Author: Dr Val Phua
Estimated reading time: 14–16 minutes
What Is Double Vision?
Double vision means seeing two images of a single object.
The medical term is diplopia.
The images may appear:
- Side by side
- One above the other
- Diagonally separated
- Slightly overlapping
- Tilted or rotated
- Like a clear image with a faint ghost beside it
Double vision may be:
- Constant
- Intermittent
- Worse when tired
- Present only at distance
- Present only during reading
- Worse in a particular direction of gaze
- Present only when both eyes are open
- Present even when one eye is covered
The first and most important step is to determine whether the double vision is monocular or binocular. These two patterns usually arise from very different causes.
Is Double Vision the Same as Blurred Vision?
No.
Blurred Vision
Blurred vision means that an object appears unclear, hazy or out of focus.
Double Vision
Double vision means that two separate or overlapping images are perceived.
Patients may find it difficult to distinguish between:
- Blur
- Ghosting
- Shadowing around letters
- Glare
- True double vision
- Distortion caused by retinal disease
A careful examination is often needed, particularly when the second image is faint rather than clearly separated.
Is Double Vision an Emergency?
New double vision should be assessed promptly.
Seek emergency medical or ophthalmic care when double vision:
- Begins suddenly
- Occurs with severe headache
- Occurs with a newly drooping eyelid
- Occurs with unequal pupils
- Follows a head or eye injury
- Occurs with weakness, numbness or facial drooping
- Occurs with speech difficulty or confusion
- Occurs with severe dizziness or imbalance
- Is associated with loss of vision
- Is associated with eye pain, swelling or fever
- Occurs with a bulging eye
- Is associated with difficulty swallowing or breathing
Sudden diplopia is included among symptoms that may require emergency assessment because it can result from stroke, aneurysm, cranial-nerve palsy, orbital disease or other neurological disorders.
What Should I Do When Double Vision Starts?
- Stop driving immediately.
- Cover one eye and then the other without pressing on them.
- Check whether the second image disappears when either eye is covered.
- Note the exact time the symptom began.
- Check for headache, eyelid drooping, unequal pupils or neurological symptoms.
- Arrange prompt eye assessment.
- Seek emergency care for sudden onset or any associated neurological warning sign.
Covering one eye may temporarily remove binocular diplopia and make movement safer, but it does not treat the underlying cause.
Monocular Versus Binocular Double Vision
What Is Monocular Double Vision?
Monocular diplopia remains present when the unaffected eye is covered and the symptomatic eye remains open.
For example:
- Cover the left eye.
- The right eye still sees two images.
- This suggests right monocular diplopia.
Monocular diplopia usually results from an optical problem within the eye rather than misalignment between the two eyes.
Common causes include:
- Dry eye
- Uncorrected astigmatism
- Irregular corneal shape
- Keratoconus
- Cataract
- Lens displacement
- Problems with an intraocular lens
- Macular disease
- Less commonly, neurological or functional visual phenomena
Monocular double vision often improves with blinking or looking through a pinhole when refractive or tear-film abnormalities are responsible.
What Is Binocular Double Vision?
Binocular diplopia occurs when the two eyes are not pointing accurately at the same object.
It disappears when either eye is covered.
For example:
- Both eyes open: two images.
- Right eye covered: one image.
- Left eye covered: one image.
This indicates that each eye can form an image, but the brain cannot combine them because the images fall on non-corresponding retinal locations.
Possible causes include:
- Strabismus
- A cranial-nerve palsy
- Thyroid eye disease
- Myasthenia gravis
- Orbital disease
- A brainstem or cerebellar disorder
- Stroke
- Head injury
- Decompensation of a longstanding eye-muscle imbalance
Binocular diplopia may reflect an eye-movement disorder, nerve disorder, muscle disorder, orbital restriction or central neurological disease.
How Can I Test Whether the Double Vision Is Monocular or Binocular?
While looking at a single object:
- Cover the right eye.
- Note whether one or two images remain.
- Uncover it.
- Cover the left eye.
- Note what happens again.
The Double Vision Disappears When Either Eye Is Covered
This suggests binocular diplopia.
The Double Vision Persists in One Particular Eye
This suggests monocular diplopia in that eye.
The Double Vision Persists with Either Eye Tested Separately
This may represent:
- Optical problems in both eyes
- Multiple ghost images
- Visual-processing symptoms
- An imprecise description of blur or distortion
This simple test is useful, but it should not delay urgent assessment.
Monocular Double Vision: Common Causes
Dry Eye and Tear-Film Instability
The tear film forms the first optical surface of the eye.
When it becomes irregular, a person may see:
- A faint second image
- Shadowing around letters
- Fluctuating blur
- Starbursts
- Glare
- Multiple images around lights
Dry-eye ghosting often:
- Changes after blinking
- Worsens during prolonged screen use
- Is worse in air conditioning
- Temporarily improves with lubrication
Persistent symptoms require examination because dry eye may coexist with cataract, corneal irregularity or retinal disease.
Astigmatism and Refractive Error
Astigmatism occurs when the cornea or lens focuses light differently in different meridians.
