Author: Dr Val Phua
Estimated reading time: 11–13 minutes
Diabetes Can Damage the Retina Before You Notice Any Change in Vision
Diabetic retinopathy is a complication of diabetes that damages the small blood vessels supplying the retina—the light-sensitive tissue lining the back of the eye.
In its early stages, diabetic retinopathy usually causes no symptoms. A person may have clear vision and remain unaware that retinal blood vessels are already leaking, closing or becoming abnormal.
As the condition progresses, it may cause:
- Blurred or fluctuating vision
- Difficulty reading
- Dark floaters or cobweb-like shadows
- Distorted central vision
- Poorer colour or contrast
- Sudden visual loss
Regular retinal screening is therefore important for everyone with diabetes, even when their eyesight appears normal. Early detection and timely treatment can greatly reduce the risk of severe visual loss.
What Is the Retina?
The retina is a thin layer of specialised nerve tissue lining the inside of the back of the eye.
It receives light and converts visual information into electrical signals that travel through the optic nerve to the brain.
The central part of the retina is called the macula. It provides the detailed vision needed for:
- Reading
- Recognising faces
- Driving
- Seeing colours
- Performing fine visual tasks
Diabetic retinopathy may affect the peripheral retina, the macula or both.
How Does Diabetes Damage the Retina?
Persistently elevated blood glucose damages blood vessels throughout the body, including the tiny capillaries supplying the retina.
Over time, retinal blood vessels may:
- Develop weakened areas called microaneurysms
- Leak blood
- Leak fluid and fatty deposits
- Become blocked
- Reduce the retina’s oxygen supply
- Stimulate fragile new blood-vessel growth
These new vessels do not function normally. They can bleed easily, produce scar tissue and eventually pull the retina away from the back of the eye.
Diabetes may therefore threaten vision through leakage, retinal swelling, bleeding, poor oxygen supply and tractional retinal detachment.
Does Everyone with Diabetes Develop Diabetic Retinopathy?
Anyone with type 1 or type 2 diabetes can develop diabetic retinopathy.
The risk generally increases with:
- Longer duration of diabetes
- Higher blood-glucose levels over time
- High blood pressure
- High cholesterol
- Kidney disease
- Pregnancy in women with pre-existing diabetes
- Smoking
- Anaemia
- Puberty
- Existing diabetic retinopathy
Good diabetes control lowers the risk but does not remove it completely. Retinal screening remains necessary even when the HbA1c is satisfactory and there are no visual symptoms.
What Are the Stages of Diabetic Retinopathy?
Diabetic retinopathy is broadly classified into:
- Non-proliferative diabetic retinopathy
- Proliferative diabetic retinopathy
Diabetic macular oedema may occur at either stage.
Non-Proliferative Diabetic Retinopathy
Non-proliferative diabetic retinopathy, or NPDR, is the earlier and more common stage.
The damaged retinal blood vessels may leak, bleed or become blocked, but abnormal new vessels have not yet grown.
NPDR may be described as mild, moderate or severe.
Mild NPDR
The earliest visible changes may include small microaneurysms—tiny balloon-like swellings in the retinal capillaries.
Vision is usually unaffected at this stage.
Moderate NPDR
As disease progresses, additional findings may appear, including:
- Small retinal haemorrhages
- Fluid leakage
- Hard exudates
- Cotton-wool spots
- Venous changes
- Areas of reduced retinal blood flow
Vision may remain good unless the macula becomes swollen.
Severe NPDR
In severe NPDR, more retinal blood vessels are blocked and larger areas of the retina become deprived of oxygen.
The eye has not yet developed definite new vessels, but the risk of progressing to proliferative disease is significantly greater.
Closer monitoring or treatment may be recommended depending on the retinal findings, follow-up reliability and whether the other eye already has advanced disease.
Proliferative Diabetic Retinopathy
Proliferative diabetic retinopathy, or PDR, is a more advanced stage.
When the retina receives insufficient oxygen, it releases signals that stimulate the growth of abnormal new blood vessels.
These fragile vessels may grow:
- On the retinal surface
- Around the optic nerve
- Into the vitreous gel
- Over the front of the eye in very advanced disease
They can cause severe visual loss through:
- Vitreous haemorrhage
- Fibrous scar formation
- Tractional retinal detachment
- Neovascular glaucoma
Proliferative retinopathy may remain painless even when vision is under serious threat.
