects looking narrower or wider than normal
- A grid appearing broken or irregular
Macular disorders such as age-related macular degeneration, macular oedema, epiretinal membrane and macular hole commonly produce this type of central distortion.
What Are Micropsia and Macropsia?
Micropsia
Objects appear smaller than they really are.
A patient may notice that:
- A person’s face looks smaller through one eye
- Words appear unusually fine
- Objects seem farther away
- The image from one eye is smaller than the other
Macropsia
Objects appear larger than they really are.
The affected eye may make:
- Letters look enlarged
- Faces appear swollen
- Objects seem closer
- One image look larger than the fellow eye’s image
Micropsia and macropsia are recognised forms of metamorphopsia and may occur when retinal photoreceptors are displaced by swelling, traction or other structural change.
What Is Aniseikonia?
Aniseikonia means that the image appears to be a different size or shape in one eye compared with the other.
Possible causes include:
- A large spectacle-prescription difference
- Retinal swelling
- Epiretinal membrane
- Macular surgery
- Retinal-detachment repair
- Differences in retinal anatomy
- Cataract or refractive surgery
Symptoms may include:
- Eye strain
- Headache
- Difficulty fusing the two images
- Distortion
- Dizziness
- Double vision
- Reduced depth perception
Why Should You Test Each Eye Separately?
One eye may compensate for distortion in the other.
This may delay recognition of a macular problem.
To test:
- Wear the appropriate reading glasses.
- Cover the left eye without pressing on it.
- Look at a doorframe, window frame, printed text or grid.
- Repeat with the right eye covered.
- Compare whether lines, sizes or missing areas differ.
A sudden difference between the eyes requires prompt assessment.
When Is Distorted Vision Urgent?
Arrange prompt or same-day eye assessment when distortion:
- Begins suddenly
- Is new in one eye
- Is rapidly worsening
- Affects the centre of vision
- Is associated with a dark or blank patch
- Is associated with sudden blurred vision
- Is accompanied by flashes or many new floaters
- Is accompanied by a curtain or shadow
- Occurs after eye trauma
- Develops after eye surgery or an injection
- Occurs in a patient with age-related macular degeneration
- Occurs in a patient with high myopia
- Occurs in a patient with diabetes
- Is accompanied by pain, redness or marked light sensitivity
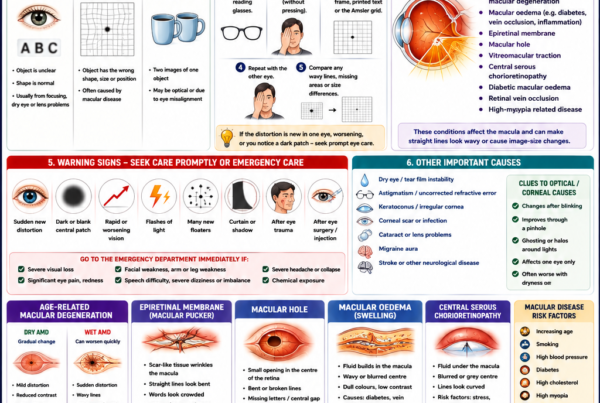
New central distortion may be the first symptom of fluid or bleeding in the macula, including wet age-related macular degeneration. Wet AMD can cause faster visual deterioration than dry AMD and benefits from early diagnosis and treatment.
Seek Emergency Care Immediately For
- A dark curtain or shadow
- Sudden loss of part of the visual field
- Severe or profound visual loss
- Distortion with facial weakness or limb weakness
- Distortion with speech difficulty
- Severe dizziness or loss of balance
- A sudden severe headache
- Significant eye trauma
- Chemical exposure
- Severe eye pain and redness
- Rapidly worsening vision after eye surgery or an injection
These symptoms may indicate retinal detachment, stroke, acute glaucoma, infection or another time-sensitive condition.
Age-Related Macular Degeneration
Age-related macular degeneration, or AMD, damages the macula.
It is broadly divided into:
- Dry AMD
- Wet AMD
Dry AMD
Dry AMD occurs when macular tissues gradually become thinner and accumulate age-related deposits.
It may cause:
- Gradual central blur
- Reduced contrast
- Difficulty seeing in dim light
- Slower adaptation between light and darkness
- Faded colours
- Mild or progressive distortion
- A central missing area in advanced disease
Early AMD may cause no noticeable symptoms.
Wet AMD
Wet AMD occurs when abnormal blood vessels grow beneath or within the retina.
