Author: Dr Val Phua
Estimated reading time: 11–13 minutes
Why Am I Seeing Flashes When There Is No Light?
Flashes of light in the vision are known medically as photopsia.
They may appear as:
- Lightning streaks
- Brief arcs of light
- Camera-like flashes
- Flickering at the side of the vision
- Sparkles or stars
- Shimmering or zigzag patterns
Many flashes occur when the vitreous gel inside the eye pulls on the retina. This is common during a posterior vitreous detachment, an age-related process in which the vitreous separates from the retina.
Most posterior vitreous detachments do not cause permanent damage. However, vitreous traction can sometimes create a retinal tear, which may progress to retinal detachment.
Arrange a prompt dilated retinal examination if flashes are:
- New
- Suddenly more frequent
- Confined mainly to one eye
- Accompanied by new floaters
- Associated with blurred vision
- Followed by a curtain or shadow
Retinal tears and detachments are usually painless. The absence of pain does not make new flashes safe to ignore.
What Causes the Sensation of a Flash?
The retina is the light-sensitive tissue lining the inside of the back of the eye.
Normally, retinal cells respond when light enters the eye. However, mechanical pulling, irritation or abnormal stimulation of the retina can produce an electrical signal even when no external light is present.
The brain interprets this signal as a flash.
This is similar to seeing stars briefly after mechanical pressure near the eye, although unexplained or repeated flashes should not be attributed to pressure without appropriate assessment.
What Do Vitreous or Retinal Flashes Usually Look Like?
Flashes caused by vitreous traction commonly appear as:
- Brief lightning-like streaks
- Curved arcs
- White or pale flashes
- Flickering at the outer edge of vision
- Flashes triggered by eye or head movement
- Symptoms that are more noticeable in darkness
They usually last for less than a second at a time but may recur intermittently over days or weeks.
These flashes generally occur in one eye because the traction is happening within that particular eye. Patients may nevertheless find it difficult to identify which eye is affected without testing each eye separately.
What Is Posterior Vitreous Detachment?
The vitreous is a transparent gel filling most of the inside of the eye.
When we are young, it is relatively firm and attached to the retina. With age, the vitreous becomes more liquefied, shrinks and begins separating from the retinal surface.
This process is called a posterior vitreous detachment, or PVD.
Typical symptoms include:
- Flashes at the side of the vision
- Sudden new floaters
- A ring-shaped floater
- Cobwebs or threads
- Temporary visual haze
The flashes occur because the separating vitreous pulls on the retina. Once the vitreous has completely released and the traction settles, the flashes usually become less frequent.
Is Posterior Vitreous Detachment Dangerous?
Most PVDs are uncomplicated.
The American Society of Retina Specialists reports that approximately 85% of patients with PVD do not develop a serious complication, and flashes and floaters usually become less noticeable over the following weeks or months.
However, the vitreous may remain strongly attached to a small area of retina. As it separates, this traction can:
- Pull on a retinal blood vessel.
- Cause vitreous haemorrhage.
- Create a retinal tear.
- Allow fluid through the tear.
- Produce a retinal detachment.
A retinal examination is therefore required to distinguish an uncomplicated PVD from a retinal tear.
How Often Is a Retinal Tear Found?
In a large prospective study of patients presenting with symptomatic PVD, approximately 9.9% had an associated retinal tear or retinal detachment at the initial assessment.
A further 3% of patients whose first examination did not identify a tear developed one during the subsequent two months.
Importantly, 15% of retinal tears in the study were detected only through indirect ophthalmoscopy with scleral depression, highlighting why retinal photographs alone may not be sufficient to exclude an acute peripheral tear.
What Symptoms Suggest a Retinal Tear?
A retinal tear may cause:
- Sudden flashes
- A marked increase in floaters
- A shower of black, pepper-like dots
- A dark or reddish cloud
- Blurred vision
The black dots may represent retinal pigment cells or blood released into the vitreous when the retina tears.
A tear may still be present even if the flashes become less frequent. Symptoms alone cannot determine whether the retina is intact.
What Symptoms Suggest a Retinal Detachment?
Seek emergency eye care if flashes or floaters are accompanied by:
- A dark curtain or veil
- A shadow entering from one side
- Loss of peripheral vision
- A missing area of the visual field
- Sudden persistent blurred vision
- Sudden central visual loss
A retinal detachment occurs when fluid passes through a retinal tear and lifts the retina away from the back wall of the eye.
