Author: Dr Val Phua
Estimated reading time: 9–10 minutes
Children’s Eyes Can Change Quickly
Children may not always realise—or know how to explain—that their vision has changed.
A child with blurred distance vision may assume that everyone sees the same way. Younger children may adapt by sitting closer to the television, holding books near their face or relying more heavily on one eye.
Regular eye examinations help detect problems early, when treatment is often most effective. This is particularly important during childhood because clear and balanced vision is needed for normal visual development, learning and coordination.
For children with myopia, follow-up is also necessary to determine whether the eyes are continuing to grow too quickly and whether myopia-control treatment is working.
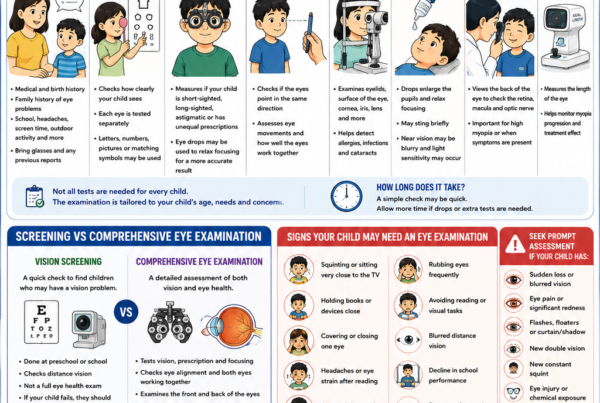
Vision Screening Is Not the Same as a Comprehensive Eye Examination
Vision screening is a useful first step. It may be performed at school, during preschool health checks or as part of a routine medical assessment.
A screening commonly checks whether a child can see letters or symbols at a specified distance. However, it is not a complete examination of the eyes.
A comprehensive eye examination may assess:
- Vision in each eye separately
- Spectacle prescription
- Eye alignment
- Focusing ability
- Eye movements
- Binocular vision
- Corneal and lens health
- Retina and optic nerve
- Axial length, when relevant to myopia management
In Singapore, school vision screening primarily looks for myopia and may not detect every eye condition. A child should therefore have a comprehensive assessment whenever there are symptoms, abnormal findings or parental concerns. [1]
How Often Should Children with No Known Eye Problems Be Checked?
There is no single schedule that applies to every child, but the following provides a practical guide.
Babies and Toddlers
A newborn’s eyes should be assessed as part of routine paediatric care.
Further evaluation is needed if there are concerns such as:
- An abnormal red reflex
- A constant squint
- Drooping of an eyelid
- Persistent tearing
- An unusually large or cloudy eye
- Poor visual attention
- A family history of significant childhood eye disease
Instrument-based vision screening may also be used in young children who are not yet able to read an eye chart.
Preschool Children
Vision should be assessed during the preschool years, ideally before the child begins formal schooling.
This is an important period for detecting:
- Refractive errors
- Squint
- Amblyopia or “lazy eye”
- Unequal vision between the eyes
Children who fail screening or cannot complete the test reliably should undergo a comprehensive eye examination rather than simply waiting for the next school screening.
Children Aged Five Years and Above
For children with no symptoms and normal screening results, vision screening every one to two years is generally reasonable. [2]
An earlier comprehensive examination should be arranged if:
- Vision changes
- School performance is affected
- The child experiences headaches or eye strain
- There is a strong family history of myopia or other eye disease
- A parent, teacher or doctor has concerns
How Often Should a Child with Myopia Be Reviewed?
A child with established myopia should generally have an eye examination at least once a year.
In Singapore, children with myopia are commonly monitored every six to twelve months, depending on their age, prescription and rate of progression. [3]
A six-month review is particularly helpful because childhood myopia may change significantly within a year, especially when it begins at a young age.
Follow-up may be more frequent when:
- Myopia is progressing rapidly
- The child is young
- One or both parents have high myopia
- The spectacle prescription has changed substantially
- Axial length is increasing quickly
- Treatment has recently started or changed
- The child has high myopia
How Often Should Children Receiving Myopia-Control Treatment Be Reviewed?
Children undergoing myopia control generally require closer monitoring than children wearing ordinary single-vision spectacles.
A common clinical schedule is:
- A baseline examination before treatment
- An early review after treatment begins, where appropriate
- Follow-up every three to six months during the initial treatment period
- Six-monthly reviews once treatment and vision are stable
The precise schedule depends on the treatment used and the child’s response.