These vessels may:
- Leak fluid
- Bleed
- Lift or distort the macula
- Form scar tissue
Symptoms may include:
- Sudden or rapidly worsening central distortion
- Straight lines appearing wavy
- A grey or dark central patch
- Reduced reading vision
- Faces appearing distorted
- A rapid reduction in central vision
Wet AMD is less common than dry AMD but generally causes faster visual loss. Treatment commonly involves injections that suppress abnormal blood-vessel activity.
Can AMD Cause Complete Blindness?
AMD primarily affects central vision.
Peripheral vision generally remains available, so AMD alone does not usually cause total black blindness.
However, severe central loss may substantially affect:
- Reading
- Driving
- Face recognition
- Cooking
- Medication management
- Independent living
Macular Oedema
Macular oedema means that fluid has accumulated within the macula.
This causes the retinal layers to swell and become disorganised.
Symptoms may include:
- Wavy central vision
- Blurred central vision
- Objects appearing different sizes between the eyes
- Dull or faded colours
- Reduced contrast
- Difficulty reading
- A central grey patch
Common causes include:
- Diabetic retinopathy
- Retinal vein occlusion
- Uveitis
- Inflammation after cataract surgery
- Other retinal vascular disease
- Selected medication effects
OCT is commonly used to identify and measure macular swelling. Treatment may include injections, anti-inflammatory medication, laser or surgery depending on the cause.
Diabetic Macular Oedema
Diabetes damages small retinal blood vessels.
When these vessels leak fluid into the macula, the condition is called diabetic macular oedema.
It may cause:
- Central blur
- Distorted text
- Wavy lines
- Reduced contrast
- Dull colours
- Difficulty recognising faces
Diabetic retinopathy may have no symptoms before advanced disease develops. Regular dilated examinations are therefore important even when vision appears normal.
Can Blood-Sugar Changes Cause Distortion?
Rapid blood-sugar changes can temporarily alter the focusing power of the natural lens and cause blur.
They do not usually cause fixed wavy lines or a focal area of central distortion.
A patient with diabetes and new metamorphopsia requires retinal assessment rather than assuming the symptom is caused only by fluctuating glucose.
Retinal Vein Occlusion
A retinal vein occlusion occurs when a vein draining blood from the retina becomes blocked.
This may cause:
- Retinal bleeding
- Macular oedema
- Sudden blur
- Distortion
- Reduced colour and contrast
- A central blind spot
Treatment may include intravitreal injections and monitoring for abnormal new blood vessels.
Epiretinal Membrane
An epiretinal membrane, sometimes called a macular pucker, is a thin layer of scar-like tissue on the surface of the macula.
As it contracts, it may wrinkle or pull the retinal surface.
Symptoms may include:
- Straight lines appearing bent
- Words appearing crowded
- Letters missing from sentences
- Objects appearing larger or smaller
- Central blur
- Difficulty reading
- Difficulty judging fine detail
Epiretinal membranes usually affect one eye and often progress slowly. Many mild cases require only monitoring. Surgery may be considered when distortion significantly interferes with daily activities.
Does an Epiretinal Membrane Always Need Surgery?
No.
Observation may be appropriate when:
- Distortion is mild
- Visual acuity remains useful
- Daily activities are not significantly affected
- OCT findings are stable
- The patient is comfortable monitoring the condition
Vitrectomy with membrane peeling may be considered when:
- Reading is significantly impaired
- Distortion is troublesome
- Image-size difference interferes with binocular vision
- Daily function is affected
- Symptoms are progressing
The decision is based on the patient’s functional difficulty rather than the OCT appearance alone.
Will Surgery Make Vision Completely Normal?
Not always.
Membrane surgery commonly reduces distortion and improves clarity, but:
- Improvement may be gradual
- Some distortion may remain
- Longstanding retinal displacement may not reverse completely
- Final vision depends on underlying macular health
- Cataract may progress after vitrectomy
The aim is usually meaningful functional improvement rather than a guarantee of perfectly undistorted vision.
Macular Hole
A macular hole is a small opening in the centre of the retina.
It commonly develops when the vitreous gel pulls on the macula.
Symptoms may include:
- Central blur
- Wavy or bent lines
- A missing piece in the centre of a line
- Difficulty reading small print
- A central dark or blank spot
- Difficulty recognising facial details
The eye is usually painless.
Macular holes commonly require vitrectomy surgery. Earlier treatment may provide a better opportunity for anatomical closure and visual improvement.
Is a Macular Hole the Same as AMD?
No.
Both may cause:
- Central blur
- Distortion
- A central missing patch
However:
- A macular hole is a physical opening in the central retina.