What Is Diabetic Macular Oedema?
Diabetic macular oedema, or DME, occurs when damaged retinal vessels leak fluid into the macula.
The macula may become thickened or swollen, causing:
- Blurred central vision
- Distorted vision
- Difficulty reading
- Reduced contrast
- Colours appearing washed out
- Difficulty recognising faces
DME may develop during mild, moderate, severe or proliferative diabetic retinopathy. It is therefore considered separately from the overall retinopathy stage.
The National Eye Institute estimates that approximately 1 in 15 people with diabetes develops diabetic macular oedema.
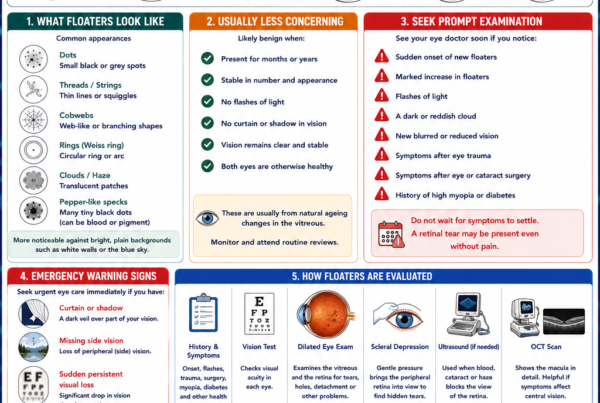
What Symptoms Can Diabetic Retinopathy Cause?
Early Disease Often Has No Symptoms
A patient may have significant retinal changes while still reading the smallest line on an eye chart.
Clear vision does not prove that the retina is healthy.
This is why screening should begin according to the type and duration of diabetes rather than waiting for symptoms.
Blurred or Fluctuating Vision
Blur may result from:
- Diabetic macular oedema
- Bleeding inside the eye
- Cataracts
- Rapid changes in blood glucose
- Changes in spectacle prescription
- Retinal detachment
Fluctuating glucose levels can temporarily alter the focusing power of the natural lens, causing vision to vary even without retinopathy.
Patients should avoid repeatedly changing spectacles while glucose levels remain unstable unless advised otherwise.
Floaters or Cobwebs
New abnormal blood vessels may bleed into the vitreous gel.
Patients may notice:
- Dark dots
- Threads
- Cobweb-like shadows
- Red or black clouds
- A sudden shower of floaters
A small haemorrhage may partially clear, but this does not mean the underlying abnormal vessel has healed.
New floaters or hazy vision in a person with diabetes requires prompt retinal assessment.
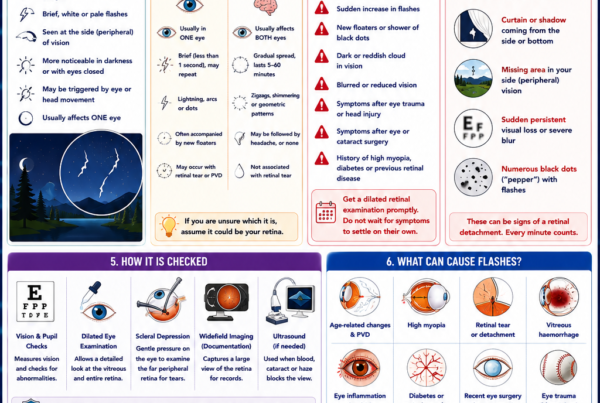
Sudden Visual Loss
Sudden vision loss may occur because of:
- Dense vitreous haemorrhage
- Severe macular oedema
- Retinal artery or vein occlusion
- Tractional retinal detachment
- Neovascular glaucoma
- Another unrelated eye emergency
Do not wait for a routine diabetic screening appointment if vision changes suddenly.
A Shadow or Curtain
A curtain, shadow or missing area of vision may indicate retinal detachment.
Advanced diabetic retinopathy can produce scar tissue that contracts and pulls the retina away from the wall of the eye. This is known as a tractional retinal detachment.
Urgent retinal assessment is required, particularly if central vision is affected.
Eye Pain and Redness
Ordinary diabetic retinopathy is usually painless.
Pain, redness, headache or nausea may occur if abnormal blood vessels block the eye’s drainage system and cause neovascular glaucoma.