The shadow may initially be peripheral and move towards the centre as more retina detaches. Prompt treatment provides the best opportunity to preserve vision.
When Should I Seek Urgent Eye Care?
Arrange a prompt, preferably same-day, retinal examination when you notice:
- New flashes in one eye
- Suddenly more frequent flashes
- Flashes with new floaters
- Numerous black dots
- A dark cloud or visual haze
- Reduced or blurred vision
- Symptoms following an eye injury
- New symptoms after cataract or retinal surgery
Seek emergency care immediately for:
- A curtain or shadow
- Missing peripheral vision
- Sudden persistent visual loss
- Rapid worsening of symptoms
Do not wait to see whether flashes settle on their own.
Who Is at Greater Risk of a Retinal Tear?
The likelihood of retinal complications is higher with:
- Increasing age
- Moderate or high myopia
- Lattice degeneration
- Previous retinal tear or detachment
- Retinal detachment in the other eye
- Family history of retinal detachment
- Recent cataract or other intraocular surgery
- Significant eye trauma
- Vitreous haemorrhage
Longer eyes and pseudophakic eyes were associated with a higher risk of retinal tears or detachment among patients with symptomatic PVD in the prospective community study.
Why Does High Myopia Increase the Risk?
A highly myopic eye is usually longer than average.
This may be associated with:
- Earlier vitreous degeneration
- Earlier PVD
- Peripheral retinal thinning
- Lattice degeneration
- Retinal tears
- Retinal detachment
LASIK, SMILE, PRK or ICL surgery corrects the focusing error but does not shorten the eyeball. A patient who previously had high myopia therefore retains the associated retinal risk.
Can Cataract Surgery Cause Flashes?
New flashes may develop after cataract surgery because:
- A PVD develops around the time of surgery.
- Existing vitreous changes become more noticeable.
- The clearer artificial lens makes visual symptoms easier to see.
- Rarely, a retinal tear or detachment has occurred.
Previous cataract surgery is a recognised risk factor for retinal detachment. New flashes, floaters or a curtain after surgery require prompt retinal examination rather than being assumed to be part of normal recovery.
Can Eye Trauma Cause Flashes?
Yes.
A blunt impact may deform the eye and pull on the retina, causing:
- Retinal commotio
- Retinal tear
- Retinal dialysis
- Vitreous haemorrhage
- Retinal detachment
- Choroidal injury
Examples include being struck by a ball, falling, road-traffic injuries and workplace accidents.
Flashes may occur immediately or appear later. A significant eye injury should be examined even when the initial central vision appears relatively good.
Can Migraine Cause Flashes of Light?
Yes.
Migraine aura can produce visual symptoms such as:
- Shimmering lights
- Zigzag lines
- Flickering patterns
- Bright spots
- Geometric shapes
- An expanding blind spot
- A crescent or kaleidoscope pattern
Unlike brief retinal flashes, a migraine aura generally develops gradually, spreads across part of the visual field and lasts approximately 5–60 minutes.
Because migraine aura originates in the visual areas of the brain, it typically affects the visual field of both eyes, even when the pattern seems more prominent on one side. A headache may follow, occur simultaneously or be entirely absent.
Retinal Flashes Versus Migraine Aura
| Feature | Vitreous or retinal traction | Migraine aura |
|---|---|---|
| Usual appearance | Brief arc, streak or lightning flash | Shimmering, zigzag or expanding geometric pattern |
| Eye affected | Usually one eye | Usually visible through both eyes |
| Duration | Often less than a second at a time, repeatedly | Usually develops and lasts 5–60 minutes |
| Location | Often peripheral | May spread across the central or peripheral visual field |
| Floaters | May occur at the same time | Not usually caused by the aura |
| Curtain or shadow | Concerning for detachment | Not typical of an ordinary aura |
| Headache | Usually absent | May occur before, during or after; sometimes absent |
This comparison is only a guide. A first episode, an unusual pattern or symptoms clearly confined to one eye should be medically assessed rather than diagnosed as migraine at home.
How Can I Tell Whether the Flashes Affect One Eye or Both?
While the symptom is occurring:
- Cover the right eye.
- Observe whether the pattern remains.
- Cover the left eye.
- Compare what you see.
A migraine aura arising from the brain generally remains visible with either eye covered because it affects the same area of the visual field in both eyes.
A retinal flash usually disappears when the affected eye is covered.