- AMD is a degenerative disease involving macular tissues and, in wet AMD, abnormal blood vessels.
OCT usually distinguishes the conditions clearly.
Vitreomacular Traction
Vitreomacular traction occurs when the vitreous partially separates from the retina but remains abnormally attached to the macula.
The attachment pulls on the macular surface.
Possible symptoms include:
- Central distortion
- Wavy lines
- Blur
- Reduced reading vision
- A central blind spot
- Image-size change
Mild cases may release spontaneously.
Persistent or significant traction may lead to:
- Macular swelling
- Macular hole
- Structural retinal damage
Management may include observation, selected injections or vitrectomy depending on the anatomy and symptoms.
Central Serous Chorioretinopathy
Central serous chorioretinopathy occurs when fluid accumulates underneath the central retina.
Patients may notice:
- A blurred or grey central area
- Straight lines appearing curved
- Objects appearing smaller
- Reduced contrast
- Colours appearing dull
- A circular central shadow
It commonly affects one eye.
Risk associations may include:
- Corticosteroid exposure
- Psychological or physiological stress
- Sleep disturbance
- Pregnancy
- Certain systemic conditions
Many first episodes improve spontaneously, but persistent or recurrent fluid may require treatment.
Patients should disclose all forms of steroid exposure, including:
- Tablets
- Inhalers
- Nasal sprays
- Skin creams
- Joint injections
- Eye drops
Steroids should not be stopped abruptly without consulting the prescribing doctor.
High Myopia and Myopic Macular Disease
Highly myopic eyes are longer and may develop degenerative changes at the macula.
Possible causes of distortion include:
- Myopic macular degeneration
- Myopic choroidal neovascularisation
- Myopic traction maculopathy
- Macular hole
- Retinal splitting
- Macular haemorrhage
New central distortion or a dark patch in a highly myopic eye requires prompt retinal assessment.
Previous LASIK, PRK, SMILE or ICL surgery corrects the focusing error but does not shorten the eyeball or remove the retinal risks associated with high myopia.
Macular Haemorrhage
Bleeding beneath or within the macula may cause:
- Sudden central distortion
- A dark central patch
- Reduced vision
- A red or brown area
- Straight lines appearing broken
- Sudden inability to recognise faces
Possible causes include:
- Wet AMD
- Myopic choroidal neovascularisation
- Retinal macroaneurysm
- Trauma
- Retinal vascular disease
Urgent OCT and retinal examination are required.
Retinal Detachment
Retinal detachment occurs when the retina separates from the back wall of the eye.
Distortion is not usually the main early symptom, but it may occur when:
- The detachment reaches the macula
- Subretinal fluid alters central retinal position
- Part of the visual field becomes displaced
- Central vision becomes blurred or missing
Typical warning symptoms include:
- Flashes of light
- Many new floaters
- A curtain or shadow
- Missing peripheral vision
- Sudden blur
Retinal detachment requires emergency treatment to reduce the risk of permanent visual loss.
Distortion After Retinal-Detachment Surgery
Some patients experience persistent visual distortion after successful retinal reattachment.
Possible reasons include:
- Macular involvement before surgery
- Residual retinal damage
- Epiretinal membrane
- Macular oedema
- Retinal folds
- Displacement of the reattached retina
- Image-size or positional differences between the eyes
The retina may be anatomically attached while central visual quality remains imperfect.
OCT and retinal imaging help identify whether further treatment is possible.
Macular Degeneration in Younger Patients
Macular distortion is not limited to older adults.
Possible causes in younger patients include:
- Central serous chorioretinopathy
- Macular dystrophy
- Inflammation
- Infection
- High-myopia-related disease
- Vitreomacular traction
- Macular hole
- Trauma
- Medication toxicity
- Inherited retinal disease
Age alone should not be used to dismiss new metamorphopsia.
Uveitis
Uveitis is inflammation inside the eye.
It may cause distortion when inflammation produces:
- Macular oedema
- Epiretinal membrane
- Choroidal inflammation
- Retinal scarring
- Abnormal blood vessels
Other symptoms may include:
- Eye pain
- Redness
- Photophobia
- Floaters
- Blurred vision
Some posterior forms of uveitis cause little pain or external redness.
Untreated uveitis may cause permanent visual loss.
Corneal Causes of Distorted Vision
Not all visual distortion comes from the retina.
The cornea may produce irregular or stretched images when its surface is uneven.