It may cause:
- Shadowed letters
- Horizontal or vertical ghosting
- Blur at distance and near
- Headaches
- Eye strain
- Halos
Monocular diplopia caused by refractive error may improve with:
- Spectacles
- Contact lenses
- Pinhole testing
- Refraction
Refractive errors can produce double or hazy vision as well as ordinary blur.
Keratoconus and Irregular Corneal Shape
Keratoconus causes progressive corneal thinning and distortion.
Possible symptoms include:
- Ghosting
- Monocular double vision
- Distorted lights
- Increasing astigmatism
- Frequent spectacle changes
- Glare
- Reduced night vision
Spectacles may become insufficient when the corneal surface becomes significantly irregular.
Assessment may include:
- Corneal topography
- Corneal tomography
- Pachymetry
- Refraction
- Contact-lens assessment
Keratoconus is a recognised cause of double vision, blur and irregular astigmatism.
Cataract
A cataract is clouding of the natural lens.
It may cause:
- Monocular double vision
- Multiple images
- Glare
- Halos
- Hazy vision
- Reduced contrast
- Poor night vision
- Faded colours
The double image usually remains when the other eye is covered.
Cataract surgery may resolve lens-related monocular diplopia after other causes are excluded.
Lens Displacement
The natural lens can become partially displaced because of:
- Trauma
- Previous eye surgery
- Inherited connective-tissue disorders
- Weakness of the supporting zonules
- Advanced pseudoexfoliation
- Other structural eye disease
Symptoms may include:
- Monocular diplopia
- Fluctuating vision
- A visible lens edge
- Marked refractive change
- Glare
Lens displacement may require observation, spectacle correction or surgery depending on severity.
Double Vision After Cataract Surgery
Possible causes include:
- Residual astigmatism
- Dry eye
- Decentration or tilt of the intraocular lens
- A multifocal-lens optical phenomenon
- Posterior capsule opacification
- Previously controlled strabismus becoming symptomatic
- Cranial-nerve palsy
- Anaesthetic-related muscle injury in older techniques
- Retinal distortion
The first step is to determine whether the postoperative symptom is monocular or binocular.
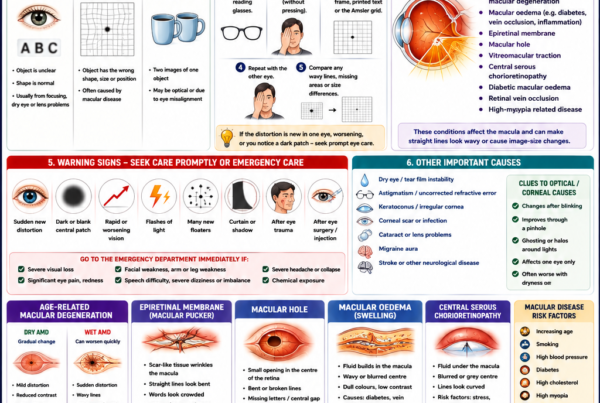
Macular Disease
Macular disease usually causes distortion rather than classic diplopia, but patients may describe:
- A doubled letter
- A displaced central image
- Image-size difference
- A tilted image
- A central ghost
Possible causes include:
- Epiretinal membrane
- Macular oedema
- Macular degeneration
- Macular hole
- Retinal displacement
Macular pathology may create a retinal misregistration problem that can persist even when the eyes appear properly aligned.
Binocular Double Vision: Why the Eyes Become Misaligned
For single binocular vision, the eyes must move together with great precision.
This depends on:
- Six eye muscles in each eye
- Cranial nerves III, IV and VI
- The neuromuscular junction
- Brainstem eye-movement centres
- Cerebellar control
- Vestibular pathways
- Orbital tissues
- The brain’s ability to fuse the two images
Disruption anywhere along this system may produce binocular diplopia.
What Does the Direction of the Double Images Mean?
Horizontal Diplopia
Images appear side by side.
Possible causes include:
- Sixth-nerve palsy
- Esotropia
- Exotropia
- Decompensated horizontal phoria
- Convergence insufficiency
- Thyroid eye disease
- Internuclear ophthalmoplegia
Vertical Diplopia
One image appears above the other.
Possible causes include:
- Fourth-nerve palsy
- Skew deviation
- Thyroid eye disease
- Orbital-floor fracture
- Restricted vertical eye movement
- Decompensated vertical phoria
Torsional Diplopia
One image appears rotated or tilted.
Possible causes include:
- Fourth-nerve palsy
- Skew deviation
- Vestibular or brainstem disease
- Bilateral superior-oblique dysfunction
The direction is helpful, but the same pattern may arise from several conditions.
Does the Gaze Direction Matter?
Yes.
The clinician may ask whether the double vision is worse:
- Looking right
- Looking left
- Looking up
- Looking down
- At distance
- At near
- When lying down
- When tilting the head
A larger separation in one direction may identify the weak, restricted or overacting muscle.
For example:
- Diplopia worse at distance may suggest divergence weakness or sixth-nerve dysfunction.
- Diplopia worse at near may suggest convergence insufficiency.
- Vertical diplopia worse when reading or walking downstairs may suggest fourth-nerve dysfunction.