A painful red eye with reduced vision requires urgent assessment.
How Often Should People with Diabetes Have Their Eyes Checked?
The appropriate interval depends on the type of diabetes, duration, retinal findings, pregnancy and overall medical control.
Type 1 Diabetes
Adults with type 1 diabetes should generally have their first comprehensive dilated eye examination within five years after the onset of diabetes.
Retinopathy usually takes time to develop after the onset of hyperglycaemia, but subsequent screening remains important throughout life.
Type 2 Diabetes
People with type 2 diabetes should have a comprehensive eye examination at the time diabetes is diagnosed.
Type 2 diabetes may have been present for several years before it is detected, so retinal changes may already be present at diagnosis.
Follow-Up When No Retinopathy Is Present
Annual retinal screening is a practical standard for many patients.
Under the American Diabetes Association’s 2026 guidance, screening every one to two years may be considered when one or more annual examinations show no retinopathy and blood-glucose control remains within the agreed target range.
In Singapore, annual diabetic retinal screening remains widely used and is readily available through diabetic retinal photography programmes.
Follow-Up When Retinopathy Is Present
If any diabetic retinopathy is detected, examinations should occur at least annually and usually more frequently according to severity.
Patients with more advanced disease, macular oedema or recent treatment may need review:
- Every two to four months
- Every few weeks during injection treatment
- At other intervals determined by OCT and retinal findings
The treating ophthalmologist will individualise the schedule.
A Practical Screening Guide
| Situation | Suggested first examination or interval |
|---|---|
| Type 1 diabetes | Within 5 years of onset |
| Type 2 diabetes | At the time of diagnosis |
| No retinopathy on repeated screening and stable medical control | Every 1–2 years may be considered |
| Any diabetic retinopathy | At least annually, often more frequently |
| Sight-threatening retinopathy or DME | Specialist review according to severity and treatment |
| Pre-existing diabetes and pregnancy | Before conception or during the first trimester, with follow-up during pregnancy |
| New floaters, blur, distortion or visual loss | Prompt assessment—do not wait for scheduled screening |
These are general recommendations. Individual follow-up may be more frequent according to retinal findings and systemic risk.
Diabetic Retinal Photography in Singapore
Diabetic retinal photography is a screening test that photographs the retina to look for diabetic changes.
In Singapore, DRP is available through polyclinics, selected family medicine clinics and community health services. Images are captured by trained staff and assessed for signs that require referral. HealthHub describes DRP as an important means of detecting early retinal changes and preventing avoidable blindness.
Retinal photography is useful because:
- It is quick and non-invasive.
- It creates a permanent retinal record.
- It can identify many patients who require referral.
- It improves access to diabetic eye screening.
- Validated digital imaging may be used as an effective screening method.
However, photography is not a complete substitute for an ophthalmologist’s examination when:
- Images are ungradable
- Retinopathy is present
- Vision has changed
- Macular oedema is suspected
- There is another eye condition
- The peripheral retina needs detailed examination
An abnormal screening result requires appropriate referral and follow-up.
What Happens During a Diabetic Eye Examination?
Visual Acuity
Vision is checked in each eye.
Reduced vision may result from diabetic retinopathy, macular oedema, cataracts, glaucoma or another eye condition.
Eye Pressure
Eye pressure may be measured because diabetes is associated with a higher risk of glaucoma, and advanced retinopathy can cause neovascular glaucoma.
Slit-Lamp Examination
The front of the eye is examined for:
- Cataract
- Corneal disease
- Abnormal blood vessels on the iris
- Inflammation
- Other diabetic eye changes
Dilated Retinal Examination
Dilating drops enlarge the pupils so that the ophthalmologist can examine the retina and optic nerve.
The clinician looks for:
- Microaneurysms
- Retinal haemorrhages
- Hard exudates
- Cotton-wool spots
- Venous abnormalities
- Areas of poor blood supply
- New blood vessels
- Vitreous haemorrhage
- Scar tissue
- Retinal detachment
Dilation may cause temporary blur and light sensitivity. Patients should avoid driving until their vision is sufficiently clear.
Optical Coherence Tomography
Optical coherence tomography, or OCT, creates detailed cross-sectional images of the retina.