However, patients may find this distinction difficult, particularly when symptoms are brief. Uncertainty should favour examination rather than reassurance.
What Is an “Ocular Migraine”?
The term ocular migraine is used inconsistently and can cause confusion.
It is often used to describe migraine with visual aura, which generally affects both eyes.
True retinal migraine is much rarer and causes fully reversible visual disturbance in one eye. Other causes of temporary monocular visual loss—particularly retinal or vascular disease—must be excluded before retinal migraine is diagnosed.
Do not assume that new one-eye flashes, dimming or loss of vision are “just an ocular migraine,” especially when the episode differs from previous symptoms.
When Might Visual Symptoms Be Neurological?
Medical assessment is important when flashes or visual disturbance are associated with:
- New weakness or numbness
- Difficulty speaking
- Facial drooping
- Confusion
- Loss of coordination
- Persistent double vision
- A new severe headache
- Loss of consciousness
- Visual loss that does not fully recover
Migraine aura can cause temporary sensory or speech symptoms, but a first or atypical neurological episode may resemble a transient ischaemic attack or another neurological emergency.
Can Inflammation Cause Flashes?
Inflammation inside the eye may irritate the retina or vitreous and produce flashes or floaters.
Associated symptoms may include:
- Eye pain
- Redness
- Light sensitivity
- Blurred vision
- Numerous small floaters
Possible causes include uveitis, retinal inflammation and infection.
Flashes accompanied by pain, redness or marked light sensitivity require assessment because this pattern is not typical of an uncomplicated age-related PVD.
Can Rubbing or Pressing the Eye Cause Flashes?
Mechanical pressure on the eye may briefly stimulate the retina and produce rings, sparks or stars known as phosphenes.
This should not be used to test the retina, and repeated eye rubbing may damage the ocular surface or worsen other eye conditions.
Spontaneous, repeated or persistent flashes should not be attributed to rubbing unless the relationship is clear and the symptoms stop completely when pressure is avoided.
Can Screens or Blue Light Cause Flashes?
Normal computer and smartphone use does not generally cause vitreous traction, retinal tears or true retinal flashes.
Screens may contribute to:
- Eye strain
- Dryness
- Glare
- After-images
- Increased awareness of visual symptoms
- Migraine triggering in susceptible individuals
New lightning-like peripheral flashes should not be dismissed as screen fatigue.
Are After-Images the Same as Flashes?
No.
An after-image may appear after looking at a bright light, camera flash or high-contrast image. It usually resembles the original object and fades gradually.
Retinal traction flashes often occur without a bright external stimulus and appear as brief arcs or lightning streaks.
Persistent after-images or visual patterns unrelated to light exposure may require assessment for retinal, neurological or medication-related causes.
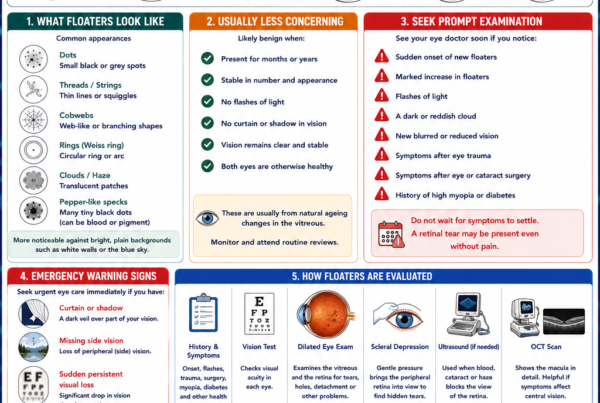
How Are Flashes Investigated?
Symptom History
Your ophthalmologist may ask:
- When the flashes began
- Whether they are sudden or gradual
- Whether they affect one eye or both
- How long each episode lasts
- Whether new floaters are present
- Whether there is blur, a curtain or shadow
- Whether there was recent surgery or trauma
- Whether you have high myopia
- Whether similar migraine symptoms occurred previously
The description helps guide the diagnosis but cannot exclude a retinal tear.
Visual-Acuity Testing
Vision is checked in each eye.
Good central vision does not exclude a peripheral retinal tear or early detachment.
Pupil Examination
Pupil responses are assessed for signs of significant retinal or optic-nerve dysfunction.
Slit-Lamp Examination
The front of the eye and the anterior vitreous are examined.