- Diplopia worse looking upwards may occur with thyroid-related inferior-rectus restriction.
Decompensated Phoria
A phoria is a tendency for the eyes to drift when binocular fusion is interrupted.
Most people can compensate for a small phoria without symptoms.
It may become symptomatic because of:
- Fatigue
- Illness
- Ageing
- Stress
- Reduced vision in one eye
- Cataract
- New spectacles
- Head injury
- Loss of fusion reserves
Symptoms may include:
- Intermittent double vision
- Eye strain
- Headache
- Difficulty maintaining focus
- Symptoms worse late in the day
Treatment may include:
- Correcting refractive error
- Prism
- Orthoptic exercises
- Treating the condition that reduced fusion
- Strabismus surgery in selected cases
Childhood Strabismus Becoming Symptomatic in Adulthood
A childhood squint may have been controlled through:
- Suppression
- An abnormal head position
- Strong fusional reserves
- Previous surgery
- Prism glasses
Double vision may later develop because compensation deteriorates.
Old photographs can help identify:
- A longstanding head tilt
- Childhood eye deviation
- Previous eyelid drooping
- Facial asymmetry
Convergence Insufficiency
Convergence is the inward movement of both eyes when looking at a near object.
In convergence insufficiency, the eyes have difficulty maintaining this inward alignment.
Symptoms may include:
- Double vision during reading
- Words appearing to move
- Near blur
- Eye strain
- Headache
- Difficulty concentrating
- Loss of place while reading
- Closing one eye
It may begin in childhood or appear after concussion or other neurological injury. Treatment may include convergence exercises, prism or other orthoptic management.
Cranial-Nerve Palsies
Three cranial nerves control the eye muscles:
- Third cranial nerve
- Fourth cranial nerve
- Sixth cranial nerve
A palsy may result from:
- Reduced blood supply
- Diabetes
- High blood pressure
- Aneurysm
- Stroke
- Tumour
- Inflammation
- Infection
- Trauma
- Raised intracranial pressure
The pattern of eye movement helps identify the affected nerve.
Third Cranial-Nerve Palsy
The third nerve controls:
- Most eye movements
- Elevation of the upper eyelid
- Pupil constriction
A third-nerve palsy may cause:
- Double vision
- A drooping eyelid
- The eye turning outward and downward
- Difficulty looking up, down or inward
- An enlarged or poorly reacting pupil
A sudden third-nerve palsy may be caused by an intracranial aneurysm and requires urgent neurological imaging.
Modern neuro-ophthalmic guidance advises urgent assessment even when the pupil appears initially spared because clinical pupil findings alone cannot reliably exclude a compressive lesion.
Third-Nerve Palsy Warning Signs
Seek emergency care for:
- Sudden double vision
- New eyelid drooping
- A newly enlarged pupil
- Severe headache
- Eye pain
- Nausea or vomiting
- Loss of consciousness
- Weakness or neurological symptoms
A pupil-involving third-nerve palsy is an ophthalmic and neurosurgical emergency.
Fourth Cranial-Nerve Palsy
The fourth nerve supplies the superior-oblique muscle.
A fourth-nerve palsy may cause:
- Vertical or diagonal diplopia
- Images that appear tilted
- Symptoms worse when looking down
- Difficulty reading
- Difficulty walking downstairs
- A compensatory head tilt
Possible causes include:
- Congenital weakness becoming symptomatic later
- Head trauma
- Microvascular disease
- Brainstem disease
- Compression
- Inflammation
A longstanding head tilt in old photographs may suggest a congenital palsy rather than a recent neurological event.
Sixth Cranial-Nerve Palsy
The sixth nerve supplies the lateral-rectus muscle, which turns the eye outward.
A sixth-nerve palsy commonly causes:
- Horizontal double vision
- The affected eye turning inward
- Symptoms worse at distance
- Symptoms worse when looking towards the affected side
- A compensatory face turn
Possible causes include:
- Diabetes
- High blood pressure
- Raised intracranial pressure
- Stroke
- Tumour
- Trauma
- Inflammation
- Infection
Even when microvascular disease is suspected, the patient requires clinical assessment and follow-up because the sixth nerve has a long intracranial course and may be affected by several neurological conditions.
What Is a Microvascular Cranial-Nerve Palsy?
Small blood vessels supplying a cranial nerve may become impaired, particularly in patients with:
- Diabetes
- Hypertension
- High cholesterol
- Smoking history
- Other vascular risks
The resulting palsy may recover gradually over several weeks or months.
Management may include:
- Controlling vascular risk factors
- Temporary occlusion
- Prism
- Monitoring recovery
- Imaging when the presentation is atypical
The diagnosis should not be made solely because the patient has diabetes or high blood pressure. New cranial-nerve palsies still require a complete assessment.
Stroke and Double Vision
Stroke may cause diplopia by affecting:
- Brainstem eye-movement centres
- Cranial-nerve nuclei
- Cerebellum
- Vestibular pathways
- Higher visual-processing systems
Associated symptoms may include:
- Facial weakness
- Arm or leg weakness
- Numbness
- Slurred speech
- Difficulty swallowing
- Severe dizziness
- Loss of balance
- Abnormal eye movements
- Visual-field loss
- Severe headache
Sudden double vision with neurological symptoms requires emergency stroke assessment, even if the symptoms improve.