It is especially useful for detecting and monitoring:
- Diabetic macular oedema
- Retinal thickening
- Cysts within the retina
- Fluid under the retina
- Vitreomacular traction
- Response to injections or laser
OCT is painless and does not involve radiation.
Fluorescein Angiography
During fluorescein angiography, a fluorescent dye is injected into a vein and retinal photographs are taken as it circulates through the eye.
The test may show:
- Leaking blood vessels
- Areas of blocked retinal circulation
- Abnormal new vessels
- The source of macular leakage
- The extent of retinal ischaemia
Fluorescein angiography is not required for every patient but may assist treatment planning in selected cases.
OCT Angiography
OCT angiography displays retinal blood flow without intravenous dye.
It can demonstrate areas of reduced circulation and abnormal vessels, although it provides different information from fluorescein angiography and does not directly show leakage.
Widefield Retinal Imaging
Widefield retinal photography captures a broad area of the retina and may help document:
- Peripheral haemorrhages
- New blood vessels
- Laser scars
- Retinal ischaemia
- Treatment response
It complements but does not always replace a dilated clinical examination.
Can Diabetic Retinopathy Be Prevented?
Not every case can be prevented, but the risk of developing or progressing to sight-threatening disease can be substantially reduced.
Control Blood Glucose
Long-term blood-glucose control is one of the most important ways to reduce retinal damage.
Work with your diabetes-care team to establish an individual HbA1c target rather than adopting a universal number without considering:
- Age
- Duration of diabetes
- Risk of low blood sugar
- Pregnancy
- Kidney disease
- Cardiovascular health
- Other medical factors
Meeting an appropriate personalised target reduces the risk of diabetic microvascular complications.
Avoid Overly Rapid Changes Without Appropriate Monitoring
Improving glucose control is beneficial.
However, a rapid large reduction in HbA1c may occasionally be associated with temporary early worsening of existing retinopathy, particularly in patients with previously poor control and advanced retinal disease.
This is not a reason to leave diabetes uncontrolled. It means that major treatment intensification should be coordinated with the diabetes team and eye monitoring when significant retinopathy is already present.
Control Blood Pressure
High blood pressure increases stress on already damaged retinal vessels.
Good blood-pressure control reduces the risk of both systemic and ocular complications.
Manage Cholesterol and Kidney Disease
High cholesterol may be associated with retinal lipid leakage and hard exudates.
Kidney disease and diabetic retinopathy often coexist because both reflect damage to small blood vessels.
Managing cholesterol, kidney function and cardiovascular risk forms part of comprehensive diabetic care.
Stop Smoking
Smoking damages blood vessels and increases cardiovascular risk.
Stopping smoking benefits the eyes, heart, brain and kidneys.
Attend Screening Even When Vision Is Clear
Waiting for blur is one of the most dangerous approaches to diabetic eye disease.
Treatment is often most effective before severe visual loss occurs.
How Is Diabetic Retinopathy Treated?
Treatment depends on:
- Retinopathy stage
- Presence of macular oedema
- Visual acuity
- OCT findings
- Retinal ischaemia
- Abnormal new vessels
- Vitreous haemorrhage
- Tractional retinal detachment
- Medical control
- Ability to attend follow-up
Observation and Medical Control
Mild or moderate retinopathy without sight-threatening findings may not require immediate ocular treatment.
Management may involve:
- Better glucose control
- Blood-pressure and lipid management
- Regular retinal photography
- OCT where appropriate
- Closer ophthalmic monitoring
Observation does not mean that the condition is unimportant. It means that treatment risks currently outweigh the expected benefit and that careful follow-up is required.
Anti-VEGF Eye Injections
Vascular endothelial growth factor, or VEGF, promotes blood-vessel leakage and abnormal new-vessel growth.
Anti-VEGF medication is injected into the vitreous cavity after the eye has been cleaned and anaesthetised.
It may be used to treat:
- Centre-involving diabetic macular oedema
- Proliferative diabetic retinopathy
- New vessels affecting the iris or drainage angle
- Selected cases before or after retinal surgery
Anti-VEGF injections can reduce macular fluid, stabilise vision and improve vision in many patients with DME. They can also cause proliferative new vessels to regress.
How Many Injections Are Needed?
There is no fixed number for every patient.