The purpose of these reviews is to determine whether treatment is:
- Being used correctly
- Well tolerated
- Providing clear vision
- Slowing refractive progression
- Slowing axial eye growth
- Still appropriate for the child
Treatment may need to be changed, strengthened or combined with another option if progression remains inadequately controlled.
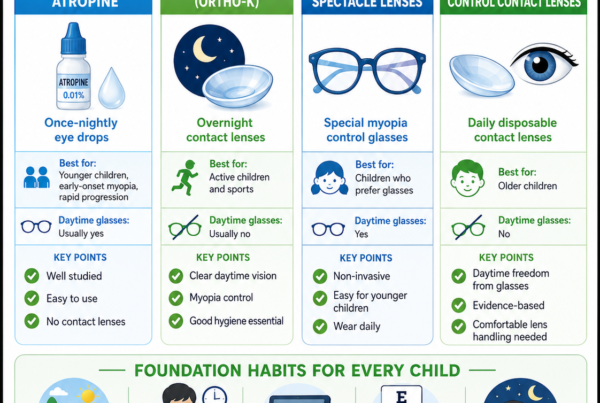
Follow-Up for Low-Dose Atropine
A child starting atropine may be reviewed within the first few months to assess:
- Light sensitivity
- Near-vision symptoms
- Allergic reactions
- Treatment adherence
- Changes in refraction
- Changes in axial length, where available
Once stable, reviews are commonly scheduled approximately every six months.
Atropine is usually continued while the child’s myopia remains active. It should not be stopped without appropriate monitoring, as some children may experience faster progression after treatment is withdrawn.
Follow-Up for Orthokeratology
Orthokeratology requires several early visits because the lens fit, corneal response and visual correction must be checked carefully.
The initial review schedule may include assessments:
- Soon after the first night or first few nights of wear
- After approximately one week
- After several weeks
- At three months
- Every three to six months thereafter
The exact schedule varies according to the practitioner and the child’s progress.
At each visit, the clinician may assess:
- Unaided vision
- Lens fit
- Corneal topography
- Corneal health
- Lens cleanliness
- Hygiene technique
- Myopia progression
Children wearing Ortho-K lenses should not wait for a routine appointment if they develop pain, redness, light sensitivity, discharge or reduced vision.
Follow-Up for Defocus Spectacle Lenses
Children wearing defocus or myopia-control spectacle lenses are often reviewed every six months.
The examination may include:
- Visual acuity
- Updated refraction
- Spectacle fit and lens positioning
- Wearing compliance
- Axial length, where available
- Assessment of myopia progression
The frame should fit properly so that the child looks through the intended optical zones of the lens.
Follow-Up for Soft Myopia-Control Contact Lenses
Children using soft myopia-control contact lenses require reviews to assess both myopia progression and contact-lens safety.
Follow-up commonly includes:
- An early fitting review
- A check after the child has adapted to lens wear
- Reviews every three to six months
The clinician will assess:
- Corneal health
- Lens fit
- Vision quality
- Wearing time
- Cleaning and handling
- Myopia progression
Poor hygiene, sleeping in lenses or exposing lenses to water increases the risk of infection and should be addressed promptly.
What Should Be Checked at a Myopia Review?
A myopia review should involve more than simply asking whether the child can still see through the glasses.
Depending on the child and treatment, it may include:
Visual Acuity
Checks how clearly the child sees at distance and near.
Refraction
Measures whether the spectacle prescription has changed.
Cycloplegic eye drops may be used when a more accurate measurement is needed, particularly in younger children.
Axial Length
Axial length measures the front-to-back length of the eye.
This is useful because myopia is usually associated with elongation of the eyeball. Monitoring axial length can help determine whether treatment is slowing structural eye growth, even when changes in spectacle power are small.
Eye Alignment and Focusing
Assessment of binocular vision, accommodation and eye alignment may be important if the child experiences headaches, eye strain or double vision.
Eye-Health Examination
The front and back of the eyes should be examined as appropriate.
Children with high myopia may require a dilated retinal examination at least annually because of their higher risk of retinal complications. [4]
When Should a Child Be Seen Earlier?
Do not wait for the next routine review if the child develops:
- Sudden blurred or reduced vision
- Eye pain
- Persistent redness
- Light sensitivity
- New double vision
- A new or worsening squint
- Flashes or floaters
- A shadow or curtain in the vision
- A white or cloudy appearance in the pupil
- Headaches associated with visual symptoms
- Contact-lens discomfort that does not resolve after removing the lens
Children receiving Ortho-K or soft contact-lens treatment should be assessed promptly if an eye becomes painful, red or sensitive to light.