Internuclear Ophthalmoplegia
Internuclear ophthalmoplegia, or INO, is caused by damage to a brainstem pathway coordinating horizontal eye movements.
It may cause:
- Horizontal diplopia
- Difficulty moving one eye inward
- Jerking movement of the opposite eye
- Imbalance between the two eyes
Possible causes include:
- Stroke
- Multiple sclerosis
- Other inflammatory or structural brainstem disease
Younger patients may require investigation for demyelinating disease, while acute INO in an older patient may suggest a vascular event.
Skew Deviation
Skew deviation is a vertical misalignment caused by disturbance of vestibular pathways in the brainstem or cerebellum.
It may be associated with:
- Sudden vertical diplopia
- Head tilt
- Eye torsion
- Imbalance
- Nystagmus
- Other neurological symptoms
Because skew deviation may indicate central neurological disease, the overall examination is essential.
Myasthenia Gravis
Myasthenia gravis is an autoimmune disorder affecting communication between nerves and muscles.
Ocular symptoms may include:
- Fluctuating double vision
- Drooping of one or both eyelids
- Symptoms worse with fatigue
- Improvement after rest
- Different patterns at different times
- Normal pupils
The eye findings may not fit neatly into one cranial-nerve pattern.
Generalised symptoms may include:
- Difficulty chewing
- Difficulty swallowing
- Slurred speech
- Neck weakness
- Limb weakness
- Shortness of breath
Breathing or swallowing difficulty is a medical emergency.
Can Myasthenia Affect Only the Eyes?
Yes.
Ocular myasthenia may initially cause only:
- Diplopia
- Ptosis
Some patients later develop more generalised weakness, while others remain limited to ocular symptoms.
Diagnosis may involve:
- Fatigability testing
- Ice-pack testing
- Blood tests for antibodies
- Electrical nerve-muscle testing
- Neurological assessment
- Chest imaging for thymic disease
A negative antibody result does not exclude every case.
Thyroid Eye Disease
Thyroid eye disease causes inflammation and later scarring of muscles and tissues within the orbit.
It may cause:
- Double vision
- Bulging eyes
- Eyelid retraction
- Puffy eyelids
- Pain or pressure
- Dryness and exposure
- Restricted eye movement
- Difficulty closing the eyes
The inferior and medial rectus muscles are commonly affected, leading to vertical or horizontal diplopia.
Severe disease can compress the optic nerve and threaten sight. Warning signs include reduced vision, impaired colour vision and progressive visual-field loss.
Orbital Cellulitis
Orbital cellulitis is a serious infection of tissues behind the eye.
It may cause:
- Double vision
- Fever
- Severe eyelid swelling
- Pain with eye movement
- Restricted eye movement
- A bulging eye
- Reduced vision
- Headache
- General illness
It is an emergency because infection may threaten vision or spread towards the brain.
Orbital Tumours or Inflammation
A mass or inflammatory disorder within the orbit may displace or restrict the eye.
Possible symptoms include:
- Progressive diplopia
- Proptosis
- Pain or pressure
- Eyelid swelling
- Reduced eye movement
- Reduced vision
- Altered colour vision
- A change in the position of the eye
CT or MRI may be required.
Orbital Fracture
A blow to the orbit may fracture the thin walls surrounding the eye.
Double vision may result from:
- Entrapment of an eye muscle
- Soft-tissue swelling
- Cranial-nerve injury
- Mechanical restriction
- Change in orbital volume
Warning signs include:
- Pain on eye movement
- Inability to look upwards
- Nausea or vomiting triggered by eye movement
- Facial numbness
- A sunken eye
- Significant swelling
- Reduced vision
Children can have “white-eye” blowout fractures with minimal bruising but significant muscle entrapment and nausea. These require urgent assessment.
Double Vision After Head Injury
Possible causes include:
- Fourth-nerve palsy
- Sixth-nerve palsy
- Third-nerve palsy
- Orbital fracture
- Brainstem injury
- Concussion-related convergence insufficiency
- Vestibular dysfunction
- Decompensation of a previous phoria
New diplopia after head trauma requires medical evaluation even when the external eye appears normal.
Double Vision with Headache
Possible explanations include:
- Migraine
- Cranial-nerve palsy
- Aneurysm
- Raised intracranial pressure
- Stroke
- Giant cell arteritis
- Pituitary apoplexy
- Cavernous sinus disease
- Orbital inflammation
Seek emergency care for double vision with:
- A sudden severe headache
- Ptosis
- Unequal pupils
- Vomiting
- Neck stiffness
- Weakness
- Speech difficulty
- Loss of consciousness
Giant Cell Arteritis
In patients over 50, double vision may occasionally be a warning symptom of giant cell arteritis.
Other symptoms include:
- New headache
- Scalp tenderness
- Temple pain
- Jaw pain while chewing
- Fever
- Weight loss
- Fatigue
- Shoulder or hip stiffness
- Temporary or permanent visual loss
Urgent blood tests and treatment may be required to protect vision.