The ophthalmologist looks for:
- Pigment cells
- Blood
- Inflammatory cells
- Cataract
- Previous surgical changes
- Other ocular abnormalities
Pigment or blood in the vitreous may increase concern for an acute retinal tear.
Dilated Retinal Examination
Dilating drops enlarge the pupil so that the vitreous and retina can be examined.
The examination looks for:
- Posterior vitreous detachment
- Retinal tears
- Retinal holes
- Lattice degeneration
- Vitreous haemorrhage
- Retinal detachment
- Inflammation
- Other retinal disease
A thorough peripheral retinal examination is the key assessment for new unilateral flashes.
Scleral Depression
Scleral depression involves gentle pressure through the eyelid or on the outside of the eye while the peripheral retina is examined.
It brings the far retinal periphery into view, where many tears occur.
The examination may feel unusual or briefly uncomfortable. It is important because some retinal tears are not visible through slit-lamp examination or widefield photography alone.
Widefield Retinal Photography
Widefield imaging can document a broad area of the retina and may help:
- Record the location of retinal lesions
- Compare future examinations
- Document laser treatment
- Explain findings to the patient
However, it may not visualise the entire extreme peripheral retina. It does not automatically replace dilated examination with scleral depression when acute flashes suggest a tear.
Optical Coherence Tomography
OCT creates detailed cross-sectional images of the macula.
It may identify:
- Vitreomacular traction
- Macular hole
- Epiretinal membrane
- Macular swelling
- Other central retinal conditions
A normal macular OCT does not exclude a tear in the peripheral retina.
Ocular Ultrasound
Ultrasound may be required if the retina cannot be seen clearly because of:
- Vitreous haemorrhage
- Dense cataract
- Corneal opacity
- Significant inflammation
It can help detect retinal detachment and other large abnormalities.
A small tear may remain difficult to identify, so repeat examination may still be necessary as the view improves.
What Happens If the First Examination Is Normal?
A normal initial examination is reassuring but does not eliminate all future risk.
The vitreous separation may still be progressing, and a delayed tear may occasionally develop.
The follow-up schedule depends on:
- Severity of symptoms
- High myopia
- Lattice degeneration
- Vitreous haemorrhage
- Previous retinal tear or detachment
- Recent eye surgery
- Whether the peripheral retina was fully visible
- Findings in the other eye
The prospective PVD study found that approximately 3% of patients without a tear at presentation developed one during the following two months.
Attend the advised review, but return earlier if:
- Flashes increase
- New floaters appear
- Vision becomes blurred
- A dark cloud develops
- A curtain or shadow appears
How Are Flashes Treated?
Treatment depends on the cause.
Uncomplicated Posterior Vitreous Detachment
No treatment is usually needed for the PVD itself.
Flashes generally become less frequent as vitreous separation completes and traction on the retina reduces.
Patients require:
- Retinal examination
- Follow-up when advised
- Education about warning symptoms
- Immediate reassessment if symptoms change
Most patients no longer notice significant flashes after several weeks or months.
Retinal Tear
A symptomatic tractional retinal tear is commonly treated with:
- Laser photocoagulation
- Cryotherapy in selected cases
Laser or freezing treatment creates a strong adhesion around the tear and reduces the risk of fluid passing underneath the retina.
Treatment may prevent a retinal detachment, but flashes and floaters may take time to settle because the vitreous separation is still occurring.
Retinal Detachment
An established detachment generally requires surgery.
Possible procedures include:
- Pneumatic retinopexy
- Scleral buckle surgery
- Vitrectomy
- A combination of procedures
The choice depends on the location and number of tears, extent of detachment, lens status and whether the macula remains attached.
Migraine Aura
Migraine-related visual symptoms are treated as part of the underlying migraine disorder.
Management may include:
- Identifying triggers
- Regular sleep and meals
- Acute migraine medication
- Preventive medication when attacks are frequent
- Medical or neurological review for atypical episodes
A first episode of apparent migraine aura, particularly later in life or without a previous migraine history, may require assessment to exclude retinal and neurological causes.
Ocular Inflammation
Inflammation requires treatment directed at its cause and may involve:
- Anti-inflammatory eye drops
- Dilating medication
- Antimicrobial treatment
- Systemic investigation
- Oral or injected medication in selected cases
Steroid eye drops should not be started without professional supervision because they may worsen certain infections and raise eye pressure.
Frequently Asked Questions
Are flashes of light always serious?
No.