Possible causes include:
- Dry eye
- Astigmatism
- Keratoconus
- Corneal scarring
- Contact-lens warpage
- Corneal swelling
- Irregular healing after surgery
- Corneal dystrophy
Corneal distortion may produce:
- Ghost images
- Streaking around lights
- Multiple outlines
- Smearing
- Monocular double vision
- Starbursts
Dry Eye
Dry eye destabilises the tear film.
It commonly causes:
- Fluctuating blur
- Ghosting
- Smearing around text
- Vision that temporarily improves after blinking
- Symptoms that worsen during screen use
- Burning or grittiness
Dry eye does not usually cause a fixed bent line in exactly the same location.
A persistent focal distortion should prompt macular assessment even when dry eye is also present.
Astigmatism
Astigmatism causes light to focus unevenly.
Patients may experience:
- Stretched letters
- Shadowed images
- Blur in one direction
- Halos
- Monocular ghosting
- Difficulty with fine detail
Distortion caused by regular astigmatism generally improves with an accurate spectacle or contact-lens prescription.
Keratoconus
Keratoconus causes corneal thinning and progressive irregular steepening.
Possible symptoms include:
- Increasing astigmatism
- Frequent spectacle changes
- Distorted or multiple images
- Glare
- Halos
- Poor night vision
- Reduced vision not fully corrected by spectacles
Corneal topography or tomography is required to assess corneal shape.
Treatment may include:
- Spectacles
- Special contact lenses
- Corneal cross-linking
- Intracorneal ring segments
- Corneal transplantation in advanced disease
Corneal Scarring
A central or irregular corneal scar may bend and scatter light.
Possible causes include:
- Previous infection
- Trauma
- Herpes keratitis
- Chemical injury
- Previous surgery
Symptoms may include:
- Distortion
- Glare
- Ghosting
- Reduced contrast
- Light sensitivity
Distortion After LASIK, PRK or SMILE
Possible causes include:
- Dry eye
- Irregular astigmatism
- Decentred optical treatment
- Corneal ectasia
- Higher-order optical aberrations
- Epithelial irregularity
- Retinal disease unrelated to the procedure
Corneal topography or tomography helps identify shape-related causes.
A patient with a history of high myopia may still develop retinal or macular disease after refractive surgery.
Can Cataract Cause Distortion?
Cataract more commonly causes:
- Haze
- Glare
- Halos
- Faded colours
- Monocular double vision
- Progressive blur
It does not usually cause a fixed area where a straight line appears wavy.
When a patient with cataract reports new metamorphopsia, the macula should be examined rather than attributing all symptoms to the lens.
Neurological Causes of Distorted Vision
Distorted vision occasionally originates from the brain rather than the eye.
Possible causes include:
- Migraine aura
- Stroke
- Seizure
- Brainstem or vestibular disease
- Occipital-lobe disease
- Visual-perception disorders
- Medication or toxic effects
Neurological distortion may affect:
- Both visual fields
- One side of both visual fields
- The apparent orientation of the environment
- Faces or body parts
- Spatial judgement
Migraine Aura
Migraine aura may cause:
- Shimmering distortion
- Zigzag lines
- A spreading blind spot
- Geometric patterns
- Objects appearing fragmented
- Temporary visual warping
Typical aura usually:
- Develops gradually
- Changes over several minutes
- Affects the visual field of both eyes
- Resolves within approximately one hour
- May occur with or without headache
A first episode, unusual pattern or persistent deficit requires medical assessment.
Stroke
Stroke may produce:
- Sudden loss of one side of the visual field
- Distorted spatial awareness
- Difficulty recognising objects
- Difficulty reading
- Double vision
- A tilted or displaced visual environment
Seek emergency care when sudden distortion is associated with:
- Facial drooping
- Arm or leg weakness
- Numbness
- Speech difficulty
- Confusion
- Severe imbalance
- A sudden severe headache
Can the Entire World Look Tilted?
Rare neurological or vestibular disorders may make the environment appear:
- Tilted
- Rotated
- Upside down
- Reversed
This is different from a single bent line caused by macular disease.
A sudden large-scale change in visual orientation requires emergency neurological assessment, particularly when associated with dizziness, imbalance or other neurological symptoms.
Facial Distortion
Patients may notice that:
- One side of a face looks enlarged
- Facial features appear displaced
- The nose or eye appears missing
- Faces appear unusually compressed
This may result from:
- Macular distortion
- Image-size difference
- Retinal misregistration
- Less commonly, a brain-based face-processing disorder
Testing each eye separately helps determine whether the symptom originates primarily from one eye.