Raised Intracranial Pressure
Raised pressure around the brain may cause:
- Sixth-nerve palsy
- Double vision
- Headache
- Nausea
- Pulsatile tinnitus
- Brief episodes of visual dimming
- Optic-disc swelling
Possible causes include:
- Intracranial mass
- Venous sinus thrombosis
- Hydrocephalus
- Idiopathic intracranial hypertension
- Other neurological disorders
Can Migraine Cause Double Vision?
Migraine may cause visual aura, blur, light sensitivity and visual distortion.
True binocular diplopia is less typical and may be associated with:
- Migraine with brainstem aura
- Cranial-nerve dysfunction
- Another neurological cause occurring during a headache
A first episode of double vision should not be assumed to be migraine without assessment.
Double Vision in Children
Children with longstanding strabismus often suppress one image rather than report diplopia.
Sudden double vision in a child is therefore important.
Possible causes include:
- Acute strabismus
- Cranial-nerve palsy
- Head trauma
- Orbital infection
- Raised intracranial pressure
- Myasthenia gravis
- Neurological disease
- Decompensated congenital strabismus
Warning signs include:
- New eye deviation
- Head tilt
- Closing one eye
- Abnormal head posture
- Headache
- Vomiting
- Unsteady walking
- Drooping eyelid
- Unequal pupils
- Fever or eyelid swelling
Why Do Children with a Squint Often Not See Double?
A young child’s visual system may adapt by suppressing the image from the deviating eye.
This prevents diplopia but can cause:
- Amblyopia
- Reduced stereoscopic vision
- Loss of binocular visual development
Adults who develop a new squint are more likely to experience double vision because mature visual pathways are less able to suppress one image.
How Is Double Vision Examined?
History
The clinician asks:
- When did it begin?
- Was the onset sudden or gradual?
- Does it disappear when one eye is covered?
- Are the images horizontal, vertical or tilted?
- Is it worse at distance or near?
- Which direction of gaze makes it worse?
- Is there pain, headache or ptosis?
- Does it fluctuate with fatigue?
- Was there trauma?
- Are there neurological symptoms?
- Is there thyroid disease, diabetes or hypertension?
Visual Acuity and Refraction
Each eye is tested separately.
Refraction helps identify:
- Astigmatism
- Corneal optical problems
- Refractive ghosting
- Reduced vision contributing to poor fusion
Pinhole Testing
Monocular ghosting that improves through a pinhole often has an optical or refractive component.
Failure to improve may suggest:
- Cataract
- Irregular cornea
- Retinal disease
- More complex optical disturbance
Cover Testing
The cover test identifies whether either eye moves when fixation is interrupted.
It helps distinguish:
- Tropia
- Phoria
- Alternating deviation
- Intermittent misalignment
Ocular-Motility Examination
The patient follows a target through different gaze positions.
The clinician looks for:
- Underacting muscles
- Restricted movement
- Overacting muscles
- Abnormal jerking
- Pain on movement
- Patterns suggesting a nerve palsy
Prism Measurement
Prisms measure the degree of horizontal, vertical or torsional misalignment.
Measurements may be taken:
- At distance
- At near
- In different gaze directions
- With different head positions
This helps guide diagnosis and treatment.
Pupil and Eyelid Examination
The clinician checks for:
- Ptosis
- Eyelid retraction
- Fatigable eyelid weakness
- Unequal pupils
- Abnormal pupil reactions
- Proptosis
- Orbital swelling
Sudden ptosis with diplopia or a pupil abnormality increases concern for third-nerve palsy or other neurological disease.
Head-Tilt Testing
Head tilt may change vertical diplopia in:
- Fourth-nerve palsy
- Skew deviation
- Certain longstanding strabismus patterns
Patients may also adopt a compensatory head position to reduce image separation.
Orthoptic Assessment
An orthoptist specialises in eye alignment and binocular vision.
Assessment may include:
- Cover tests
- Prism measurements
- Fusion testing
- Stereopsis
- Convergence
- Hess or Lees screen testing
- Assessment of abnormal head posture
Orthoptic clinics commonly evaluate diplopia, ghosting and eye-movement disorders.
Slit-Lamp and Retinal Examination
These examinations look for monocular causes such as:
- Dry eye
- Corneal irregularity
- Cataract
- Lens displacement
- Intraocular lens problems
- Macular disease
Blood Tests
Depending on the suspected cause, tests may include:
- Blood glucose
- HbA1c
- Full blood count
- Inflammatory markers
- Thyroid function
- Thyroid antibodies
- Myasthenia antibodies
- Autoimmune or infectious testing
CT, MRI and Vascular Imaging
Imaging may be required when there is concern for:
- Aneurysm
- Stroke
- Tumour
- Brainstem disease
- Orbital mass
- Orbital cellulitis
- Orbital fracture
- Raised intracranial pressure
- Cavernous sinus disease
- Multiple cranial-nerve palsies
CT angiography or MR angiography may be used when an intracranial aneurysm is suspected.
Can Double Vision Be Diagnosed from a Photograph?