Signs That a Routine Appointment Should Be Brought Forward
Parents and teachers should watch for:
- Squinting to see distant objects
- Sitting close to the television
- Moving nearer to the classroom board
- Holding books or devices very close
- Closing or covering one eye
- Frequent eye rubbing
- Headaches after reading
- Avoiding reading or visually demanding tasks
- Frequent changes in spectacle prescription
- A decline in school performance
These behaviours do not always indicate myopia, but they warrant an eye assessment.
Is School Vision Screening Enough?
School screening is valuable but should not be viewed as a substitute for comprehensive eye care.
A screening may:
- Detect reduced distance vision
- Identify many children who require spectacles
- Prompt referral for further assessment
However, it may not fully assess:
- Eye alignment
- Amblyopia
- Eye health
- Peripheral retinal disease
- Focusing or binocular-vision problems
- The rate of axial eye growth
Parents should arrange a comprehensive examination when symptoms are present, even if the child previously passed school screening.
Frequently Asked Questions
My child’s glasses still seem clear. Is a review necessary?
Yes.
Children may compensate for mild changes, and myopia may progress before they complain. A review also checks eye health, spectacle fit and whether progression is adequately controlled.
Is an annual review enough for every myopic child?
Not always.
Annual review may be sufficient for selected stable children, but six-monthly assessment is often more appropriate for younger children, progressing myopia or children receiving treatment.
Does my child need axial-length measurements?
Axial-length monitoring can provide useful information about eye growth, especially during myopia-control treatment. However, availability varies and clinical decisions may also be based on refraction, age, risk factors and treatment response.
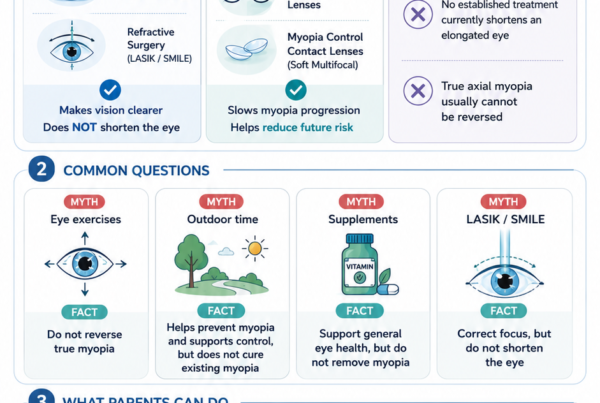
When can myopia-control treatment be stopped?
Treatment is usually continued until progression has slowed or stabilised, often during the later teenage years. The decision should be individualised, and closer monitoring may be recommended after stopping treatment.
Should siblings also be examined?
Yes, particularly when there is a family history of myopia. A sibling may have blurred vision without recognising or reporting it.
A Practical Follow-Up Guide
| Child’s situation | Suggested interval |
|---|---|
| No symptoms and normal screening | Vision screening every 1–2 years after age five |
| Myopia wearing ordinary spectacles | Every 6–12 months |
| Newly diagnosed or rapidly progressing myopia | Approximately every 3–6 months |
| Receiving atropine or defocus spectacles | Commonly every 6 months once stable |
| Ortho-K or soft contact-lens treatment | Early fitting checks, then every 3–6 months |
| High myopia | At least annual dilated retinal assessment, or as advised |
| New pain, redness or sudden visual change | Urgent assessment—do not wait |
These intervals are general guides. The treating eye-care professional may recommend a different schedule based on the child’s age, eye health, treatment and rate of progression.
The Bottom Line
Children’s eyes can change quickly, particularly during the primary-school years.
Children with no known eye problems should receive regular age-appropriate vision screening. Children with myopia should generally be reviewed every six to twelve months, while those with rapid progression or receiving active myopia-control treatment may require assessment every three to six months.
Regular reviews allow changes to be detected early, help determine whether treatment is working and provide an opportunity to reinforce healthy visual habits.
The right review schedule is not simply based on age—it should reflect the individual child’s vision, eye growth, risk factors and treatment needs.
References
- Health Promotion Board, Singapore. Health Screening for Primary School: Vision Screening.
- American Association for Pediatric Ophthalmology and Strabismus. Vision Screening Guidelines.
- Singapore National Eye Centre. Childhood Myopia: Diagnosis, Monitoring and Treatment.
- International Myopia Institute. IMI Clinical Management Myopia Guidelines Report.
- American Association for Pediatric Ophthalmology and Strabismus. Myopia and Treatment of Myopia in Children.
- American Academy of Ophthalmology. Vision Screening for Infants and Children.