Distortion in Children
Children may not use the word “distorted.”
They may say:
- “The letters move.”
- “The lines bend.”
- “One side looks bigger.”
- “The page looks funny.”
- “The face looks crooked.”
Possible causes include:
- Refractive error
- Keratoconus
- Macular disease
- Retinal dystrophy
- Inflammation
- Migraine
- Neurological disease
- Functional visual symptoms
New persistent distortion in a child requires examination.
How Is Distorted Vision Assessed?
Visual Acuity
Each eye is tested separately.
Visual acuity may be:
- Normal despite distortion
- Mildly reduced
- Significantly reduced when the central macula is involved
The eye-chart result does not fully measure visual quality.
Refraction and Pinhole Testing
Refraction determines whether spectacles improve clarity.
Pinhole improvement may suggest:
- Refractive error
- Tear-film irregularity
- Corneal optical problems
Persistent wavy lines despite pinhole correction increase concern for retinal or macular disease.
Amsler Grid
The Amsler grid is a square grid of horizontal and vertical lines with a central fixation point.
It may reveal:
- Wavy lines
- Missing areas
- Blurred patches
- Uneven squares
- Central distortion
Changes in the macula may cause lines on the grid to appear wavy or disappear.
How to Use an Amsler Grid
- Wear the normal reading glasses.
- Hold the grid at the usual reading distance.
- Use good, even lighting.
- Cover one eye without pressing on it.
- Look directly at the centre dot.
- Keep looking at the dot.
- Notice whether any lines look wavy, missing, blurred or unequal.
- Repeat with the other eye.
- Mark the abnormal area if instructed by the eye doctor.
What Should I Do If the Amsler Grid Changes?
Contact the eye clinic promptly if:
- Lines suddenly become wavy
- A new patch appears
- Part of the grid disappears
- The centre becomes blurred
- The abnormal area enlarges
- One eye differs noticeably from the other
Do not wait for the next routine appointment when the change is new.
Can a Normal Amsler Grid Exclude Macular Disease?
No.
The Amsler grid may miss:
- Small defects
- Early disease
- Changes outside the central tested area
- Abnormalities the brain fills in
- Subtle image-size differences
It is a useful monitoring tool but does not replace:
- Visual-acuity testing
- Dilated examination
- OCT
- Retinal imaging
Slit-Lamp Examination
The slit lamp assesses:
- Tear film
- Cornea
- Anterior chamber
- Iris
- Lens
This helps distinguish optical distortion from retinal disease.
Dilated Retinal Examination
Dilation allows examination of:
- Macula
- Retinal blood vessels
- Peripheral retina
- Optic nerve
- Vitreous
The clinician looks for:
- AMD
- Bleeding
- Retinal swelling
- Epiretinal membrane
- Macular hole
- Diabetic changes
- Retinal detachment
- Inflammation
Optical Coherence Tomography
OCT produces high-resolution cross-sectional images of the retina.
It is one of the most important tests for distorted central vision.
OCT may identify:
- Macular fluid
- Epiretinal membrane
- Macular hole
- Vitreomacular traction
- Retinal splitting
- Central serous fluid
- AMD-related changes
- Diabetic macular oedema
OCT Angiography
OCT angiography images retinal and choroidal blood flow without injected dye.
It may help detect:
- Abnormal macular blood vessels
- Wet AMD
- Myopic choroidal neovascularisation
- Retinal vascular abnormalities
It complements rather than replaces structural OCT and clinical examination.
Fluorescein Angiography
Fluorescein dye is injected into a vein, and photographs are taken as it passes through retinal vessels.
The test may identify:
- Leakage
- Abnormal new blood vessels
- Blocked vessels
- Macular oedema
- Inflammatory lesions
It may be used when the cause or activity of retinal leakage is uncertain.
Fundus Autofluorescence
Fundus autofluorescence assesses patterns related to retinal pigment epithelium health.
It may help evaluate:
- Dry AMD
- Geographic atrophy
- Macular dystrophy
- Inflammatory retinal disease
- Selected toxic retinal conditions
Corneal Topography or Tomography
These tests map corneal shape.
They may identify:
- Keratoconus
- Corneal warpage
- Post-LASIK irregularity
- Irregular astigmatism
- Corneal ectasia
Visual-Field Testing
Visual-field testing may be needed when the patient reports:
- A missing area
- Loss of one side of vision
- Neurological symptoms
- Optic-nerve disease
- A fixed central or peripheral defect
Neurological Imaging
CT or MRI may be required when distortion is associated with:
- Neurological deficits
- A visual-field defect affecting both eyes
- Severe headache
- Seizure
- Abnormal eye movements
- A tilted visual environment
- Unexplained persistent symptoms with a normal ocular examination
Can Distorted Vision Be Diagnosed Online?