A photograph may show:
- A visible squint
- Ptosis
- Proptosis
- Abnormal head posture
- Eyelid swelling
It cannot reliably determine:
- Whether the diplopia is monocular or binocular
- The size of the deviation
- Eye movement in every direction
- Pupil reactions
- Optic-nerve function
- Neurological cause
- Whether urgent imaging is required
How Is Double Vision Treated?
Treatment depends on the cause.
Possible approaches include:
- Correcting refractive error
- Treating dry eye
- Cataract surgery
- Corneal treatment
- Temporary occlusion
- Prism glasses
- Orthoptic exercises
- Treating diabetes and vascular risk factors
- Thyroid-eye-disease treatment
- Myasthenia treatment
- Neurological treatment
- Botulinum toxin
- Strabismus surgery
Temporary Occlusion
Covering one eye removes binocular diplopia because the brain receives only one image.
Options include:
- Eye patch
- Frosted adhesive film
- Opaque contact lens
- Translucent tape over one spectacle lens
Complete black patches may reduce peripheral awareness and depth perception.
A translucent occlusion may be more comfortable for some patients.
Does It Matter Which Eye Is Covered?
Either eye may eliminate binocular diplopia.
The chosen eye depends on:
- Which eye sees better
- Dominance
- Field of vision
- Work tasks
- Comfort
- Cosmetic preference
Alternating the covered eye may sometimes reduce strain, but individual advice is preferable.
Prism Glasses
Prisms bend light so that the images can be brought closer together.
They may be:
- Temporary Fresnel prisms placed on spectacles
- Ground permanently into spectacle lenses
Prisms work best when the deviation is:
- Small or moderate
- Relatively similar in different gaze positions
- Stable
Limitations include:
- Blur from temporary Fresnel prisms
- Coloured fringes
- Limited correction of large deviations
- Incomplete correction when the deviation changes with gaze
Can Prism Cure the Cause?
No.
Prism aligns the images to relieve symptoms.
It does not restore a damaged cranial nerve or remove restrictive thyroid tissue.
It may be used:
- During spontaneous recovery
- As long-term treatment
- Before strabismus surgery
- When surgery is unsuitable
Orthoptic Exercises
Exercises may help selected conditions, particularly:
- Convergence insufficiency
- Reduced fusional reserves
- Certain decompensated phorias
Exercises are not appropriate for every cranial-nerve palsy, restrictive eye disease or neurological disorder.
Treating a Microvascular Nerve Palsy
Management may include:
- Controlling diabetes
- Managing blood pressure and cholesterol
- Smoking cessation
- Temporary prism or occlusion
- Monitoring recovery
- Imaging when indicated
Many presumed microvascular palsies improve over several weeks to months, but persistent or progressive symptoms require reassessment.
Treating Myasthenia Gravis
Treatment may include:
- Pyridostigmine
- Corticosteroids
- Other immune-modifying medication
- Thymectomy in selected patients
- Emergency respiratory support during myasthenic crisis
- Prism or occlusion for symptomatic diplopia
Because the deviation may fluctuate, permanent prism can be difficult to prescribe.
Treating Thyroid Eye Disease
Management depends on disease activity and severity.
Possible treatments include:
- Lubricants
- Smoking cessation
- Selenium in selected mild cases
- Steroids
- Other immune-modifying treatment
- Orbital radiotherapy
- Orbital decompression
- Strabismus surgery
- Eyelid surgery
Eye-muscle surgery is generally planned after active inflammation and measurements have stabilised.
Botulinum Toxin
Botulinum toxin may be injected into an eye muscle to weaken its action temporarily.
It may be used in selected:
- Acute nerve palsies
- Small-angle deviations
- Restrictive disorders
- Patients awaiting stability
- Patients unsuitable for surgery
Possible effects include:
- Temporary ptosis
- Vertical deviation
- Overcorrection or undercorrection
- Need for repeat treatment
Strabismus Surgery
Strabismus surgery adjusts the position or strength of one or more eye muscles.
It may be considered when:
- The deviation is stable
- Spontaneous recovery is unlikely
- Prism is inadequate
- Diplopia interferes with daily function
- An abnormal head posture is developing
Surgery aims to improve alignment in the most useful gaze positions.
It cannot always produce single vision in every direction.
Adjustable Sutures
Selected adult strabismus operations use adjustable sutures.
These allow limited postoperative modification of muscle position to improve alignment.
They are particularly useful in some:
- Complex deviations
- Restrictive disorders
- Previous strabismus operations
- Cranial-nerve palsies
- Thyroid eye disease cases
Will Double Vision Go Away?
The prognosis depends on the cause.
Double vision may improve after:
- Tear-film treatment
- Updated spectacles
- Cataract surgery
- Recovery of a microvascular nerve palsy
- Treatment of inflammation
- Recovery from trauma
- Control of myasthenia
- Prism or surgery
Persistent diplopia is more likely when there is:
- Permanent nerve damage
- Muscle fibrosis
- Significant orbital restriction
- Longstanding neurological disease
- Large or variable misalignment
Can I Drive with Double Vision?
Do not drive while experiencing uncontrolled double vision.