Many are caused by an uncomplicated PVD or migraine aura. However, new flashes require assessment because symptoms alone cannot distinguish a harmless PVD from a retinal tear.
Are retinal flashes usually in one eye?
Yes.
Vitreous traction and retinal tears affect an individual eye. Migraine aura generally affects the visual fields of both eyes.
Why are flashes more noticeable at night?
The bright flash contrasts more strongly against a dark background. Darkness may also make brief peripheral photopsias easier to detect.
Why do flashes occur when I move my eyes?
Eye movement shifts the vitreous and may increase momentary traction on an area where it remains attached to the retina.
How long do PVD flashes last?
Individual flashes are brief, but they may recur for days or weeks. Most become less frequent as the vitreous separation settles. Some patients notice occasional flashes for longer.
Can flashes stop even when a retinal tear is present?
Yes.
A reduction in flashes does not prove that the retina is intact. The tear may remain even after traction reduces.
Can artificial tears treat flashes?
No.
Artificial tears treat the ocular surface and do not affect vitreous traction or retinal disease.
Can vitamins stop flashes?
No vitamin or supplement has been shown to stop flashes caused by PVD or prevent a retinal tear.
Can I exercise when experiencing new flashes?
New flashes should be assessed before assuming that strenuous activity is safe.
Once a retinal tear or detachment has been excluded, your ophthalmologist can advise whether any temporary activity restriction is needed.
Should I drive while having flashes?
Do not drive if flashes, migraine aura, blurred vision or a visual-field defect interferes with safe vision.
Pull over safely if a new visual disturbance begins while driving.
Can flashes occur after retinal laser?
Yes.
The underlying PVD may continue producing flashes even after a tear has been successfully surrounded with laser.
A new increase in symptoms still requires reassessment because another tear can develop elsewhere.
Can both eyes develop PVD?
Yes.
PVD commonly develops in both eyes at different times. The second eye may develop symptoms months or years after the first.
Does a normal retinal photograph exclude a tear?
Not always.
A small tear in the extreme peripheral retina may not appear on standard or widefield photographs. A careful dilated examination, often with scleral depression, remains important for acute symptoms.
A Practical Triage Guide
| Visual symptom | Recommended action |
| Longstanding occasional flashes already assessed and unchanged | Continue planned monitoring |
| New brief peripheral flashes in one eye | Arrange prompt dilated retinal examination |
| Flashes with sudden new floaters | Seek same-day assessment |
| Flashes with numerous pepper-like dots or a dark cloud | Seek urgent assessment |
| Flashes after eye trauma or surgery | Seek prompt ophthalmic assessment |
| Curtain, shadow or missing side vision | Emergency eye care immediately |
| Gradually spreading zigzag pattern lasting 5–60 minutes in both eyes, similar to previous migraine aura | Follow established migraine advice, but seek review if the pattern changes |
| First-ever visual aura, persistent symptoms or associated neurological deficits | Seek medical assessment promptly |
The Bottom Line
Flashes of light may arise from the eye or the brain.
The most common ocular cause is vitreous traction during posterior vitreous detachment. Most PVDs are uncomplicated, but approximately one in ten symptomatic patients may have an associated retinal tear or detachment at presentation.
Seek prompt retinal examination for:
- New flashes
- Flashes mainly in one eye
- Flashes with new floaters
- A pepper-like shower of dots
- A dark cloud
- Blurred or reduced vision
- Symptoms after injury or surgery
Seek emergency care for:
- A curtain or shadow
- Missing peripheral vision
- Sudden persistent visual loss
Migraine aura more often produces a gradually spreading, shimmering or zigzag pattern affecting both eyes and lasting several minutes. A first, unusual or one-eye episode should not automatically be labelled migraine.
New flashes are a warning symptom until the peripheral retina has been properly examined.
References
- Kim SJ, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern. Ophthalmology. 2025.
- National Eye Institute. Vitreous Detachment. Updated December 2024.
- National Eye Institute. Retinal Detachment. Updated November 2025.
- American Society of Retina Specialists. Posterior Vitreous Detachment.
- American Society of Retina Specialists. Retinal Tears.
- Nixon TRW, et al. Posterior Vitreous Detachment and Retinal Tear: A Prospective Study of Community Referrals. Eye. 2024.
- International Headache Society. International Classification of Headache Disorders: Migraine With Aura.
- National Institute of Neurological Disorders and Stroke. Migraine. Updated July 2026.