No.
A description cannot reliably distinguish between:
- Wet AMD
- Macular oedema
- Epiretinal membrane
- Macular hole
- Central serous disease
- Corneal irregularity
- Migraine
- Stroke
A photograph of the external eye may appear normal in serious macular disease.
The required assessment often includes:
- Testing each eye separately
- Dilated examination
- OCT
- Retinal imaging
- Corneal imaging when indicated
How Is Distorted Vision Treated?
Treatment depends on the cause.
Wet AMD or Choroidal Neovascularisation
Treatment commonly involves intravitreal anti-VEGF injections.
The goals are to:
- Reduce leakage
- Control abnormal blood vessels
- Reduce retinal swelling
- Limit scarring
- Preserve or improve central vision
Repeated treatment and monitoring are often required.
Macular Oedema
Treatment may include:
- Anti-VEGF injections
- Steroid injections or implants
- Anti-inflammatory eye drops
- Retinal laser
- Vitrectomy
- Treatment of diabetes
- Treatment of retinal vascular disease or uveitis
Epiretinal Membrane
Mild cases may be monitored.
Troublesome cases may be treated with:
- Vitrectomy
- Membrane peeling
Surgery is considered mainly when symptoms interfere meaningfully with daily life.
Macular Hole
Treatment commonly involves:
- Vitrectomy
- Removal of tractional tissue
- A gas bubble
- Postoperative positioning in selected cases
Air travel must be avoided while an intraocular gas bubble remains.
Central Serous Chorioretinopathy
Management may include:
- Observation
- Reviewing steroid exposure
- Treating sleep or systemic contributors
- Photodynamic therapy
- Selected laser treatment
- Other retinal treatment for persistent or recurrent disease
Corneal Causes
Treatment may include:
- Artificial tears
- Treatment of meibomian gland dysfunction
- Updated spectacles
- Special contact lenses
- Corneal cross-linking
- Treatment of infection or scarring
- Corneal surgery in advanced disease
Migraine
Management may include:
- Identifying triggers
- Acute migraine medication
- Preventive medication
- Neurological assessment when atypical
- Lifestyle and sleep modification
Migraine treatment should not be started as the only explanation for a first episode of new monocular distortion before retinal causes are excluded.
Will Distorted Vision Return to Normal?
The prognosis depends on:
- Cause
- Duration
- Amount of structural retinal change
- Whether bleeding or scar tissue is present
- Timing of treatment
- Baseline macular health
- Whether both eyes are affected
Possible outcomes include:
- Complete resolution
- Partial improvement
- Stable mild distortion
- Persistent distortion despite improved visual acuity
- Progressive central visual loss
Treatment may be successful even when some distortion remains, particularly if it prevents further deterioration.
Why Can Distortion Persist After the OCT Improves?
Structural recovery and visual perception are not always identical.
Distortion may remain because:
- Photoreceptors have been permanently displaced
- Retinal organisation remains altered
- Scar tissue is present
- The brain has adapted to an abnormal image
- Image-size differences remain
- Longstanding disease caused irreversible cellular loss
Can Glasses Correct Metamorphopsia?
Ordinary spectacle lenses can improve refractive blur.
They generally cannot straighten lines distorted by macular disease.
Prism, image-size modification or specialist low-vision strategies may help selected patients with:
- Aniseikonia
- Retinal misregistration
- Binocular difficulty
Can Vitamins Cure Distorted Vision?
No general vitamin cures metamorphopsia.
AREDS2 supplements may reduce the risk of progression in selected patients with intermediate AMD or late AMD in one eye. They do not treat wet AMD, remove an epiretinal membrane or close a macular hole.
High-dose supplements should not be started without confirming:
- The diagnosis
- The AMD stage
- Smoking history
- Other medications
- Medical suitability
Can Eye Exercises Straighten Wavy Lines?
No.
Eye exercises do not reposition swollen or displaced macular tissue.
They may help selected binocular-vision problems but do not treat:
- AMD
- Macular oedema
- Epiretinal membrane
- Macular hole
- Retinal detachment
Can Distortion Be Caused by Stress?
Stress may contribute to:
- Migraine
- Central serous chorioretinopathy
- Increased awareness of symptoms
- Sleep disruption
However, persistent one-eye metamorphopsia should not be attributed to stress without retinal examination.