Diplopia can impair:
- Judgement of distance
- Lane position
- Pedestrian detection
- Reading road signs
- Reaction to moving objects
Driving may sometimes resume when the diplopia is reliably controlled by:
- Prism
- An approved occlusion method
- Successful treatment
- Strabismus surgery
Local licensing requirements apply.
Moorfields advises that diplopia must be controlled appropriately before driving.
Can I Work with Double Vision?
This depends on:
- Severity
- Occupation
- Need to drive
- Work at heights
- Machinery use
- Precision visual tasks
- Whether temporary occlusion is tolerated
Temporary workplace adjustments may include:
- Larger text
- Reduced screen glare
- Breaks
- Occlusion
- Prism
- Avoiding hazardous tasks
Frequently Asked Questions
Is double vision always neurological?
No.
Monocular diplopia commonly results from tear-film, corneal, refractive or lens problems.
Binocular diplopia may be neurological, muscular, mechanical or strabismic.
Is sudden double vision serious?
It can be.
Sudden onset requires prompt assessment, especially with headache, ptosis, pupil changes or neurological symptoms.
Can dry eye cause double vision?
Dry eye can produce monocular ghosting or multiple images that fluctuate with blinking.
It does not usually cause true binocular misalignment.
Can astigmatism cause double vision?
Yes.
It can cause monocular ghosting or shadowed images.
Can cataract cause double vision?
Yes.
Cataract may cause monocular diplopia that remains when the other eye is covered.
Can glaucoma cause double vision?
Chronic glaucoma does not usually cause diplopia directly.
Double vision may occur after:
- Glaucoma drainage surgery
- Advanced visual-field loss impairing fusion
- Another neurological or orbital disorder
- Coexisting cataract or corneal disease
Can a stroke cause only double vision?
Yes.
A small brainstem or cerebellar stroke may initially produce diplopia, imbalance or abnormal eye movements without obvious arm weakness.
Can high blood pressure cause double vision?
Hypertension may contribute to a microvascular cranial-nerve palsy.
It can also increase stroke risk.
Can diabetes cause double vision?
Yes.
Diabetes may affect the small blood vessels supplying cranial nerves III, IV or VI.
The diagnosis still requires assessment rather than assuming every palsy is diabetic.
Can double vision be caused by fatigue?
Fatigue may reveal:
- Myasthenia gravis
- A decompensated phoria
- Poor convergence
- Reduced fusion reserves
Persistent or new diplopia should not be dismissed as tiredness.
Why is the double vision worse at the end of the day?
Possible explanations include:
- Myasthenia gravis
- Decompensated phoria
- Fatigue-related loss of fusion
- Dry-eye ghosting
Why is the double vision worse at distance?
Possible causes include:
- Sixth-nerve palsy
- Distance esotropia
- Divergence insufficiency
- Sagging eye syndrome
- Decompensated horizontal alignment
Why is it worse during reading?
Possible causes include:
- Convergence insufficiency
- Fourth-nerve palsy
- Decompensated near phoria
- Refractive ghosting
- Dry eye
Why do I tilt or turn my head?
An abnormal head position may place the eyes in a direction where the image separation is smaller.
It may also compensate for torsion or vertical misalignment.
Does closing one eye harm the other eye?
Temporary occlusion in an adult does not usually damage the uncovered eye.
It reduces depth perception and field of view.
Prolonged occlusion in young children may contribute to amblyopia and should be medically supervised.
Can glasses fix binocular diplopia?
Ordinary spectacle power does not correct eye misalignment, but prism incorporated into the glasses may help.
Can double vision return after strabismus surgery?
Yes.
Alignment may change because of:
- Healing
- Scarring
- Progressive thyroid disease
- Neurological change
- Age-related muscle changes
- Recurrence of the original deviation
Can LASIK cause double vision?
LASIK may contribute to monocular ghosting through:
- Dry eye
- Irregular astigmatism
- Decentration
- Higher-order aberrations
True binocular diplopia may arise if refractive changes disrupt a previously controlled alignment problem.
Can double vision occur after new glasses?
Possible causes include:
- Incorrect prescription
- Excessive prism
- Optical-centre misalignment
- Large change in prescription
- Anisometropia
- Adaptation to progressive lenses
- A pre-existing phoria becoming symptomatic
Persistent symptoms should be checked.
Can double vision be psychological?
Functional visual symptoms are possible, but potentially serious ocular and neurological causes must first be excluded.
A Practical Urgency Guide
Emergency Assessment Now
- Sudden diplopia with severe headache
- Double vision with a new drooping eyelid
- Double vision with an enlarged or unequal pupil
- Double vision with weakness, numbness or speech difficulty
- Double vision with severe imbalance or collapse
- Double vision after significant head trauma
- Double vision with a bulging eye, fever or painful eye movement
- Double vision with swallowing or breathing difficulty
- Double vision with sudden vision loss
Same-Day or Prompt Assessment
- Any new persistent binocular diplopia
- Intermittent diplopia of recent onset
- Double vision with eye pain
- Double vision with ptosis
- Double vision with thyroid-eye symptoms
- Double vision following minor trauma
- Double vision that is progressively worsening
- New diplopia in a child
Routine Assessment May Be Appropriate
- Longstanding stable prism-controlled diplopia
- Stable monocular ghosting associated with known dry eye
- A previously assessed stable childhood squint
- Predictable convergence symptoms without neurological signs
A sudden change from the usual pattern makes the symptom urgent.