Treatment commonly begins with closer-spaced injections, followed by an individualised schedule according to:
- Visual acuity
- OCT fluid
- Retinal thickness
- Response to treatment
- Recurrence
- The medication used
Some patients require injections for months or years.
Regular attendance is particularly important when anti-VEGF injections are used to control proliferative retinopathy. If treatment is interrupted for a prolonged period, abnormal vessels may reactivate and cause bleeding or retinal detachment.
Steroid Treatment
Corticosteroid injections or implants may reduce diabetic macular oedema in selected patients.
They may be considered when:
- Anti-VEGF response is incomplete
- Injection frequency is difficult to sustain
- The eye has undergone cataract surgery
- Other clinical factors favour steroid treatment
Possible complications include:
- Cataract progression
- Raised eye pressure
- Glaucoma
- Infection following injection
Patients require monitoring of eye pressure and the natural lens.
Panretinal Photocoagulation
Panretinal photocoagulation, or PRP, is laser treatment applied to the peripheral retina.
The laser reduces the retinal drive for abnormal new-vessel growth and lowers the risk of severe visual loss from proliferative retinopathy.
PRP does not directly improve central vision. Its primary purpose is to reduce the risk of:
- Vitreous haemorrhage
- Progressive new-vessel growth
- Tractional retinal detachment
- Neovascular glaucoma
Possible effects include:
- Reduced peripheral vision
- Reduced night vision
- Temporary blur
- Increased macular swelling in some eyes
Despite these limitations, PRP remains an established and durable treatment for proliferative diabetic retinopathy.
Macular Laser
Focal or grid laser may be used in selected cases of diabetic macular oedema.
It is used less often as primary treatment for centre-involving DME because anti-VEGF injections generally provide better visual outcomes in appropriate patients.
Laser may still have a role when:
- Leakage lies outside the centre of the macula
- Oedema is non-centre-involving
- Particular leaking microaneurysms are present
- It is used alongside injections
Vitrectomy Surgery
Vitrectomy removes the vitreous gel and allows the retinal surgeon to treat advanced complications.
It may be required for:
- Non-clearing vitreous haemorrhage
- Tractional retinal detachment
- Scar tissue threatening the macula
- Combined tractional and rhegmatogenous detachment
- Severe proliferative disease
- Selected cases of traction-associated macular oedema
During surgery, the surgeon may:
- Remove blood and vitreous
- Peel scar tissue
- Release retinal traction
- Apply retinal laser
- Drain retinal fluid
- Insert gas or silicone oil when required
Vitrectomy may clear the visual axis and reattach the retina, but recovery depends on the condition of the macula, duration of detachment and degree of retinal ischaemia.
Does Treatment Restore Lost Vision?
Treatment is often highly effective at preventing further loss, but it cannot always restore retinal tissue already permanently damaged.
Visual recovery depends on:
- How early disease was detected
- Duration of macular oedema
- Degree of retinal ischaemia
- Previous bleeding
- Presence of scar tissue
- Whether the macula detached
- Other eye conditions
This is why screening before symptoms begin is so important.
Diabetes and Pregnancy
Pregnancy can accelerate diabetic retinopathy in women who already have type 1 or type 2 diabetes.
Women with pre-existing diabetes who are planning pregnancy should ideally have a comprehensive eye examination before conception. Otherwise, assessment should be arranged early in the first trimester.
Follow-up during pregnancy and for up to one year after delivery depends on the baseline retinal findings and severity.
Rapid improvement in glucose control during early pregnancy may also be associated with temporary retinopathy worsening, so diabetes treatment and retinal monitoring should be coordinated.
Women who develop gestational diabetes alone generally do not require the same diabetic-retinopathy screening pathway during pregnancy unless there is evidence that diabetes predated pregnancy or persists afterwards.
Can Cataract Surgery Be Performed in Patients with Diabetic Retinopathy?
Yes.
Cataracts are common in people with diabetes and may develop earlier.
Before cataract surgery, the ophthalmologist should assess:
- Retinopathy severity
- Macular OCT
- Existing macular oedema
- Blood-glucose stability
- Previous laser or injections
- Likely visual potential
Significant macular oedema or active proliferative disease may need treatment before or around the time of cataract surgery.
Cataract surgery removes lens-related blur but cannot restore vision already limited by macular or optic-nerve damage.