Can Screen Use Cause Distorted Vision?
Screen use may worsen:
- Dry eye
- Tear-film ghosting
- Eye strain
- Awareness of existing macular distortion
It does not usually cause an epiretinal membrane, wet AMD or macular hole.
Bright screens and straight text lines may simply make an existing distortion easier to notice.
Frequently Asked Questions
Are wavy lines always caused by macular degeneration?
No.
Other causes include:
- Macular oedema
- Epiretinal membrane
- Macular hole
- Vitreomacular traction
- Central serous disease
- High-myopia-related disease
- Corneal irregularity
Are wavy lines an emergency?
New or sudden wavy lines require prompt assessment, particularly in one eye or in a patient with AMD.
Can dry eye make lines appear bent?
Dry eye can produce fluctuating smearing or ghosting.
A fixed focal bend in the same location is more suggestive of retinal or macular disease.
Can cataract make straight lines wavy?
Cataract usually causes haze, glare or multiple images rather than true fixed metamorphopsia.
Can astigmatism cause distortion?
Yes.
Astigmatism may stretch or shadow images, but it generally improves with refraction or pinhole testing.
Why do faces look strange?
Macular distortion may displace facial features or make one area appear enlarged, compressed or missing.
Why do words look crowded?
An epiretinal membrane or other macular disorder may compress the retinal image and make letters appear crowded.
Why does one eye see objects smaller?
Possible causes include:
- Macular swelling
- Central serous disease
- Retinal displacement
- Refractive image-size difference
- Other macular disease
Does distortion mean I am going blind?
Not necessarily.
Some causes are mild, stable or treatable.
Prompt diagnosis is important because certain conditions can cause permanent central visual loss.
Can an epiretinal membrane cause total blindness?
No.
It affects central visual quality but does not usually eliminate all peripheral vision.
Does an epiretinal membrane always worsen?
No.
Some remain stable for years.
Can a macular hole close by itself?
A small early hole may occasionally resolve, but many full-thickness holes require surgery.
Does wet AMD always affect both eyes?
No.
It may begin in one eye, although the fellow eye remains at increased risk.
Why did I not notice the distortion earlier?
The other eye may have compensated.
Testing each eye separately often reveals symptoms that binocular vision had concealed.
Can retinal injections improve distortion?
They may reduce distortion when it is caused by active fluid or abnormal blood vessels.
Some symptoms may remain if permanent retinal damage or scarring has occurred.
Can distortion recur after treatment?
Yes.
Recurrence may occur with:
- Wet AMD
- Macular oedema
- Central serous disease
- Inflammation
- Epiretinal membrane
- Recurrent abnormal blood-vessel activity
Why is the Amsler grid normal even though something feels wrong?
Small, subtle or non-central abnormalities may not be detected by the grid.
Formal examination and OCT may still reveal disease.
Should I test the Amsler grid every day?
The advised frequency depends on the diagnosis.
Many patients at risk of wet AMD are advised to monitor regularly, but excessive repeated testing can increase anxiety and make comparison difficult.
Follow the schedule recommended by the eye doctor.
Can I drive with distorted vision?
Do not drive when distortion affects:
- Road signs
- Lane position
- Pedestrian detection
- Depth judgement
- Recognition of traffic lights
- Central visual clarity
Visual acuity and field requirements still apply.
Can low-vision aids help?
Yes.
Helpful measures may include:
- Magnifiers
- Electronic enlargement
- Increased contrast
- Better lighting
- Text-to-speech software
- Eccentric-viewing training
- Occupational-therapy support
A Practical Urgency Guide
Emergency Assessment Now
- Curtain or shadow
- Sudden visual-field loss
- Severe sudden visual reduction
- Distortion with stroke symptoms
- Significant eye trauma
- Chemical injury
- Severe pain and redness
- Worsening vision after surgery or injection
Prompt or Same-Day Eye Assessment
- Sudden new wavy lines
- New central distortion in one eye
- New dark or blank central patch
- Rapidly worsening reading vision
- New distortion in a patient with AMD
- New distortion in a highly myopic eye
- New distortion in a patient with diabetes
- Distortion with flashes or new floaters
Routine Assessment May Be Appropriate
- Longstanding stable epiretinal-membrane distortion
- Stable corneal ghosting
- Known refractive distortion corrected by glasses
- Previously assessed stable symptoms
Any sudden change moves the condition into a more urgent category.