A Practical Diagnostic Approach
Step 1: Cover Each Eye
Determine whether the symptom is:
- Monocular
- Binocular
Step 2: Describe the Images
- Horizontal
- Vertical
- Diagonal
- Rotated
- Clear second image
- Faint ghost
Step 3: Determine the Pattern
- Sudden or gradual
- Constant or intermittent
- Distance or near
- Worse in one gaze direction
- Worse with fatigue
Step 4: Look for Red Flags
- Headache
- Ptosis
- Unequal pupils
- Neurological symptoms
- Trauma
- Proptosis
- Fever
- Swallowing or breathing difficulty
Step 5: Examine the Eye Optically
Assess:
- Tear film
- Refraction
- Cornea
- Lens
- Macula
Step 6: Examine Alignment and Movement
Assess:
- Cover test
- Ocular motility
- Prism measurements
- Head position
- Pupil and eyelid function
Step 7: Investigate the Underlying Cause
Possible tests include:
- Blood tests
- CT
- MRI
- Vascular imaging
- Thyroid testing
- Myasthenia testing
- Orbital imaging
Step 8: Relieve Symptoms Safely
Consider:
- Temporary occlusion
- Fresnel prism
- Permanent prism
- Exercises in selected conditions
Step 9: Treat the Cause
Treatment may involve:
- Lubrication
- Spectacles
- Cataract surgery
- Neurological treatment
- Immune therapy
- Orbital treatment
- Botulinum toxin
- Strabismus surgery
Common Myths About Double Vision
“Double vision is always caused by weak eye muscles.”
False.
It may result from optical problems, nerve palsies, brain disease, orbital restriction or neuromuscular disease.
“If covering one eye fixes it, the problem is harmless.”
False.
This confirms binocular diplopia but does not identify the cause.
“A normal pupil excludes an aneurysm.”
False.
Acute third-nerve palsy requires urgent assessment even when the pupil initially appears normal.
“Diabetes explains every new nerve palsy.”
False.
Aneurysm, stroke, inflammation, tumour and other causes must still be considered.
“Double vision from fatigue is never serious.”
False.
Myasthenia gravis and decompensated neurological disorders may worsen with fatigue.
“Prism cures the underlying disease.”
False.
Prism relieves image separation but does not treat the cause.
“Children with a squint always see double.”
False.
Young children commonly suppress one image and may instead develop amblyopia.
“A clear eye examination excludes a neurological cause.”
False.
The cornea, lens and retina may appear normal in cranial-nerve palsies, myasthenia and brainstem disease.
The Bottom Line
Double vision may be monocular or binocular.
Monocular Double Vision
Persists when the other eye is covered.
Common causes include:
- Dry eye
- Astigmatism
- Irregular cornea
- Keratoconus
- Cataract
- Lens displacement
- Macular disease
Binocular Double Vision
Disappears when either eye is covered.
Possible causes include:
- Strabismus
- Decompensated phoria
- Cranial-nerve palsy
- Stroke
- Myasthenia gravis
- Thyroid eye disease
- Orbital disease
- Raised intracranial pressure
- Head trauma
Seek emergency care for sudden diplopia accompanied by:
- Severe headache
- Ptosis
- An enlarged or unequal pupil
- Weakness or numbness
- Speech difficulty
- Severe imbalance
- Fever and orbital swelling
- Swallowing or breathing difficulty
- Sudden loss of vision
Do not drive with uncontrolled diplopia.
Temporary occlusion or prism may relieve the symptom, but effective treatment depends on identifying the underlying optical, muscular, neurological or orbital cause.
The most important first question is simple: does the double vision remain when one eye is covered? The answer separates optical ghosting from eye misalignment—but any new binocular double vision still deserves prompt assessment because the cause may lie anywhere from the eye muscles to the brain.
References
- National Health Service. Double Vision.
- American Academy of Ophthalmology. When Is Diplopia a Sign of Something Dangerous?
- Mackay DD. Approach to Diplopia. Continuum. 2025.
- Najem K, et al. Diplopia. StatPearls. Updated 2024.
- National Eye Institute. Convergence Insufficiency. Updated December 2024.
- National Eye Institute. Graves’ Eye Disease. Updated November 2024.
- National Health Service. Myasthenia Gravis.
- University Hospitals Sussex. Myasthenia Gravis. Updated April 2026.
- American Academy of Ophthalmology. Diagnostic Considerations in an Acquired, Isolated Third-Nerve Palsy. 2024.
- American Academy of Ophthalmology. Third-Nerve Palsy.
- American Academy of Ophthalmology. Basic Approach to Diplopia.
- National Eye Institute. Refractive Errors. Updated December 2025.
- National Eye Institute. Corneal Dystrophies and Keratoconus. Updated December 2024.
- Moorfields Eye Hospital. Diplopia, Double Vision and Driving.
- National Health Service. Transient Ischaemic Attack: Symptoms.