What Should I Do If My Screening Photograph Is Abnormal?
An abnormal screening result does not necessarily mean that treatment is immediately required.
It means that a more detailed assessment may be needed.
The next appointment may include:
- Dilated retinal examination
- OCT
- Additional photography
- Angiography
- Discussion of medical control
- A personalised review interval
- Treatment where sight-threatening disease is present
Do not miss the referral simply because your vision remains clear.
Warning Signs Requiring Prompt Assessment
Seek prompt ophthalmic care if you develop:
- Sudden blurred or reduced vision
- New dark floaters or cobwebs
- A sudden shower of black dots
- A shadow or curtain in the vision
- New distortion
- A painful red eye
- Marked light sensitivity
- Sudden loss of part of the visual field
- Rapid worsening after an eye injection or surgery
After an intravitreal injection, increasing pain, worsening redness, marked light sensitivity or declining vision may indicate infection inside the eye and requires urgent review.
Frequently Asked Questions
Can I have diabetic retinopathy with good vision?
Yes.
Early and sometimes moderately advanced retinopathy may cause no noticeable visual symptoms.
Does a normal eye chart result mean my retina is healthy?
No.
Visual acuity primarily measures central detail. Peripheral diabetic changes may be present while central vision remains normal.
Can diabetic retinopathy be reversed?
Some retinal changes, fluid and abnormal vessels may improve with better medical control and eye treatment.
However, longstanding retinal ischaemia, atrophy and scar damage may be permanent.
Will better diabetes control remove existing retinopathy?
Good control can slow progression and reduce future risk, but it may not make all established retinal abnormalities disappear.
Do I need an eye examination if my HbA1c is good?
Yes.
Good glucose control reduces risk but does not exclude diabetic retinopathy.
Is diabetic retinal photography painful?
No.
A camera photographs the back of the eye. Dilating drops may sometimes be used and can temporarily cause blur and light sensitivity.
Is retinal photography enough?
It is an effective screening method when validated protocols are used. An ophthalmologist’s assessment is still needed when images are abnormal, unclear or when symptoms or other eye conditions are present.
Are injections painful?
Anaesthetic drops are used. Most patients experience pressure or brief discomfort rather than significant sharp pain.
Will I need injections forever?
Not necessarily.
The duration varies according to disease activity and response. Some patients require long-term intermittent treatment, while others become stable after an initial course.
Can laser make me blind?
Retinal laser has possible side effects, particularly involving peripheral and night vision, but it is used because untreated proliferative retinopathy carries a much greater risk of severe blindness.
Can diabetic retinopathy return after laser or injections?
Yes.
Treatment controls the disease but does not cure diabetes or permanently remove the risk. Continued systemic control and retinal monitoring remain essential.
Can diabetes cause other eye problems?
Yes.
People with diabetes are also at increased risk of:
- Cataracts
- Glaucoma
- Temporary refractive changes
- Cranial nerve palsies
- Retinal vascular occlusions
- Ocular-surface disease
The Bottom Line
Diabetic retinopathy is damage to the retinal blood vessels caused by diabetes.
It may remain completely silent until vision is threatened.
The main stages are:
- Non-proliferative diabetic retinopathy, where retinal vessels leak, bleed or close
- Proliferative diabetic retinopathy, where fragile new vessels grow
- Diabetic macular oedema, where fluid accumulates in the central retina
Protecting vision requires:
- Regular retinal screening
- Good blood-glucose control
- Blood-pressure and cholesterol management
- Prompt referral when screening is abnormal
- Timely injections, laser or surgery when required
Patients with type 1 diabetes should generally begin comprehensive eye screening within five years of onset. Patients with type 2 diabetes should be assessed at diagnosis.
Do not wait for blurred vision. Diabetic retinopathy is most safely managed when it is found before you can see its effects.
References
- American Diabetes Association Professional Practice Committee. Retinopathy, Neuropathy, and Foot Care: Standards of Care in Diabetes—2026. Diabetes Care. 2026.
- Lim JI, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025.
- National Eye Institute. Diabetic Retinopathy. Updated September 2025.
- HealthHub Singapore. Diabetic Retinal Photography. Reviewed January 2026.
- HealthHub Singapore and Singapore National Eye Centre. Eye Examinations for Eye Diseases.