A Practical Clinical Approach
Step 1: Clarify the Symptom
- Wavy
- Bent
- Stretched
- Shrunken
- Tilted
- Missing
- Displaced
- Double
Step 2: Test Each Eye Separately
Determine whether:
- One eye is affected
- Both eyes differ
- The same change is present binocularly
Step 3: Determine the Timing
- Sudden
- Gradual
- Constant
- Intermittent
- Progressive
- Recurrent
Step 4: Look for Warning Signs
- Central dark patch
- Flashes
- Floaters
- Curtain
- Pain
- Redness
- Neurological symptoms
- Trauma
- Recent surgery
Step 5: Examine the Optical Media
Assess:
- Tear film
- Refraction
- Cornea
- Lens
Step 6: Examine the Macula
Use:
- Dilated examination
- OCT
- Retinal imaging
- Angiography when indicated
Step 7: Identify the Mechanism
- Fluid
- Bleeding
- Traction
- Wrinkling
- Hole
- Degeneration
- Corneal irregularity
- Neurological dysfunction
Step 8: Treat the Cause
The correct treatment may involve:
- Lubrication
- Spectacles or contact lenses
- Intravitreal injections
- Anti-inflammatory medication
- Retinal laser
- Photodynamic therapy
- Vitrectomy
- Neurological treatment
Common Myths About Distorted Vision
“Wavy lines just mean I need new glasses.”
False.
Macular disease is a common cause and may not improve with spectacles.
“If there is no pain, the retina must be healthy.”
False.
Most macular conditions are painless.
“A normal eye-chart result excludes macular disease.”
False.
Distortion may be significant even when high-contrast acuity remains relatively good.
“The good eye means I can wait.”
False.
The better eye may be masking important disease in the other eye.
“All distortion in an older person is AMD.”
False.
Epiretinal membrane, macular hole, diabetic disease and other retinal conditions may cause similar symptoms.
“Amsler-grid monitoring replaces eye examinations.”
False.
The grid may miss early or subtle disease.
“AREDS2 vitamins treat wet AMD.”
False.
Wet AMD generally requires active retinal assessment and commonly intravitreal treatment.
“Screens damage the macula and create wavy lines.”
False.
Screens may reveal or worsen awareness of symptoms but do not usually cause structural macular disease.
“Once distortion develops, nothing can be done.”
False.
Several causes are treatable, and early treatment may preserve or improve vision.
The Bottom Line
Distorted vision means that objects appear to have the wrong shape, size, position or orientation.
Patients may notice:
- Wavy lines
- Bent doorframes
- Crowded letters
- Stretched faces
- Smaller or larger images
- A missing central area
Common causes include:
- Age-related macular degeneration
- Macular oedema
- Epiretinal membrane
- Macular hole
- Vitreomacular traction
- Central serous chorioretinopathy
- Diabetic retinopathy
- Retinal vein occlusion
- High-myopia-related macular disease
- Corneal irregularity
The first practical steps are:
- Test each eye separately.
- Determine whether the distortion is new.
- Look for a dark patch, flashes, floaters or a curtain.
- Arrange prompt eye assessment for sudden central distortion.
- Seek emergency care for field loss, severe visual reduction or neurological symptoms.
Assessment commonly includes:
- Visual acuity and refraction
- Slit-lamp examination
- Dilated retinal examination
- OCT
- Retinal photography
- Angiography
- Corneal imaging when indicated
New distorted vision should not be dismissed as tired eyes or an outdated spectacle prescription. Straight lines becoming wavy may be the first warning that the macula is swollen, pulled, bleeding or otherwise structurally altered—and early assessment may preserve central vision.
References
- National Eye Institute. Age-Related Macular Degeneration.
- National Eye Institute. Macular Edema. Updated August 2025.
- National Eye Institute. Macular Pucker. Updated December 2024.
- National Eye Institute. Macular Hole. Updated December 2024.
- National Eye Institute. Diabetic Retinopathy. Updated September 2025.
- National Eye Institute. Retinal Detachment. Updated November 2025.
- National Eye Institute. Dry Eye. Updated August 2025.
- National Eye Institute. Corneal Conditions. Updated August 2025.
- National Eye Institute. Uveitis. Updated December 2024.
- Singapore HealthHub. Common Eye Problems and Their Symptoms.
- Moorfields Eye Hospital. Epiretinal Membrane.
- Moorfields Eye Hospital. Age-Related Macular Degeneration.
- NHS. Macular Hole.
- American Academy of Ophthalmology. Vitreomacular Traction Syndrome.
- Midena E, Vujosevic S. Metamorphopsia: An Overlooked Visual Symptom. Ophthalmic Research. 2015.